


Meniscus Tear Rehab 101

Anatomy & Role of a Meniscus
Each knee has two menisci, a lateral and medial, which are situated between the femur (thigh bone) and tibia (shine bone). They are anchored to the bone via ligamentous attachments including the medial collateral ligament (MCL), horn attachments at the posterior and anterior horn, the transverse ligament and the meniscofemoral ligaments (known as Wrisberg & Humphrey). Anatomical studies have shown us that much like rest of our body everyone has variances to the shape of their menisci. Fun Fact: 100% of people have at least one of the meniscofemoral ligaments but only 46% have both. Although both menisci are a semi-lunar wedge shape, the lateral has greater variances in the width, thickness and shape.
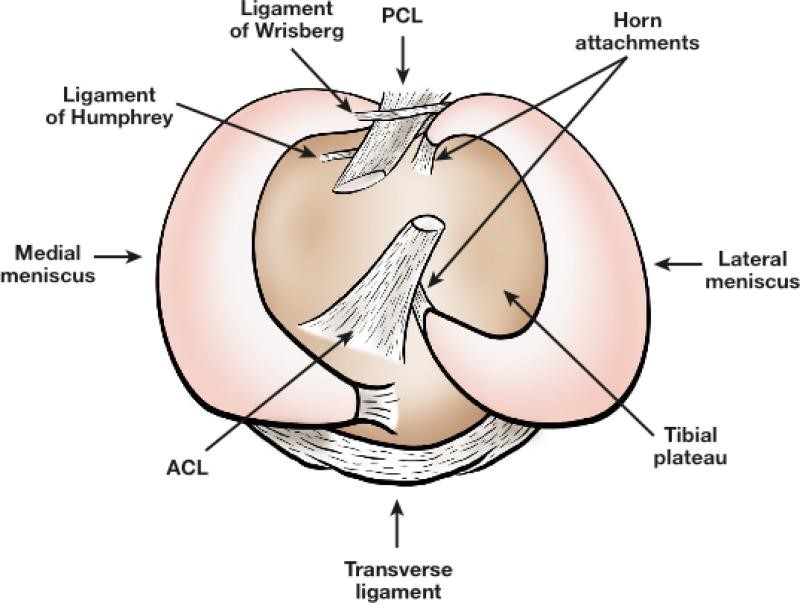
Image: Birdseye view looking down to the menisci on top of the tibia with associated ligaments.
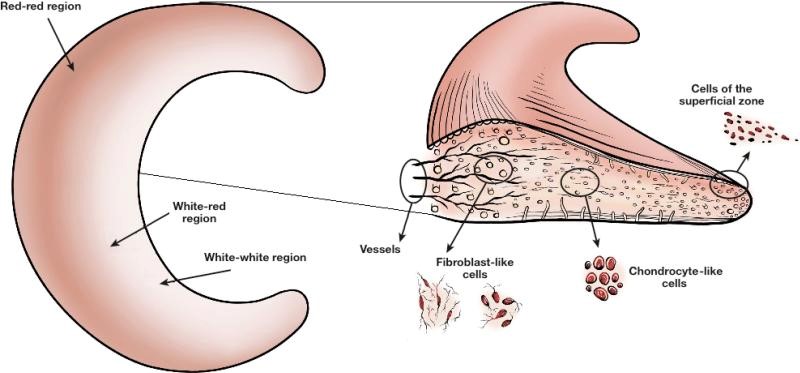
The meniscus has full vascularisation at birth but this decreases with age. Eventually by full maturation, only the outer zone of the meniscus has a full blood supply and the inner most part (known as the white-white zone) has no blood supply. The amount of blood supply dictates the healing capacity and therefor the inner white zone is susceptible to poor healing and permanent damage following trauma or degeneration. It also helps dictate surgical success (read more about that HERE>>).
I can still recall one of my first year university lecturers preaching about meniscus biomechanics and he was adamant that these are ‘shock distributors’ not ‘shock absorbers’ – they spread the force not absorb it – that’s a subtle distinction but it has always stuck in my head as to how a meniscus works and why it is important. It’s about the spread of force between the tibia and femur (see diagram below). Paletta et. al. found that total removal of the meniscus increases contact force by 235-335% and another research group found that even a partial meniscectomy increased load through the articular cartilage by >350% (7). Over time that’s a substantial amount of added force being point loaded.
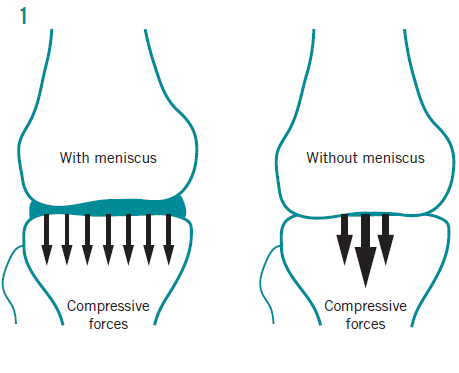
Image: Diagram displaying the changes in joint forces within the knee with & without the meniscus
Risk Factors for Tears
In 2013 a systematic review and meta-analysis (10) was published that identified the biggest risk factors for a meniscal injury. Please note these are not the only ways tears occur, just what is known from the evidence. They found the following:
Degenerative Tears
- older age (> 60 years) [strong evidence]
- being male (3x more likely) [strong evidence]
- work-related kneeling and squatting (>1 hour per day) [strong evidence]
- climbing stairs (>30 flights per day for 12 months) [strong evidence]
- higher BMI (greater than 25 kg/m2) [moderate evidence]
- standing (>2 hrs per day) [moderate evidence]
- walking (>3.2km per day for 12 months) [moderate evidence]
- lifting or carrying heavy weights (greater than 10 kg-50 kg) [moderate evidence]
The authors also found strong evidence to suggest that sitting longer than 2 hours per day was protective of degenerative meniscal tears. There was also minimal or no evidence that driving, smoking, and alcohol consumption were associated with the incidence of degenerative meniscal tears.
Acute Tears
- playing rugby or soccer [strong evidence]
- weight bearing during trauma [moderate evidence]
- swimming and other sports [moderate evidence]
- running has minimal evidence as a risk factor
Tear Due to Knee Laxity
- greater than 12months between ACL injury and reconstruction (medial meniscus only) [strong evidence]
- systemic joint laxity (Beighton score >1) [moderate evidence]
Diagnosing a Meniscus Tear
Mechanism of Injury
Traumatic tears generally occur with a twisting injury to the knee, usually when it is bent and loaded with bodyweight. Think of cutting or twisting movements where the foot is planted on the ground (especially common in sports like rugby, soccer, skiing, basketball). A shearing force occurs on the meniscus that it more than the tissue can withstand and leads to tearing of the cartilage structure. Traumatic tears may also appear in the older population with only a small trauma or load applied to the meniscus, for example, a small twisting movement when working in the garden.
Degenerative (non-traumatic) tears occur in the absence of any obvious event or moment. This is due to the fact the knee has undergone some age-related changes and the meniscus has somewhat weakened. Day-to-day normal forces may cause some tearing to the meniscus which becomes symptomatic (pain, swelling, loss of range of motion). This may represent the early stages of knee osteoarthritis (16) and therefore makes sense these tears are mostly seen in middle-to-older aged people.
Physical Exam & History
Pain: pain will likely feel more medial or lateral depending on the meniscus that is injured. It will generally be reported close to the joint line. Pain may occur with weightbearing, exercise and deep knee bending however is not limited to these. A “pop” noise or sensation may have occurred at time of injury.
Swelling: following an isolated traumatic meniscus tear a small amount of swelling is likely to develop over the following 24-48 hours due to the low vascularisation of the meniscus. Immediate large volume swelling suggests injury to another structure. Swelling continually developing post exercise may also allude to a chronic meniscus injury (2). A Sweep Test is a simple test for determining the presence intra-articular swelling.
Mechanical Symptoms: patients may report locking, clicking or catching in the knee joint which can result from displaced flaps of tears. They may also report feelings of instability within the knee.
Range of Motion: often there will be a loss of knee extension and it may be painful for the knee to be held passively in extension. Pain may also occur with deep knee flexion compressing the meniscus.
Knee Joint Line Tenderness: palpation of the joint line with the knee bent at 90° generally caused pain. It has been shown that pain with joint line palpation can be quite accurate in the diagnosis of meniscus tears (3).
Special Knee Tests: There is a multitude of special tests that have been developed to attempt to accurately diagnose meniscus tears. Reproduction of pain with these tests increases likelihood of a meniscus injury but are often not perfect when used in isolation and using multiple tests paired with the clinical history appears to be most accurate (2). These tests are listed in the table below.
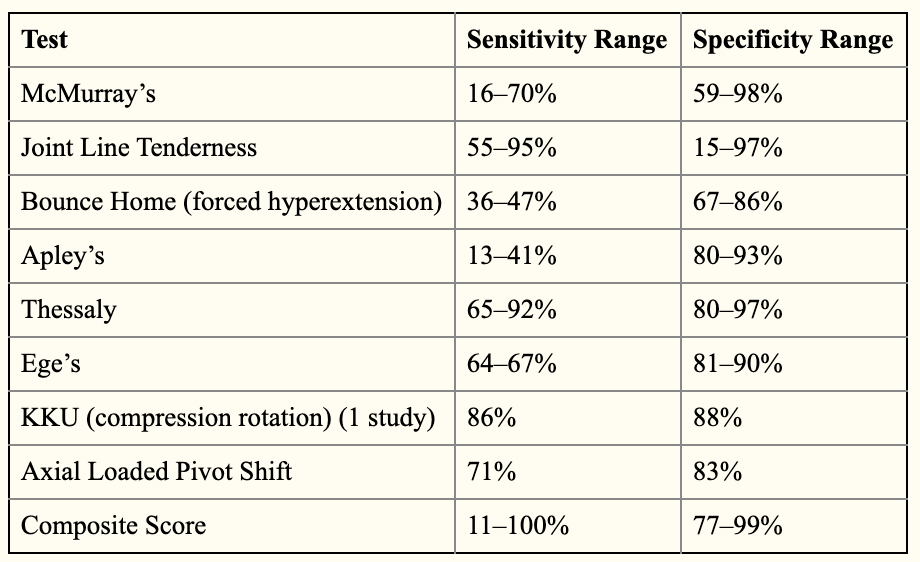
Image: accuracy of the special knee tests taken from Chivers et. al 2009
Additionally, a Lachman’s or Anterior Drawer test can be used to investigate the integrity of the Anterior Cruciate Ligament. Whilst not a test for the meniscus they may still be provocative of symptoms however they have value in helping to rule out concomitant ACL injuries or anterior laxity of the knee which can increase likelihood of meniscus tears.
Medical Imaging
As the meniscus is located within the knee joint, x-rays and ultrasound imaging are not helpful in the diagnosis of a meniscus injury. MRI is required to visualise a meniscus on imaging however it is often not needed unless there is concern of concomitant injury or other factors such as malignancy or infection. Recent studies have shown that approximately 10-30% of people without any knee pain at all will have a meniscus tear on MRI imaging (14,15). So scans need to be interpreted carefully with the patients history and physical assessment results.
Physiotherapy
Initial Symptom Management
The initial stages can be summed up nicely into the P.O.L.I.C.E acronym 👮🏻♂️🚨, this is the modern replacement of the age old favourite R.I.C.E. The new acronym stands for:
- P (Protect) – this means prevention of any further damage but not necessarily completely resting the area. Still actively engaging in daily activities but with guidance from your physio or doctor about what to avoid. It may mean the use of crutches.
- L (Optimal Load) – the right amount of loading or activity can help facilitate recovery and prevent muscle atrophy and weakness associated with complete rest. Some light isometric strength work in a non-weightbearing position can be of use very early on.
- C.E (Ice, Compression, Elevation) – these three are to help alleviate swelling and pain. These can be helpful early on but contemporary research has discovered the inflammatory process is an important part of healing, I wouldn’t place too much importance on these. Cryotherapy (or cold therapy) is effective at both swelling management and reducing pain signals from the brain. The I.C.E components become more important if swelling is causing loss of joint range of motion or preventing rehabilitation exercises.
Exercise & Progressive Load
This is the cornerstone of successful meniscal injury rehab. Targeted lower limb exercise has been shown time and time again (17,18,19) to be just as effective as surgical intervention for meniscal injuries. The following is a list of exercises that can be used for meniscus rehab, ideally we want to increase strength of the whole lower limb whilst addressing issues of knee positioning and landing mechanics. Specifics on repetitions and sets should be prescribed individually to you by your physio and not given as a ‘recipe’ approach. This is not an exhaustive list.
Isometrics: these can be very helpful early on when the patient may have pain through knee range of motion. By fixing the angle, we still work the muscles without stirring up symptoms. These exercises focus on quadriceps strength & activation as we know knee pain will effect quadriceps activation (5).
- Wall sit
- Alternating Leg Wall Sit (3 seconds per leg)



Image: normal wall sit (left), alternating leg wall sit (right)
Glutes: whilst the glutes aren’t located near the knee they do play an important role. The 3 gluteus muscles (maximus, medius & minimus) act to abduct and externally rotate the femur (thigh bone). This movement directly affects knee positioning therefor weak gluteal muscles can contribute to knee valgus which is a knee position that increases injury risk (11).
- Standing Hip Abductions
- Monster walks >>click HERE to see monster walks exercise<<


Image: standing hip abduction performed with cable machine (left) or resistance band (right)
Hip Adductors: these are the often neglected inner thigh muscles
- Banded Hip Adduction
- Copenhagen Plank
- These can be intense on the knee. Start with the knee supported version (far left, below) and progress to the full plank (middle, below).



Image: half Copenhagen (left), full Copenhagen (middle), banded adduction (right)
Calves: no knee rehab program is complete without calf muscle exercises, especially for the soleus, the deeper calf muscle. Research has shown that the soleus plays just as an important role in preventing shear force on the knee when landing as the hamstring do (8).
- Soleus Wall Sits
- Start with both feet on floor and progress to single leg (far right, below)
Soleus Raise (smith machine)
- aiming to build strength to achieve on 8 reps of your own body weight on the bar with a single leg
- Standing Calf Raise



Image: soleus raise on the smith machine (left), standing calf raise (middle), single leg soleus wall hold (right)
Single Leg Work: I like to implement single leg work as soon as possible. Side to side discrepancies are easily highlighted when on one limb, it also throws in a component of balance. It makes sense since these injuries generally happen when the person is on one leg.
- Bulgarian Split Squats
- Resistance Band Lunges (exercise 1 in the below Instagram post)
- Banded Single leg Reverse Squats (exercise 2 in the below Instagram post)

Image: Bulgarian split squat
Landing & Jumping: dynamic jumping and landing work should be reserved for when the patient has progressed through their rehab and is able to withstand the impact loading without causing pain or swelling.
- Jump lunge landing (exercise 3 in the above Instagram post)
- Depth jump landing (exercise 4 in the above Instagram post)
- Single leg box jump

Image: Single leg box jump
Patient Education
Empowering the patient with knowledge about their injury is an important part of rehabilitation. Research has shown that when the patient knows and understands their injury and recovery process, they generally have more favourable outcomes, better compliance to rehab program as well as less anxiety and depression.
Other Conservative Treatment Options
Medication: Pain relief medication such as paracetamol, ibuprofen or GP-prescribed NSAIDs may be helpful in pain management.
Corticosteroid Injections: Cortisone shots are injections that can help relieve pain and inflammation in a specific area or joint. A 2013 study showed that arthroscopic debridement was only marginally better than corticosteroid injections in degenerative meniscus tears (12). This may be a viable option.
Platelet Rich Plasma (PRP): PRP has hid mixed results in the literature for meniscal lesion healing. Some studies show no effect (4) whilst others are promising (6,13). I will dedicate another blog to discussing the evidence for PRP knee injections.
Surgical Options
I’ve recently written an extensive blog covering this topic titled “Meniscus Tear: Do I need Surgery?”, read it HERE>>. In that blog I take a deep dive into the surgical options and what current body of scientific evidence is telling us about meniscal tear surgeries.
Recent studies have really put the brakes on the idea that meniscus injuries need surgery. Multiple studies have emerged in the last decade where comparison was made between meniscal ‘clean-up’ surgeries (a.k.a partial meniscectomy) and sham surgeries. Both groups of patients were taken into the operating theatre, had incisions made, instruments inserted, given walking and aids and followed the same rehab procedures. The only difference between groups was that one had part of their torn meniscus removed and the other didn’t. So what did they find? There was no difference in outcomes between groups at 1 or 2 years follow-up (1,9). Yep that’s right, fake surgery worked just as well as real surgery…let that sink in.
There may be more value in meniscal surgery in the younger active populations or when there is symptoms such as a locking knee, recurrent pain or failure with conservative management over a 3-6 month period.
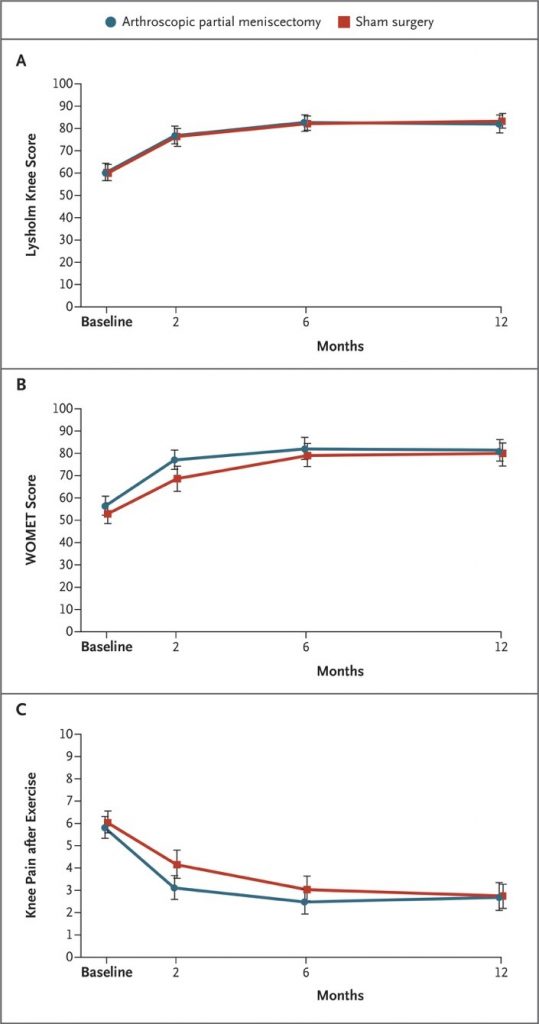
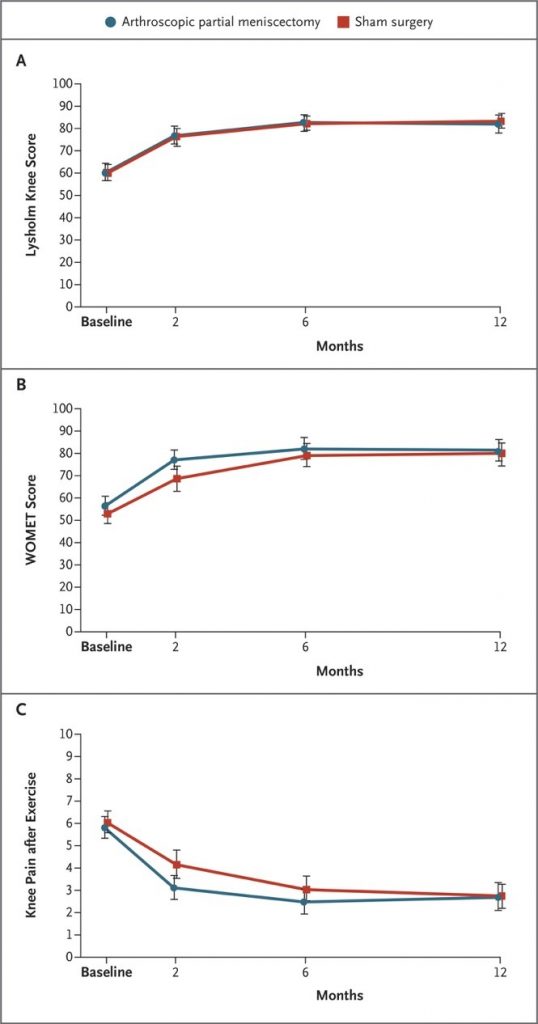
Image: graphs from Sihvonen et. al showing almost no different in both a validated outcome measure (left) and pain after exercise (right) when comparing sham surgery to the real deal
Related Resources
Listen to episode #86 of The Physical Performance Show to hear Gold Coast knee surgeon Dr Chris Vertullo discuss meniscus injuries
Additional Blogs on this topic:
Mensicus Tear – Do I need Surgery?
Why your Meniscus Tear might be normal

James Gardiner
POGO Physiotherapist
Book an Appointment with James here.
Featured in the Top 50 Physical Therapy Blog
References
- Sihvonen R, Paavola M, Malmivaara A The FIDELITY (Finnish Degenerative Meniscal Lesion Study) Investigators, et alArthroscopic partial meniscectomy versus placebo surgery for a degenerative meniscus tear: a 2-year follow-up of the randomised controlled trialAnnals of the Rheumatic Diseases 2018;77:188-195.
- Chivers, M. D., & Howitt, S. D. (2009). Anatomy and physical examination of the knee menisci: a narrative review of the orthopedic literature. The Journal of the Canadian Chiropractic Association, 53(4).
- Eren, O. T. (2003). The accuracy of joint line tenderness by physical examination in the diagnosis of meniscal tears. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 19(8), 850-854. https://doi.org/10.1016/s0749-8063(03)00736-9
- Griffin, J. W., Hadeed, M. M., Werner, B. C., Diduch, D. R., Carson, E. W., & Miller, M. D. (2015). Platelet-rich plasma in Meniscal repair: Does augmentation improve surgical outcomes? Clinical Orthopaedics and Related Research®, 473(5), 1665-1672. https://doi.org/10.1007/s11999-015-4170-8
- Hart, J. M., Pietrosimone, B., Hertel, J., & Ingersoll, C. D. (2010). Quadriceps activation following knee injuries: A systematic review. Journal of Athletic Training, 45(1), 87-97. https://doi.org/10.4085/1062-6050-45.1.87
- Kaminski, R., Maksymowicz-Wleklik, M., Kulinski, K., Kozar-Kaminska, K., Dabrowska-Thing, A., & Pomianowski, S. (2019). Short-term outcomes of percutaneous Trephination with a platelet rich plasma Intrameniscal injection for the repair of degenerative Meniscal lesions. A prospective, randomized, double-blind, parallel-group, placebo-controlled study. International Journal of Molecular Sciences, 20(4), 856. https://doi.org/10.3390/ijms20040856
- Makris, E. A., Hadidi, P., & Athanasiou, K. A. (2011). The knee meniscus: Structure–function, pathophysiology, current repair techniques, and prospects for regeneration. Biomaterials, 32(30), 7411-7431. https://doi.org/10.1016/j.biomaterials.2011.06.037
- Maniar, N., Schache, A. G., Pizzolato, C., & Opar, D. A. (2020). Muscle contributions to tibiofemoral shear forces and valgus and rotational joint moments during single leg drop landing. Scandinavian Journal of Medicine & Science in Sports. https://doi.org/10.1111/sms.13711
- Sihvonen, R., Paavola, M., Malmivaara, A., Itälä, A., Joukainen, A., Nurmi, H., Kalske, J., & Järvinen, T. L. (2013). Arthroscopic partial meniscectomy versus sham surgery for a degenerative Meniscal tear. New England Journal of Medicine, 369(26), 2515-2524. https://doi.org/10.1056/nejmoa1305189
- Snoeker, B. A., Bakker, E. W., Kegel, C. A., & Lucas, C. (2013). Risk factors for Meniscal tears: A systematic review including meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 43(6), 352-367. https://doi.org/10.2519/jospt.2013.4295
- Tamura, A., Akasaka, K., Otsudo, T., Shiozawa, J., Toda, Y., & Yamada, K. (2017). Dynamic knee valgus alignment influences impact attenuation in the lower extremity during the deceleration phase of a single-leg landing. PLOS ONE, 12(6), e0179810. https://doi.org/10.1371/journal.pone.0179810
- VERMESAN, D., PREJBEANU, R., LAITIN, S., DAMIAN, G., DELEANU, B., ABBINANTE, A., FLACE, P., & CAGIANO, R. (2013). Arthroscopic debridement compared to intra-articular steroids in treating degenerative medial meniscal tears. European Review for Medical and Pharmacological Sciences, 17, 3192-3196.
- Blanke, F., Vavken, P., Haenle, M., Von Wehren, L., Pagenster, G., & Majewski, M. (2015). Percutaneous injections of platelet rich plasma for treatment of intrasubstance meniscal lesions. Muscle Ligaments and Tendons Journal, 05(03), 162. https://doi.org/10.32098/mltj.03.2015.04
- Culvenor, A. G., Øiestad, B. E., Hart, H. F., Stefanik, J. J., Guermazi, A., & Crossley, K. M. (2018). Prevalence of knee osteoarthritis features on magnetic resonance imaging in asymptomatic uninjured adults: A systematic review and meta-analysis. British Journal of Sports Medicine, 53(20), 1268-1278.
- Horga, L. M., Hirschmann, A. C., Henckel, J., Fotiadou, A., Di Laura, A., Torlasco, C., D’Silva, A., Sharma, S., Moon, J. C., & Hart, A. J. (2020). Prevalence of abnormal findings in 230 knees of asymptomatic adults using 3.0 T MRI. Skeletal Radiology
- Herrlin, S., Hållander, M., Wange, P., Weidenhielm, L., & Werner, S. (2007). Arthroscopic or conservative treatment of degenerative medial meniscal tears: A prospective randomised trial. Knee Surgery, Sports Traumatology, Arthroscopy, 15(4), 393-401
- Rogers, M., Dart, S., Odum, S., & Fleischli, J. (2019). A cost-effectiveness analysis of isolated Meniscal repair versus partial meniscectomy for red-red zone, vertical Meniscal tears in the young adult. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 35(12), 3280-3286.
- Lee, D., Park, Y., Kim, H., Nam, D., Park, J., Song, S., & Kang, D. (2018). Arthroscopic meniscal surgery versus conservative management in patients aged 40 years and older: A meta-analysis. Archives of Orthopaedic and Trauma Surgery, 138(12), 1731-1739.
- Khan, M., Evaniew, N., Bedi, A., Ayeni, O. R., & Bhandari, M. (2014). Arthroscopic surgery for degenerative tears of the meniscus: A systematic review and meta-analysis. Canadian Medical Association Journal, 186(14), 1057-1064.






