


Meniscus Tear: Do I need surgery?

Did you know that up to 30% of people can have a meniscus tear without any pain at all? (6). Yet knee pain is really common, and if you’re suffering from it you’re not alone. When I see a patient who’s had a meniscus tear I can always relate, having suffered several tears myself. I still manage to get around fine, stay active and remain mostly pain free. But would it be better to get surgery for these tears? This is probably the same question you’re asking yourself right now so let’s unpack what the science says.

Anatomy of a Tear
Traumatic Meniscus Tear
These types of tears are associated with an event that causes a shearing force to the meniscus beyond its capability to withstand, often when the knee is in flexion and the thigh rotating. Usually the person’s body is rotating and their foot is planted to the ground. There seems to be great variance in pain following a tear, pain may be experienced immediately whilst others feel almost no pain with it appearing later (1). Traumatic tears tend to occur in the young, or older active populations.
Degenerative Meniscus Tear
Many people end up with a meniscus tear without any acute trauma or incident that they are able to pinpoint. This is due to the fact their knee has undergone some age-related changes and the meniscus has somewhat weakened. Day-to-day normal forces may cause some tearing to the meniscus which becomes symptomatic (pain, swelling, loss of range of motion). This may represent the early stages of knee osteoarthritis (5) and therefore makes sense these tears are mostly seen in middle-to-older aged people.
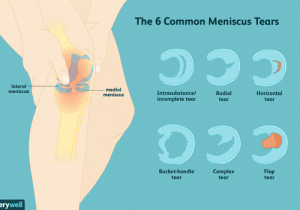
6 common types of meniscus tears & the location of the 2 menisci in the knee joint
Surgical Options
Meniscectomy
A meniscectomy means the removal of either the whole meniscus (total meniscectomy) or just a portion (partial meniscectomy). It’s been well established that the meniscus has its own very important roles in maintaining knee health which include joint force distribution, joint stability, lubrication of the joint and helping maintain nutrition. Removing the meniscus will have detrimental affects to the health of the knee joint. Research has shown that a total meniscectomy leads to point loading, meaning the same force is spread over a smaller area. Peak contact pressure has been shown to increase by 235%. This leads to an increase of osteoarthritis in the knee joint. Over the next 20 years these people are 14 times more likely to suffer knee OA compared to an age and sex matched person with an intact meniscus (15).
Total meniscectomies are generally considered a surgery of the past. A partial meniscectomy aims to retain as much of the normal, non-torn meniscus as possible. In particular the outer rim of the meniscus is maintained as it has the most important biomechanical implications. Despite what appears to be a better option than a total meniscectomy, long term studies still do show degeneration in the knee following a partial removal although it is somewhat delayed (11). One study following patients for 8.5 years showed a significant increase in knee osteoarthritis in the operated knee, increasing to 53% compared to only 22% in the unoperated knee (3). Currently we likely have insufficient information regarding the long-term impacts of a partial meniscectomy on knee OA (17).
Meniscus Repair
Repairing torn menisci has grown in popularity although it may not be suitable for every patient as success is highly dependent on the location of the tear. For a repair to have a chance at healing it must have adequate blood supply. Only tears in the red-red zone or possibly the white-red zone are expected to heal (see diagram below). The rest of the meniscus doesn’t have sufficient blood supply to promote healing. Two systematic reviews (4,12) have compared failure rates between different surgical repair techniques and found that all repair techniques had similar failure rates. A 2019 study showed repair to be more cost effective and improve quality of life over a 40-year modelled period compared to partial meniscectomy (14).
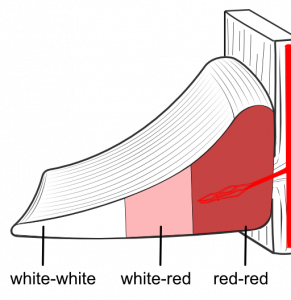
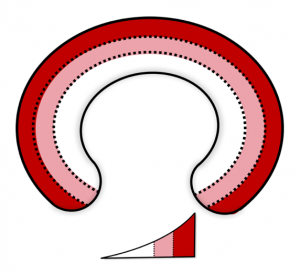
Left; front on view of the meniscus with blood vessel entering from the outer rim. Right; top view of the blood supply zones
Uncommon Surgical Options
Meniscal Reconstruction: these are relatively rare and involve using an allograft (donated) meniscus to replace a partially or totally resected meniscus in an aim to mimic the natural meniscus and restore function (2).
Meniscal Scaffold: a biodegradable scaffold made from either collagen or polyurethane is inserted into the meniscal defect in an aim to allow growth of new meniscal tissue (2).
Surgery – What does the science say?
More than 4 million meniscal debridement’s are performed each year worldwide. Surgeries aren’t without risk and there is potential for complications. The risk of surgery must be weighed against the potential for beneficial results (9).
A growing body of evidence suggests that meniscal surgeries rarely yield better results than physiotherapy and exercise. Three meta-analyses have been conducted into surgery vs conservative management. I’ll summarise them below:
- A 2014 metanalysis found that when meniscal debridement was compared against either sham surgery or conservative management in middle aged patients there was no benefit from surgery. The surgical group had no improvements in pain at 6 or 24 months (9).
- 773 patients results were summarised in a 2016 metanalysis which found that pain and function were slightly improved at 6 months with surgery. However this benefit was lost at any longer follow-ups (14).
- In 2018 another metanalysis came to the conclusion that surgery was no better for knee pain or function in over 1000 patients, concluding that arthroscopic surgery should be reserved for those that fail conservative management. (10)
Now is there any risk that waiting and try physiotherapy will cause more harm? The short answer is not likely. One study which only offered surgery to those who failed conservative treatment found that waiting for surgery didn’t reduce success. 58% of patients were successful with exercise therapy, avoiding the knife (13). Numerous other studies out there (5,16,20) show that 2-3 sessions per week for 8-12 weeks of physiotherapy guided exercise leads to just as good results as an arthroscopic surgery.
Not only have we found that conservative management is at least equal to surgery, we known know the exercise effectively decreases levels of depression and anxiety. This is something that wasn’t achieved in the surgical group. Now this is important as it has been well established that depression and anxiety are contributing factors to the development of persistent pain (19).
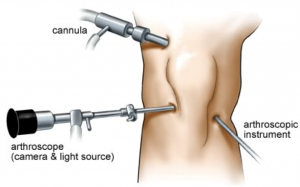
Arthroscopic knee surgery diagram – this is the technique used for meniscal repair.
Conservative Treatment Options (non-operative)
Conservative management can include anything that is considered non-surgical such as rest, ice, activity modification, medications, injections (corticosteroid, platelet rich plasma etc.).
Physiotherapist Lead Exercises
This is the big ticket item! I am going to spend more time in an upcoming blog delving into the practicalities of rehabilitation for a meniscus tear although the evidence based protocols in the scientific literature all involve exercises targeted at:
- Balance
- Proprioception
- Neuromuscular control
- Strength
- Aerobic exercise
Final Word
So the good news is that if you’ve suffered a meniscus tear you’re going to get better! Whether your journey is though surgery or exercise or both. This article is not written to convince you either way, it’s merely intended inform you of what the scientific evidence says about surgery.
A lot of the evidence is in degenerative tears in mostly middle-aged and older individuals. Surgical options may have more of a place in a younger active population. There has been evidence of excellent outcomes of meniscal repair with young athletes (18).
Finally, every patient is individual and has different needs, goals and symptoms. At the end of the day you need to ask yourself… “does surgery match my need and goals?” and “am I willing to try physiotherapy for 3-6 months before considering surgery?”. This is an important discussion to have with your GP, orthopaedic surgeon and physiotherapist.
Summary
- Meniscus tears are VERY common especially as we age
- Two broad categories of tears include traumatic and degenerative (non-traumatic)
- Surgical options include total meniscectomy (cut it all out), partial meniscectomy (cut some of it out), repair (stitch it up)
- Three large & high quality review studies have concluded that in the long-term surgery offers no better result than exercises alone (plus multiple more)
- A positive outcome doesn’t appear to be reduced by waiting for surgery
- It is important to have a discussion with your GP, orthopaedic surgeon & physiotherapist about your options
Dr Christopher Vertullo – Orthopaedic Knee Surgeon Episode 86 of The Physical Performance Show

James Gardiner
POGO Physiotherapist
Book an Appointment with James here.
Featured in the Top 50 Physical Therapy Blog
References
- Brukner, P., & Khan, K. (2018). Brukner & Khan’s clinical sports medicine: Injuries (5th ed.). McGraw-Hill Education Australia.
- Doral, M. N., Bilge, O., Huri, G., Turhan, E., & Verdonk, R. (2018). Modern treatment of meniscal tears. EFORT Open Reviews, 3(5), 260-268.
- Faunø, P., & Nielsen, A. B. (1992). Arthroscopic partial meniscectomy: A long-term follow-up. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 8(3), 345-349.
- Grant, J. A., Wilde, J., Miller, B. S., & Bedi, A. (2012). Comparison of inside-out and all-inside techniques for the repair of isolated Meniscal tears: a systematic review. The American Journal of Sports Medicine, 40(2), 459-468.
- Herrlin, S., Hållander, M., Wange, P., Weidenhielm, L., & Werner, S. (2007). Arthroscopic or conservative treatment of degenerative medial meniscal tears: A prospective randomised trial. Knee Surgery, Sports Traumatology, Arthroscopy, 15(4), 393-401.
- Horga, L. M., Hirschmann, A. C., Henckel, J., Fotiadou, A., Di Laura, A., Torlasco, C., D’Silva, A., Sharma, S., Moon, J. C., & Hart, A. J. (2020). Prevalence of abnormal findings in 230 knees of asymptomatic adults using 3.0 T MRI. Skeletal Radiology.
- Howell, R. (2014). Degenerative meniscus: Pathogenesis, diagnosis, and treatment options. World Journal of Orthopedics, 5(5), 597.
- Katz, J. N., Brophy, R. H., Chaisson, C. E., & Chaves, L. D. (2013). Surgery versus physical therapy for a Meniscal tear and osteoarthritis. New England Journal of Medicine, 368(18), 683-683.
- Khan, M., Evaniew, N., Bedi, A., Ayeni, O. R., & Bhandari, M. (2014). Arthroscopic surgery for degenerative tears of the meniscus: A systematic review and meta-analysis. Canadian Medical Association Journal, 186(14), 1057-1064.
- Lee, D., Park, Y., Kim, H., Nam, D., Park, J., Song, S., & Kang, D. (2018). Arthroscopic meniscal surgery versus conservative management in patients aged 40 years and older: A meta-analysis. Archives of Orthopaedic and Trauma Surgery, 138(12), 1731-1739.
- Mordecai, S. C. (2014). Treatment of meniscal tears: An evidence based approach. World Journal of Orthopedics, 5(3), 233.
- Nepple, J. J., Dunn, W. R., & Wright, R. W. (2012). Meniscal repair outcomes at greater than five years. The Journal of Bone and Joint Surgery-American Volume, 94(24), 2222-2227.
- Rathleff, C. R., Cavallius, C., Jensen, H. P., Simonsen, O. H., Rasmussen, S., Kaalund, S., & Østgaard, S. E. (2013). Successful conservative treatment of patients with MRI-verified meniscal lesions. Knee Surgery, Sports Traumatology, Arthroscopy, 23(1), 178-183.
- Rogers, M., Dart, S., Odum, S., & Fleischli, J. (2019). A cost-effectiveness analysis of isolated Meniscal repair versus partial meniscectomy for red-red zone, vertical Meniscal tears in the young adult. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 35(12), 3280-3286.
- Roos, H., Lauren, M., Adalberth, T., Roos, E. M., Jonsson, K., & Lohmander, L. S. (1998). Knee osteoarthritis after meniscectomy: Prevalence of radiographic changes after twenty-one years, compared with matched controls. Arthritis & Rheumatism, 41(4), 687-693.
- Stensrud, S., Roos, E. M., & Risberg, M. A. (2012). A 12-Week exercise therapy program in middle-aged patients with degenerative meniscus tears: A case series with 1-Year follow-up. Journal of Orthopaedic & Sports Physical Therapy, 42(11), 919-931.
- van de Graaf, V. A., Wolterbeek, N., Mutsaerts, E. L., Scholtes, V. A., Saris, D. B., De Gast, A., & Poolman, R. W. (2016). Arthroscopic partial meniscectomy or conservative treatment for Nonobstructive Meniscal tears: A systematic review and meta-analysis of randomized controlled trials. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 32(9), 1855-1865.e4.
- Vanderhave, K. L., Moravek, J. E., Sekiya, J. K., & Wojtys, E. M. (2011). Meniscus tears in the young athlete. Journal of Pediatric Orthopaedics, 31(5), 496-500.
- Østerås, H., Østerås, B., & Torstensen, T. A. (2012). Medical exercise therapy, and not arthroscopic surgery, resulted in decreased depression and anxiety in patients with degenerative meniscus injury. Journal of Bodywork and Movement Therapies, 16(4), 456-463.
- Van de Graaf, V. A., Noorduyn, J. C., Willigenburg, N. W., Butter, I. K., De Gast, A., Mol, B. W., Saris, D. B., Twisk, J. W., & Poolman, R. W. (2018). Effect of early surgery vs physical therapy on knee function among patients with Nonobstructive Meniscal tears. JAMA, 320(13), 1328.






