

Proximal hamstring tendinopathy is a common running and triathlon ailment. It affects many active individuals and also sedentary individuals alike. We know that 11% of all running injuries occur at the hip or pelvis (van Mechelen, 1992), but there are no epidemiological statistics specifically relating to the incidence or prevalence of proximal hamstring tendinopathy that can be sourced from the literature.
For individuals suffering from proximal hamstring tendinopathy it can be frustrating to navigate the rehabilitation required, and oftentimes symptoms may persist for extended periods of time, ranging from months even extending to years.
As a result there are many athletes and individuals experiencing proximal hamstring tendinopathy who may become dismayed and lose hope with ever getting rid of the symptoms or making meaningful progress.
It is for this reason that I wanted to produce a evidence based, comprehensive and freely available guide for runners and triathletes looking to get back to their physical best and on top of their proximal hamstring tendinopathy symptoms.
The blog will review the diagnosis of PHT, best practice rehabilitation of PHT, mistakes to avoid, and re-introduction to running/training loads.
Diagnosing Proximal Hamstring Tendinopathy
Successful rehabilitation is always under- pinned by an accurate diagnosis. I have seen athletes be unnecessarily frustrated and stagnated with any meaningful rehabilitation progression due to being incorrectly diagnosed with PHT or more commonly misdiagnosed as not having it.
When it comes to proximal hamstring tendinopathy (PHT) several chief signs and symptoms exist.
a. Symptoms of PHT
The athlete suffering from proximal hamstring tendinopathy will typically report pain over the area of the ‘sitting bone’ or deep buttock. The reported pain may vary in intensity from mild and annoying to very debilitating and intense.
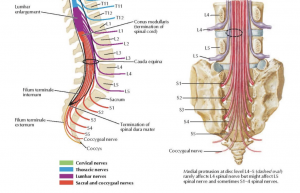
Anatomically this region is known as the ischial tuberosity. The three hamstring muscles have a common origin via their tendons on the outside (lateral) border of the ischial tuberosity. The long head of the biceps femoris and the semitendinosus originate more medial, distal, and deeper on the sitting bone via what is referred to as the ‘conjoint tendon’. This conjoint tendon has been reported to comprise 57.4% of the total common hamstring origin attachment. The semimembranosus muscle originates via its tendon more laterally and proximally in a crescent shape comprising 42.6% of the area of the proximal hamstring complex (Temponi, et. al, 2016)
See the below images for an illustration of the anatomy.
Of significance is that the sciatic nerve is approximately 1.2cm lateral to the most outside edge of the ischial tuberosity positioned underneath the piriformis muscle in the majority of people. The sciatic nerve can be a contributory source of symptoms for some people experiencing proximal hamstring tendinopathy.
When it comes to location of the tendon pathology for proximal hamstring tendinopathy it has been reported that all three of the hamstring tendons can be affected with perhaps a greater prevalence for the semimembranosus to be affected more often (Lempainen, et. al, 2009), with insertional tendinopathy appearing to be more common for PHT than mid portion tendinopathy.
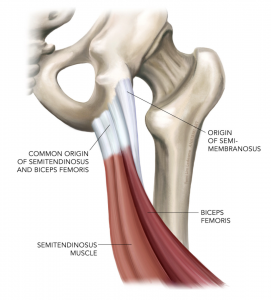
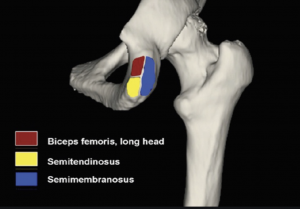
Image Source: Ortho Bullets: Hamstring Injuries
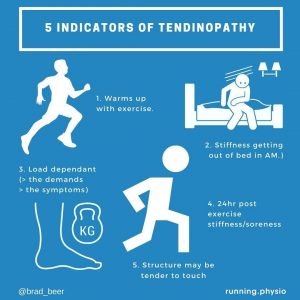
True tendon/tendinopathy pain (ie PHT) will present in a manner that is what clinicians refer to as ‘load dependant’. This means that pain will be increased with the muscle tendon unit being required to produce more force (ie greater load). For example while a steady run pace may be tolerable where the hamstrings are required to produce less force, in cases of true PHT a faster running speed will produce heightened symptoms. If load dependency cannot be determined during a clinical history and examination it may indicate that the presenting complaint is not tendon related.
This load dependency and subsequent tendon response can be a key differential diagnosis tool that the therapist must listen out for when taking a history, and that the athlete needs to be aware of.
Likewise the ‘24hr sign’ is a well established characteristic of pain and symptoms experienced by an individual dealing with tendinopathy. This is where the next morning or circa 24hrs after activity the tendon symptoms and stiffness may be exacerbated, proportionate to the loading and activity undertaken in the prior 24hrs. For example if you have completed a run session involving intensity work in the evening you may expect to wake up the next morning experiencing stiffness and pain in the region of the proximal hamstring tendon origin/sitting bone.
Characteristic aggravating activities that the athlete suffering from PHT will typically report include:
- A progressive onset of pain and stiffness around the sitting bone (ischial tuberosity). It should be noted that there can also be cases of acute PHT strains that progress onto more persistent cases that mimic tendinopathy presentation with time.
- Pain with sitting or pressure on the area. With prolonged sitting often triggering greater symptoms of pain or stiffness in the area of the sitting bone than shorter or lesser periods of sitting.
- Pain with activities that involve forward flexion. These may include: putting shoes/ clothing on, time trial position for cyclists, yoga, incidental bending down to the ground to pick things up, or any position where the hip joint is maximally flexed.
- Pain with activities that involve deep hip flexion: these may include loaded squatting (eg deep back squats in the gym), sprinting, deadlifts, hiking steep hills, or hill sprinting. These activities increase compressive tendon loads at the hamstring tendon which can enhance provocation of symptoms.
- Runners may report pain following speed work (where hip flexion is greater), and/or hill running.
- Triathletes may report symptom exacerbation with time spent on time trial bikes where the hip is in greater degrees of flexion than on a road bike.
It is important to note that an absence of such reported signs listed above for classical ‘tendon behaviour’ may alert the athlete and therapist to potential other diagnoses for the symptoms being experienced. These potential differential diagnoses are detailed below.
The below infographic summarises characteristic tendinopathy/ tendon pathology behaviour:
b. Differential Diagnosis of PHT
Furthermore it is important to differentiate true PHT from several other possible differential diagnoses that may mimic or contribute to symptoms of PHT. The treating therapist and athlete must differentiate true proximal hamstring tendinopathy from the below:
Hamstring muscle strain
Such a strain may or may not involve the proximal hamstring tendon. If the tendon is involved in a strain it will add time to the overall required injury recovery period. Athletes who experience a strain will report a mechanism of injury which involved an acute onset of pain. This may for example involve a position of hip flexion whilst running (such as bending to pick something up off the ground while running) or strains can occur during terminal knee extension when sprinting when hamstring forces have been shown to be the greatest (Yang et al., 2016)
Sciatica /referred pain from the lower back
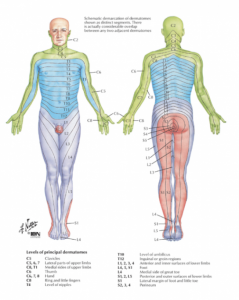
If symptoms extend into the belly of the hamstring itself or across the lower back, upper gluteal region consideration needs to be given to the possibility of pain in the PHT region being possibly neurologically derived such as through L5, or S1 nerve root irritability/pathology. Such an individual may not report symptoms characteristic of a tendinopathy as prior outlined but rather may report ‘sciatica’ symptoms which can include worsening of symptoms in the evening, and aggravation with prolonged sitting that extends distally beyond the PHT region possibly into the lower calf or even foot.
The referral of pain may be due to disc injury (disc protrusion, or extrusion) or localised lumbar spine vertebral changes (osteoarthritis of the facet joints, or narrowing of the exit foramina for the nerves), or spinal nerve root irritation of L5/S1..
Provocation tests such as the Straight Leg Raise Test or the Slump Test are good indicators of neural pain in the area of the PHT.
See the below image from Netter: Atlas of Human Anatomy for the region innervated by the L5/S1 nerve roots which can produce pain in the area of the PHT.
It is also important to not miss the individual presenting with a ‘mixed pathology’ which may include the proximal hamstring tendon and adjacent sciatic nerve, which in protracted cases of PHT can become sensitised and contribute to the clinical presentation.
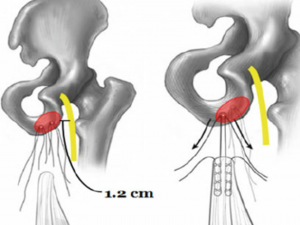
Source: Harris et. al, 2015: Surgical Technique Open Proximal Hamstring Repair
Ischial tuberosity bone stress injury
While uncommon bone stress injuries can occur at the ischial tuberosity due to excessive muscular force (tensile, compressive, and rotational) being applied to the bone. MR imaging is required to assess for bone marrow oedema at the PHT and subsequent diagnosis of a bone stress reaction of the ischial tuberosity. Plain film imaging has been reported to be normal in up to 70% of patients with a pelvic stress fracture (Yang et al, 2016)
Avulsion fractures can occur when the hamstring tendon fractures the ischial tuberosity pulling it away from the pelvis. The mechanism for such a bone stress injury often involves sudden and forceful hip flexion, while one case study reported that prolonged periods into end or range hip flexion invoked a ischial tuberosity stress fracture (Yang, et al., 2016). The patient will typically experience a sudden onset of pain +/- sensation of tearing or ‘popping’ and an inability to bear weight.
Many authors suggest displacement of 2 to 3 cm, painful non-union, exostosis formation, neurologic symptom as an indication for surgery. While others report that some patients who had displacement of more than 5 cm eventually regained muscle strength nearly equal to contralateral leg (Yang, et al., 2016)
Ischiofemoral impingement (IFI)
This is a form of impingement whereby the morphology (shape) of the femoral lesser trochanter and ischium may result in groin and or buttock pain. The contact between opposing bone surfaces typically occurs in positions of repeated hip extension, adduction, and external rotation. Females are more predisposed to IFI. Painful clicking sensations may be reported. Clinical diagnostic special tests are not sensitive and lacking with diagnosis typically being made by the presence of bone marrow oedema around the quadratus femoris muscle, and/or reduced space between the ischial tuberosity and lesser trochanter of the femur (see MR image below evidencing oedema of the quadratus femoris muscle between opposing ischial tuberosity and lesser trochanter bone surfaces)
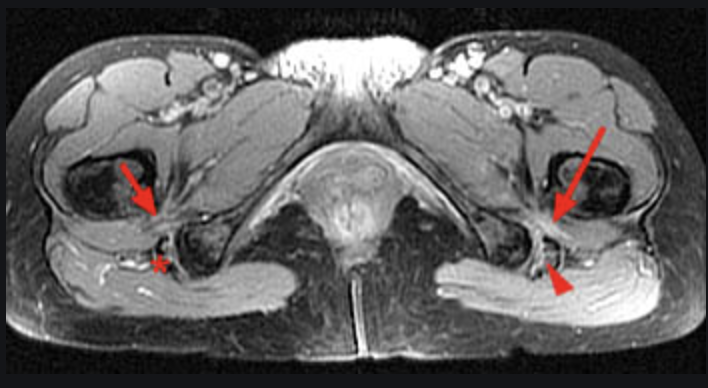
Image Source: Radsource.us
Ischiogluteal bursitis
Ischiogluteal bursitis often co-exists in combination with PHT. It is frequently reported on imaging of the PHT region (diagnostic ultrasound and MRI). The bursa lies between the gluteus maximus and ischial tuberosity.
If ischiogluteal bursitis is suspected to be a potential driver for an individual’s pain clinically a course of NSAID (anti inflammatory medication) may be prescribed or warranted.
In most instances whereby PHT symptoms co-exist with bursitis the chief pain driver tends to be the active tendinopathy.
For more on ischiogluteal bursitis click HERE>>
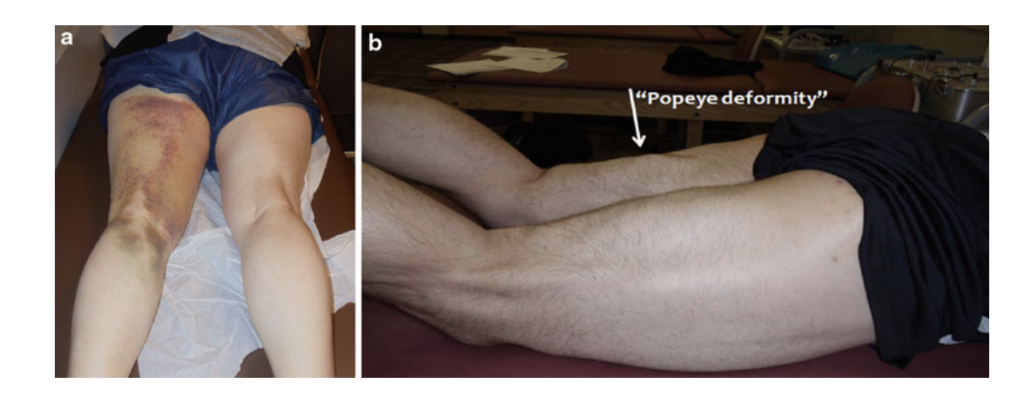
Proximal hamstring tendon rupture
The below image illustrates the appearance of the posterior thigh whereby a complete rupture of the proximal hamstring tendon has occurred as evidenced by the ‘popeye’ sign. That is the proximal hamstring tendon has completely dissociated away from the origin sote being the sitting bone (ischial tuberosity)
Athletes in their early-mid forties with underlying proximal hamstring pathology are most vulnerable.
Ruptures can occur with slips or falls whereby the knee is suddenly extended and the hip is suddenly flexed as someone falls.
Ruptures can be mistaken for strains of the hamstring, however some of the ‘tell tale’ signs can be: a reported sensation of ‘being shot in the thigh’, feeling or hearing a pop in the back of the leg, marked bruising in the back of the thigh and glute region, an antalgic (hobbling) gait pattern, and clinically the ‘Bowstring sign’ may be present whereby there is a notable lack of tension in the distal hamstring muscle mass with active knee flexion while in prone.
Treatment of proximal hamstring tendon ruptures is well summarised by Wood et al (2008) Classification system-see below:
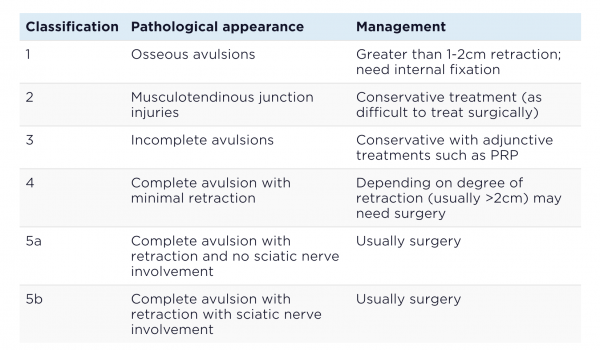
Image Source: Sports Injury Bulletin
- Single tendon rupture that has retracted 1-2cm is well managed conservatively, while surgical criteria include: two tendon ruptures with > 2cm retraction, complete rupture of all three tendons, and failed conservative treatment with persistent pain.
- To read more about proximal hamstring avulsion management and injuries click HERE>>
- Central sensitisation
- With persistent cases the spinal cord may become involved through a process of what is clinically referred to as ‘central sensitisation’. This process results in heightened sensitivity.
- People with central sensitisation may experience: pain that spreads and shifts in location, secondary hyperalgesia (an increase in pain sensitivity when a noxious stimulus is delivered to a region surrounding, but not including, the zone of injury), and pain that is not load dependent or proportionate to the extent of the injury.
- Objectively questionnaires may be used to assess for central sensitisation including: Central Sensitisation Inventory and the Pain Sensitivity Questionnaire.
- To read more about central sensitisation click HERE>>
c. Assessing for PHT
Assessment of PHT like any tendinopathy is reliant on a sound history of onset and current symptomatology being taken by the treating clinician.
In addition to this comprehensive subjective assessment a clinician will need to use provocative diagnostic tests to determine structures involved and to differentiate between the aforementioned differential diagnoses.
Diagnostic provocative tests typically include a progression along the below, noting that speed is used to increase load and pain provocation. The clinician is looking for a load dependency or increase in symptoms with increasing difficulty and demands of the below tests.
- Short lever (bent knee) bridge

- Long lever (straight leg) bridge
- Long lever bridge with speed
- Long lever bridge with perturbation
- Single leg deadlift

In addition to the above provocative tests stretch tests such as the bent knee stretch test & modified bent knee stretch test have the highest validity and reliability scores from the literature (Cacchio et al, 2012).
Furthermore in addition to these localised special tests looking to reproduce symptoms the clinician also needs to determine individual muscle capacities through ‘capacity testing’ the key muscles that comprise the runner’s ‘kinetic chain’.
Such muscles that need capacity testing include the quadriceps, hamstrings, adductors, hip abductors, and plantar flexors. Any identified side to side discrepancies, or notable muscle strength deficits should be targeted through the rehabilitation program along with the local hamstring muscle tendon unit.
Benchmarks for the hamstring capacity are based on a prone hamstring curl whereby an athlete would ideally be able to prone hamstring curl 0.3-0.4 x their body mass single leg with good control concentrically and eccentrically, being able to complete 4x8reps (see below and view HERE>>).

What causes PHT?
As with any tendinopathy the chief cause of symptoms is an exceeding of the muscle tendon unit’s ability to tolerate loads that it is being exposed to.
Classically an athlete may report an increase in training loads preceding the onset of PHT.
It has been estimated that 60% of all running related injuries are due to training errors. Training errors can be doing too much too soon, too hard, too often as outlined by Dave Poulter in the below image:
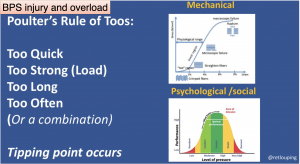
Image Source: Dave Poulter @retlouping
Amongst runners developing PHT I have observed an increase in overall training volume, intensity, and or the addition or increase in hill running to be workload changes that can be identified in a presenting athlete’s history.
Additionally periods of greater time spent sitting and/or stretching the hamstrings in compressive positions (e.g. yoga poses) can be reported by people who develop PHT.
Goom et al (2016) have reported that systemic factors may reduce the threshold for tendon pain and pathology from load -related factors. Such systemic factors that may increase the risk of developing tendon pain include hormonal changes such as perimenopause (may negatively affect tendon morphology & biomechanical properties), medications including antibiotics such as fluoroquinolone, metabolic disorders such as insulin resistance, and genetic polymorphisms such as COL5A.
Role of the hamstrings
Before we look at the rehabilitation of PHT it is worth appreciating the role that the hamstring muscles play in the running gait. The infographic below depicts five of the key roles of the hamstring muscle group, from one-third of the ‘push off’ power/force generation required for running to holding a runner’s form together as the runner fatigues.
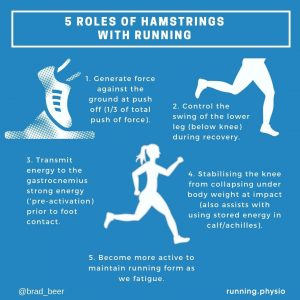
I have expanded on the roles of the hamstrings with running in more detail in a prior blog post HERE>>
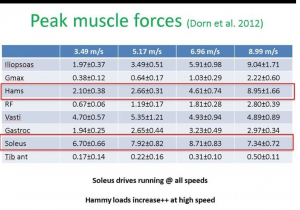
The below image from Dr Peter Malliaras summarises research findings whereby the hamstring muscle fore production was shown to increase from approximately 2 x body weight at 6min km pace (jogging) to beyond 8x body weight at fast/maximal sprinting speeds.
So recognising the importance of the hamstrings and therefore the strength and tissue abilities of the hamstrings as a muscle group let’s now delve into the practical how to’s of rehabilitation for proximal hamstring tendinopathy.
Conservative Rehabilitation (non surgical):
Conservative rehabilitation is the mainstay of rehabilitating PHT and any tendinopathy condition.
Successful tendinopathy rehabilitation requires optimising outcomes at all levels of dysfunction: tendon, muscle, kinetic chain, and brain. The chief reason I observe PHT persisting is typically when rehabilitation programs do not load the athlete enough with localised hamstring strength gain.
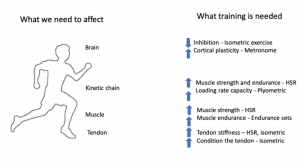
Image Source: Jill Cook: Management of Tendinopathy: La Trobe Head to Toe Symposium
The Brain
Tendinopathy rehabilitation needs to be undertaken with the biopsychosocial framework in mind (see below image). The treating practitioner needs to not just think about the rehabilitation of the affected tissues (ie proximal hamstring) but also the influence of the individuals beliefs regarding their condition and rehabilitation, and consider any social influences that may affect the outcome or expectation of rehabilitation.
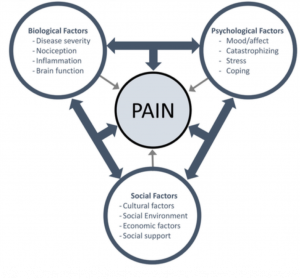
Image Source: Ben Cormack
Practitioners need to be very mindful with language and avoid using nocebic terms (eg ‘tendinitis’ and ‘tears’) when educating patients as this can negatively impact on the individual’s willingness to undertake the required strength loading program, and drive elements of fear avoidance behaviours whereby the individual does not want to exercise their leg due to the belief that the pain is signalling tissue ‘damage’.
Good questions to ask in order to enhance understanding of an individual’s beliefs re their PHT rehabilitation/condition can include:
- What do you think has caused this?
- What is your understanding of this condition?
- Do you believe this can improve?
- What do you believe will help you get this right?
- How long do you think this may take you to fully recover from?
These questions really do yield insights and therefore opportunities to coach and steer the PHT sufferer forwards with evidence based best thinking and action.
Beyond clarifying limiting beliefs, retraining the brain in cases of PHT also needs to address the control or regulation of movement or force generation, in this case from the hamstrings.
In simple terms in cases of persistent tendinopathy and painful conditions the brain’s organisation of movement can become ‘disorganised’ whereby there is heightened ‘inhibition’ and reduced motor drive or muscle excitement on an attempt to recruit a muscle. Dr Ebonie Rio during Expert Edition 222 of The Physical Performance Show described movements of someone with persisting tendinopathy being analogous to a ‘learner driver’, where they have one foot on the brake and one foot on the accelerator. That is when it comes to producing movement of the affected muscle group -in this case the hamstrings- there is inhibition overriding the drive to recruit-which needs to be addressed.
Dr Rio’s scientific work (2016) has focussed on the use of external auditory cues while performing rehabilitation exercises which has been shown to positively influence the brain and motor drive. A great way to include the required external auditory cue is to simply use a metronome with targeted gym exercises or home exercises. My go to is MetroTimer app freely available from the Apple App Store (see below) set to 60bpm.
Example of metronome app: The Metronome App
Failure to incorporate such motor drive training may result in an inability of the targeted muscle to perform the required task. Using the metronome practically may look like: 3s concentric phase of exercise, and a 4s lowering (eccentric phase) for 4 x 8 reps completing a prone hamstring curl in the gym. Therapists are aiming to use metronome retraining to make hamstring exercises skilled tasks which enhance cortical (brain)drive compared with strength exercise prescription without the use of a metronome.
The Kinetic Chain
Successful tendinopathy rehabilitation must include identification and correction of any muscle group weaknesses that form the kinetic chain for the individual/athlete. Looking ‘below and above’ the affected /symptomatic body region is required. For example with PHT rehabilitation, the quadriceps, hamstrings, and plantar flexors (calf musculature) must be addressed.
Clinical benchmarks for key running related muscle groups that I use for kinetic chain rehabilitation are listed below:
- hamstrings (0.3-0.4 x body weight) 4x8reps [prone hamstring curls]
- quadriceps (0.4-0.5 x body weight) 4x8reps [leg extension machine]
- hip abductors (0.15-0.25x body weight) 4x8reps or side bridging of at least 1min [cable abductions]
- adductors (aiming for 30s-90s) [adductor chair plank test]
- soleus (1.0-1.5 x body weight) 4x 8reps [seated calf raises]
- gastrocnemius (0.3-0.4 x body weight) 4x8reps [standing calf raises]
I will incorporate kinetic chain rehabilitation into PHT rehabilitation programs as early as possible-with both home and gym based exercise prescription. Progressing resistance loads is paramount for kinetic chain musculature and overall successful PHT rehabilitation.
I will tend to prescribe isolated muscle group work early in the rehabilitation program that will progress into compound movements such as squats, deadlifts, and step ups.
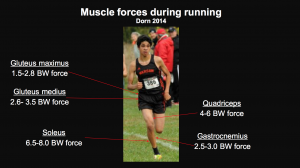
The below image from Dr Rich Willy renowned running researcher depicts the muscle forces that are produced by kinetic chain muscle groups when running. These muscle groups all need to be addressed with tendon rehabilitation. The more persistent tendon pain has been the greater the need to typically address resultant weaknesses of muscles above and below the symptomatic site.
The Muscle
In all cases of lower limb tendinopathies the muscle attaching to the symptomatic tendon will exhibit varying degrees of weakness. In the case of PHT the attaching hamstring musculature will be deconditioned and ‘weak’.
Typically the longer the case of symptomatic tendinopathy the weaker the attaching muscle will be.
Successful rehabilitation requires restoration of the muscle tendon unit’s energy storage capacity. That is the ability of the muscle/tendon unit to produce, store, and release force for propulsive and braking purposes.
Clinical benchmarks are used to determine the starting point for hamstring strength and to also calculate the desired strength level that will be required.
As outlined above the clinical benchmark I utilise for hamstring strength work is:
- (0.3-0.4 x body weight) 4x8reps [prone single leg hamstring curls] as shown below
It is not uncommon to see sufferers of PHT struggling to perform a prone single leg hamstring curl of 2.5-5kgs, evidencing marked inhibition of the hamstring musculature.
Oftentimes it is a ‘powerful moment’ of the rehabilitation journey when the injured athlete/ individual experiences the difference in strength between their symptomatic and asymptomatic sides perforong a prone hamstring curl. The patient will tend to ‘get it’ when they can feel the strength difference-which has the further advantage of instilling motivation and adherence with the required prescribed corrective exercise program.
To remedy the strength deficit of the hamstring it is key to isolate the hamstrings with the prescription of prone single leg hamstring curls.
I will prescribe typically 4x8reps initially performed with a metronome 2s up (concentric), 3s down (eccentric phase), as shown below:
There are a myriad of further hamstring exercises progressing beyond isolated prone hamstring curls which increase the demands on the hamstrings.
An example of such progressive exercise prescription may include:
- Glute hamstring raises. These can be progressed from double leg to singe leg (as shown below), and with progressive heel height e.g. from the floor to having the heel(s) elevated on a chair or bench.


- Heel sliders progressing from double leg to single leg
View HERE>>
- Back raises progressing from double leg to single on either horizontal or 45degree machines.


- Gym ball hamstring curls progressing from double leg to single


View HERE>>
- Harrop curls
View HERE>>
- Nordics (assisted or unassisted) and associated variations
Assisted HERE>>

Unassisted HERE>>

Introducing step up exercises that take the hip into flexion and expose the PHT region to compressive and tensile loading can be important, such as shown below:
Furthermore progressively adding in squatting and variants of deadlift exercises is also required for successful PHT rehabilitation, with progressive exposure to compressive and tensile tenon loading being key.
Exercise prescription can include:
- Smith rack squats
- Back squats progressing from body weight to loaded in a squat rack
- Romanian deadlifts

- Staggered romanian deadlifts
- Single leg romanian deadlifts (dumbell or barbell)
- Rear foot elevated split squats
In summary, effective and successful PHT rehabilitation exercise prescription must be progressive, individualised, and matched to the demands of the affected athlete’s sports and activities of daily living.
The exercise rehabilitation must progress through the stages outlined by Cook and Docking (2015) strength, energy storage, and energy storage and release.
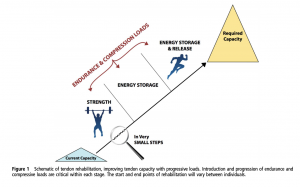
Image Source: Cook & Docking (2015)
Progression through the stages must be symptom led and not time based. General guidelines for working through a rehabilitation program are to monitor symptoms 24hr post completion of the program. Pain (eg 0-3/10) during and post exercise is typically acceptable. If irritability and symptoms worsen the exercise program will need to be modified accordingly.
It is widely accepted and clinically a consistent observation that individuals will experience symptoms flares and tendon irritability as they progress through the rehabilitation stages. I have found that ‘counselling’ patients through these flare ups is key in order to ensure adherence to the continuing with the program.
The Tendon
Isometric holds (prone or supine) in positions that are not compressive for the PHT sare routinely prescribed and can be ‘analgesic’ for an irritable and symptomatic PHT. These isometric holds e.g. 5×20-45s can be very helpful when trying to reduce pain levels in early tendon rehabilitation. Rio et al (2014) found that isometric holds of moderate resistance isometric exercise performed at 70% MVC (maximal isometric voluntary contraction) reduced tendon pain (patellar) and provided longer relief than isotonic exercise.
Isometric holds can be performed in either the prone position or the supine position as shown below. Prone hamstring isometrics can be useful when the irritability of someone’s tendon pain is high, precluding them from being able to perform supine holds without pain.
A progression beyond the prone hamstring isometric curl can be single leg back extensions as shown below:
Energy storage exercises represent the final phase of tendon rehabilitation. These exercises are challenging to perform and confer large amounts of load on the muscle/tendon unit.
Examples include hamstring plyo taps shown below:
Running drills can also be used for exposing the hamstring muscle/tendon to plyometric loads which mimic that which occurs with running. Such drills cans include: bounding, split squat jumps, A-skips, B-skips, high knees etc
An example of some running drills can be viewed below:
Non Conservative Rehabilitation: Surgical
As outlined above conservative rehabilitation is the mainstay of successful proximal hamstring tendinopathy rehabilitation.
Surgery is rarely required with proximal hamstring tendinopathies.
However surgical management of proximal hamstring tendon ruptures is indicated for two- or three-tendon ruptures with greater than 1–2 cm of retraction in active, healthy individuals (Harris et. al, 2015). With only one tendon involved or even multiple tendon involvement without significant retraction, nonoperative conservative management may be highly successful (Harris et. al, 2015). For patients with significant comorbidities, or without a desire to return to athletic activities, nonsurgical treatment is considered. Although less successful and predictable, chronic repair or reconstruction may also be warranted secondary to pain, weakness, and loss of function after failed conservative treatment or delay in diagnosis (Harris et. al, 2015).
Acute repairs of PHT ruptures have also been reported to have lower complications and re-rupture rates.
Partial thickness tendon tears can typically be managed conservatively, however I have consulted with athletes who have had surgical intervention for at times substantial partial tearing as opposed to a frank rupture.
Rehabilitation-things to avoid:
When it comes to tendinopathy rehabilitation and PHT rehabilitation there are numerous commonly espoused treatment approaches that people try and recommend to others. Unfortunately there is little evidence base for these modalities and in some instances incorporating these treatment approaches can actually result in unwanted symptom flares and irritability.
These approaches can include direct massage over the affected area, dry needling/acupuncture of the affected area, and stretching of the hamstrings.
While passive therapies such as stretching, massage therapy, acupuncture are frequent ‘go to’ modalities they do not address the deficits outlined above in the affected tendon’s reduced energy storage capacity, and hence will not be effective in rehabilitating PHT.
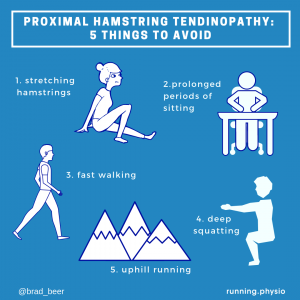
It is also worth noting that being mindful of periods of fast walking and periods of prolonged sitting while working through rehabilitation can also be useful in avoiding avoidable symptom flares. These activities can expose the tendon to excessive tensile and compressive tendon loads which may provoke tendon irritability.
The below infographics outline activities to be mindful of when rehabilitating PHT. It is key to introduce activities with known tensile and compressive loads such as outlined below progressively throughout the rehabilitation.

Adjunctive therapies
Other treatment modalities that are often utilised for PHT rehabilitation can include shockwave therapy, cortisone injections, and platelet rich plasma (PRP) injections.
PRP injection use for PHT rehabilitation has little scientific evidence supporting its use (read more HERE>>).
Meanwhile shock wave therapy (ESWT) use for PHT rehabilitation has mixed results in the literature. I have found that using ESWT for patients with highly irritable PHT may result in an exacerbation of tendon pain. Hence I advocate its use very sparingly for PHT rehabilitation.
Corticosteroid injections into the pathological tendon itself are contraindicated due to risk of tendon rupture. Peritenon injections may modulate pain in the short term however at best may be a ‘calming agent’ with limited overall long term efficacy.
In summary:
As with any lower limb tendinopathy rehabilitation PHT rehabilitation can be challenging and take time. The key steps in successful rehabilitation being to ensure an accurate diagnosis of PHT is made early on. Furthering on from an accurate diagnosis rehabilitation must be focussed on restoring the affected tendon’s energy storage capacity through sound and progressive exercise prescription. Rehabilitation of the overall kinetic chain must not be overlooked.
When patients present with persisting PHT symptoms I find that the rehabilitation efforts and strength benchmarks have not been addressed in full. It is therefore vital that the treating therapist is aware of how ‘far and hard’ and individual will need to be progressed with their rehabilitation exercises.
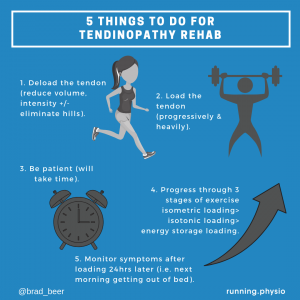
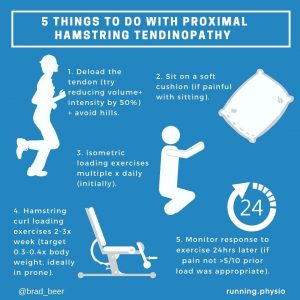
The below infographics summarise the overall treatment approach to successfully treating PHT.
Need help?
If you have read this blog and have been struggling with persisting PHT pathology and would like individual assistance I am available in person or via telehealth appointments.
You can schedule your appointment HERE>>
Related Resources:
1. Podcast Anthony Nasser

2. Podcast Dr Peter Malliaras HERE>>

3. Podcast Dr Ebonie Rio HERE>>
4. Mountain Running Podcast: High Hamstring Tendinopathies with Tom Goom
5. Ortho Bullets: Hamstring Injuries
6. 13 top tips that will help your proximal hamstring tendinopathy
7. Tendinopathy Update: Current Concepts

Brad Beer
APA Titled Sports & Exercise Physiotherapist (APAM), POGO Founder
Book an Appointment with Brad here.
Featured in the Top 50 Physical Therapy Blog
References:
- Van Mechelen, W. Running Injuries. Sports Medicine 14, 320–335 (1992). https://doi.org/10.2165/00007256-199214050-00004
- Temponi, Eduardo & Costa, Lincoln & Sonnery-Cottet, Bertrand & Vassalo, Carlos & Barros, Antônio. (2016). A New Technique for Surgical Treatment of Proximal Hamstring Tendinopathy in a Triathlon Athlete. J Orthop Case Rep. 6. 69-72. 13107/jocr.2250-0685.638.
- Lempainen L, , Sarimo J, , Mattila K, , Vaittinen S, , Orava S. and Proximal hamstring tendinopathy: results of surgical management and histopathologic findings. Am J Sports Med. 2009; 37: 727– 734. http://dx.doi.org/10.1177/0363546508330129
- Goom TS, Malliaras P, Reiman MP, Purdam CR. Proximal Hamstring Tendinopathy: Clinical Aspects of Assessment and Management. J Orthop Sports Phys Ther. 2016 Jun;46(6):483-93. doi: 10.2519/jospt.2016.5986. Epub 2016 Apr 15. PMID: 27084841.
- Harris, Joshua & Nho, Shane & Bush-Joseph, Charles. (2015). Surgical Technique: Open Proximal Hamstring Repair. 915-920. 10.1007/978-1-4614-6965-0_78.
- Yang BK, Yi SR, Ahn YJ, Im SH, Park SH. Ischial Tuberosity Avulsion Stress Fracture after Short Period of Repetitive Training. Hip Pelvis. 2016;28(3):187-190. doi:10.5371/hp.2016.28.3.187
- Wood DG, Packham I, Trikha SP, Linklater J. Avulsion of the proximal hamstring origin. J Bone Joint Surg Am. 2008 Nov;90(11):2365-74. doi: 10.2106/JBJS.G.00685. PMID: 18978405.
- Cacchio A, , Borra F, , Severini G, , et al.. Reliability and validity of three pain provocation tests used for the diagnosis of chronic proximal hamstring tendinopathy. Br J Sports Med. 2012; 46: 883– 887. http://dx.doi.org/10.1136/bjsports-2011-090325
- Rio E, Kidgell D, Moseley GL, et alTendon neuroplastic training: changing the way we think about tendon rehabilitation: a narrative reviewBritish Journal of Sports Medicine 2016;50:209-215.
- Rio, E., Moseley, L., Purdam, C., Samiric, T., Kidgell, D., Pearce, A. J., … & Cook, J. (2014). The pain of tendinopathy: physiological or pathophysiological?. Sports medicine, 44(1), 9-23.




