



I recently attended the La Trobe Sport and Exercise Medicine Tendinopathy Head to Toe Symposium in Melbourne. The Symposium provided some great updates into all things tendinopathy rehabilitation of both the upper and lower limbs, and was presented by some of the luminaries of tendinopathy research and practice.
My top takeaways from the Symposium speakers were as follows:
1. Professor Jill Cook
Jill presented on ‘10th birthday of the continuum model-where are we now?’ As a co-author of the seminal continuum model of tendinopathy first published in 2009 with Craig Purdam (1) which gave clinicians a framework for approaching the continuum of tendinopathy presentations from acute onset to more persistent it was a wonderful opportunity to learn what has changed in understanding over the ensuing decade since release of the original continuum model . The continuum model of tendon pathology, proposed in 2009, synthesised clinical and laboratory-based research to guide treatment choices for the clinical presentations of tendinopathy (1). See below for the visual of the then proposed continuum model.
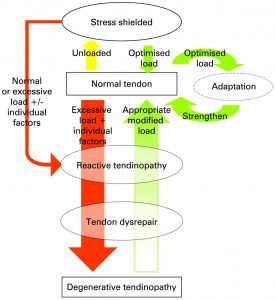
Image Source: Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy, BJSM 2009
My top takeaways from Professor Jill Cooks’ sharings were:
A. The tendinopathy continuum model-update.
Despite quite a bit of ‘noise’ by way of opinion there is no evidence that the continuum model as it was proposed in 2009 is no longer accurate or relevant in practice. The continuum model proposed a model for staging tendinopathy based on the changes and distribution of disorganisation within the tendon. However, classifying tendinopathy based on tendon structure alone in what is ‘primarily a pain condition has been challenged’ (2). The interplay between structure, pain and function is not yet fully understood, which has partly contributed to the complex clinical picture of tendinopathy. The concept that ‘some tendons may have discrete regions that are in different stages at one time’ led Purdam and Cook to publish a framework that illustrates that tendon pathology can also include the ‘hybrid’ reactive on degenerative tendinopathy presentation. Such presentations encapsulates where the ‘normal’ (on imaging) part of the tendon may ‘drift in and out’ of a reactive state (see below):
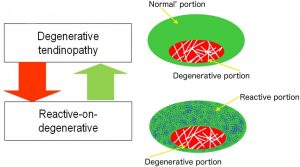
Image Source: Revisiting the continuum model of tendon pathology: what is its merit in clinical practice and research?British Journal of Sports Medicine 2016
B. The role of inflammation in tendinopathy.
Despite there being a reemergence of interest in the presence and role of inflammation in tendinopathy Professor Cook stated that the concentration and levels of inflammatory markers is actually very low and likely to not be a primary driver of pain or pathology. In 2016 Cook et al stated that ‘while inflammatory cells have been observed in pathological tendons the response does not seem to be a traditional inflammatory response’
C. The role of the interfasicular matrix in reactive tendinopathy.
Cook outlined that one area of emerging interest in tendinopathy pathogenesis is the role that the connective tissue of tendons may play in the onset of tendinopathy. Cook outlined that the interfasicular matrix, the matrix between tendon fascicles, also known as the endotendon (see below figure) may play a key role in the pathogenesis of tendinopathy.
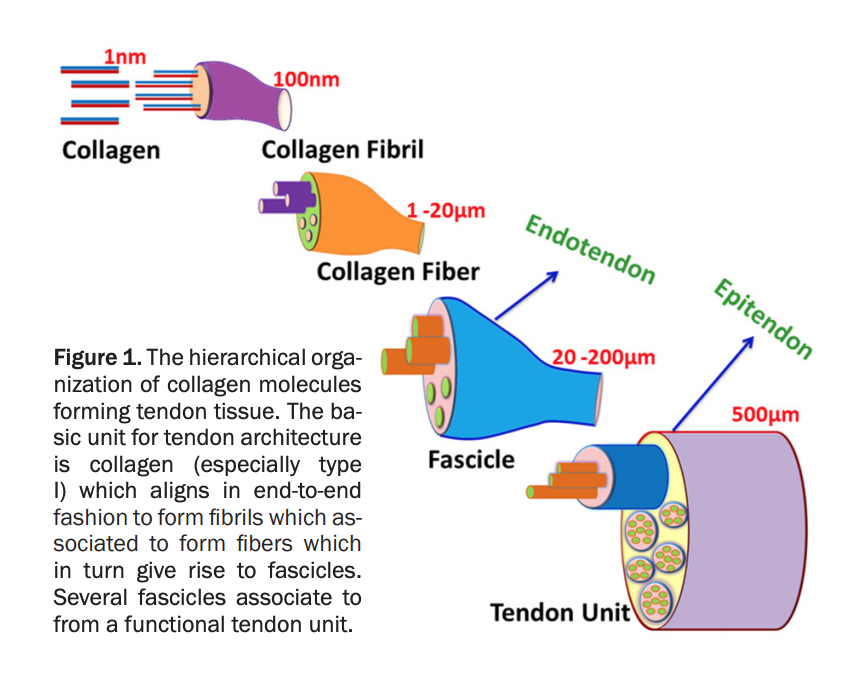
Image Source: Am J Transl Res 2018;10(11):3291-3309
Professor Cook raises the suggestion that perhaps in reactive tendinopathy the change in the interfascicular matrix (swelling or breakdown) may be the start of tendon pathology. This theory may be supported when we consider that reactive tendons can show no tissue changes however they can swell in size and then return to normal size without tendon structural change. The role of the interfasicular matrix in the pathogenesis of tendinopathy may also be supported by the fact that tendon compressive forces alone don’t stir up tendons, however when the tendon is subjected to compressive and tensile forces; which involve sliding and rotation of the interfascicular matrix the tendon may become irritated.
D. ‘Osgood schlatters disease’: how does patellar tendinopathy develop?
Cook spent some time exploring how patellar tendinopathy develops in the adolescent population. Tendons physiologically mature in adolescence & the tendon Cook stated ‘wants to maintain itself at all costs’ (across the lifespan). Cook further extrapolated this by saying that ‘you still have the same tendon at age 80 that you did at age 17yrs’.
Turning the focus towards a common adolescent sporting injury ‘osgood schlatters’ Cook stated that despite popular opinion ‘Osgood Schlatters’ in adolescents is not an apophyseal injury as the patellar tendon does not have a classic apophysis. This made sense to me as I had always wondered as a practitioner how treating irritable patellar tendons in adolescents varied from treating a patellar tendinopathy in the adult population.
Pathophysiologically Cook stated that as an adolescent passes through puberty the patellar tendon develops through an articular cartilage interface and gradually attaches to the tibial tuberosity in an anterior to posterior (front to back) fashion. This maturation of the tendon to bone interface occurs 1-2yrs before peak growth velocity of the adolescent, meaning that this is a key time for jumping loads to be moderated.
Adolescents who jump excessively while they are maturing risk the development of patellar tendinopathy, as are tall athletes who are late to puberty, or involved in jumping based sports. Females who have a late onset of menarche, delayed maturation, and those that participate in low body weight sports (eg dance and gymnastics) are most at risk. Cook outlined that the often observed ‘big bumps’ of the tibial tuberosity present with Osgood Schlatters reflects that too much load was applied to the maturing tendon/bone interface while the adolescent’s body was trying to attach the patella tendon through. With the above knowledge it really brings into question whether the diagnosis of ‘Osgood Schlatter Disease’ really has a place in contemporary sports medicine, rather should patellar tendinopathy in the adolescent population simply be referred to as patellar tendinopathy?
E. Do all tendons have the same response to pathology?
Cook raised the observation that not all tendons in the body (upper and lower limb) tend to respond to pathology in the same way. Some tendons we know to get thicker with an onset of reactive tendinopathy (see C-role of the interfascicular matrix) such as the achilles tendon, while some tendons seem to get ‘thinner’ before ‘letting go’ (e.g. rotator cuff tendons, tibiaais posterior, gluteal tendons). Cook stated that this highlights just how far there is to go in understanding the pathophysiology of tendinopathy.
2. Ebonie Rio
Ebonie Rio has been at the forefront of tendinopathy research and rehabilitation for over a decade. It is always exciting to see Ebonie present. These were my top takeaways:
a. Tendinopathy rehabilitation needs a biopsychosocial framework
Ebonie Rio challenged all practitioners to remember that tendinopathy rehabilitation needs to be undertaken with the biopsychosocial framework in mind. Ebonie reminded the attendees of the need to be very mindful with language and avoid using nocibic terms (eg ‘tendinitis’ and ‘tears’) when educating patients.
B. All levels of dysfunction need to be optimised with rehabilitation
Ebonie also stressed the importance of optimising outcomes at all levels of dysfunction for someone with tendinopathy: tendon, muscle, kinetic chain, and brain. With the brain and motor drive being influenced through external pacing when performing heavy slow resistance rehabilitation exercises through the use of a metronome. Failure to incorporate such motor drive training may result in an inability of the targeted muscle to perform the required task. One of Jill Cook’s slides highlighted the same need to address the brain, tendon, kinetic chain, and muscle with rehabilitation, see below.
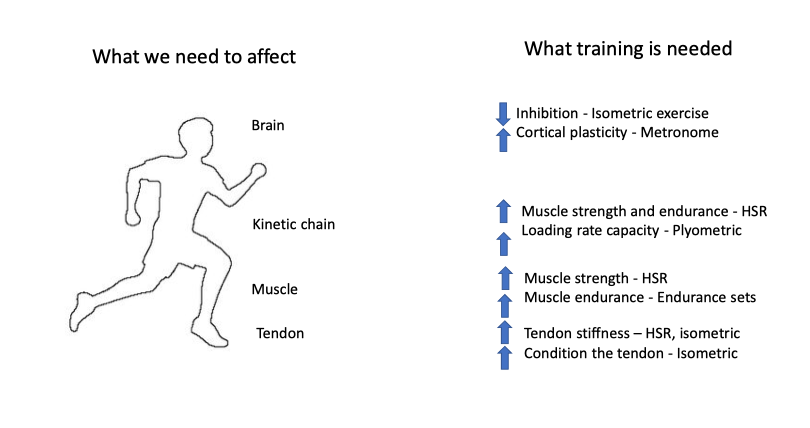
Image Source: Jill Cook: Management of Tendinopathy: La Trobe Head to Toe Symposium
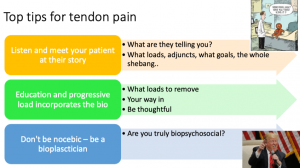
Ebonie Rio’s final slide can be seen below highlighting ‘top tips for tendinopathy rehabilitation’.
3. Myles Murphy : The prognosis of achilles tendinopathy rehabilitation and how to monitor progress.
Myles PhD candidate (University of Notre Dame and SportsMed Subiaco) shared the need to monitor not only patient’s progress, but also their expectations with their tendinopathy rehabilitation. Myles shares the below key considerations for astute achilles tendinopathy rehabilitation:
A. Acknowledging that pain as is typically quantified in practice by the numerical rating score (NRS) of pain has very poor reliability in the management of mid-portion achilles tendinopathy.
B. Alternately Myles shared that the Victorian Institute of Sport Assessment-Achilles tendon (VISA-A) questionnaire has been found to be the only validated and reliable measure for pain and function for mid-portion achilles tendinopathy. Within session functional tests such as a single leg counter movement jump for height may also be useful.
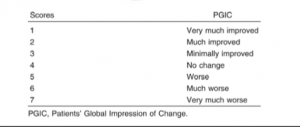
C. For quantifying the patient’s perception of their progress Myles suggested that using the Patient’s Global Impression of Change (see scale below) where the patient is simply asked ‘do you think you are getting better?” is helpful:
D. Myles also explored findings from a systematic review and meta-analysis (3) which looked at the rate of change/improvement of pain and function in mid-portion achilles tendinopathy with loading protocols. The published data demonstrated an improvement in pain and function as early as 2 weeks which then peaked at 12 weeks following the inception of a loading protocol. These findings are interesting given that tendon structure does not change at 2 weeks and muscle hypertrophy is typically not evident until circa 4 weeks following the inception of a rehabilitation loading protocol.
E. Myles suggested that if patients beyond 12 weeks are plateauing with rehabilitation than the following may be worthy of consideration:
- review of the diagnosis (eg may need to consider superficial retrocalcaneal bursa, sural nerve, or the plantaris as possible differential diagnoses)
- Review the loading protocol (underloaded or overloaded and program must be individualised)
- Review exposure to provocative loads-look to amend program as required.
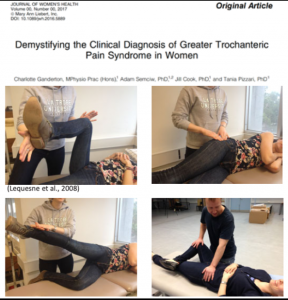
4. Dr Charlotte Ganderton: Greater trochanteric pain syndrome or gluteal tendinopathy
Charlotte Ganderton of Swinburne University presented on lateral hip or gluteal tendinopathy/ greater trochanteric pain syndrome. The below were my top takeaways:
A. Ganderton outlined that some of the known causative factors for gluteal tendinopathy include: post menopausal women, peripheral adiposity, and decreased hip abductor strength.
B. Surprisingly the literature reports that approximately only 20% of gluteal tendinopathy cases involved the trochanteric bursa.
C. Aggravating factors for the onset of gluteal tendinopathy include: repeated compression (eg cross body stretching, sitting with legs crossed, or sudden lateral hip load increases such as walking on cobblestones or on the beach).
D. Assessment items include in room clinical physical examination assessments including: FABER test, palpation, ‘derotation test’, and resisted hip abduction , along with valid and reliable outcome measures such as the Victorian Institute of Sport Assessment-Gluteal tendon (VISA-G). See the below slide from Charlotte’s presentation:
E. Several trials have evidenced that education (reducing abusive loads) and exercise (loading protocol out of tendon compression + kinetic chain loading) are the cornerstones of effective gluteal tendinopathy rehabilitation.
General key takeaways:
Some of my favourite quotes and pearls of wisdom from the Symposium were:
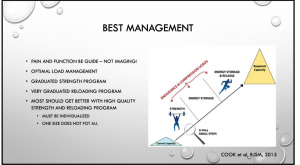
1. Tendinopathy rehabilitation should in essence remain ‘simple’. Jill Cook asserted that it’s simply about learning where your patient is, and where they want to be and simply ensuring that you get them there (ie the below image from Cook et al BJSM 2018 paper) and Sports Doctor Adam Castricum summarises it well:
2. Irrespective of the patient being treated (sedentary or elite athlete) the same process of clinical reasoning and exercise prescription applies. It is only the end point that will be different. Returning someone to their desired function and performance is the aim of intervention.
3. In order to monitor progress with rehabilitation measure load related pain, patient related change, pain related function and disability, psychological measures, and avoid palpating the tendon.
4. There are no recipes when it comes to tendinopathy. Rather work with the patient in front of you and design a loading program that will get them back to their desired function with no consequences to loading.
5. Capacity deficits in the kinetic chain will tend to exist below the level of the tendon pathology. For example a proximal hamstring tendon will often result in muscle weakness of the glutes, hamstrings, quadriceps and plantar flexors.
6. Tendons do not ‘get into trouble’ with low loads (this can include heavy slow resistance exercise), rather it is the high loads on the tendon (eg anything performed fast) that can put the tendon at risk. Knowledge of this can be helpful when educating the patient about why heavy slow resistance training is not to be feared.
7. The response to loading should be a sign post as to whether you are working with a tendinopathy or otherwise: for example a tendinopathy will get better with warm up, worse after loading, than ‘horrible’ the next day. If this is not the case it is unlikely to be a tendon you are dealing with. Furthermore the patient should be educated to not worry about pain after exercise, informing them that if ‘it hurts a bit when you load the tendon than that is OK’.
8. Reassurance can be a key tool in tendinopathy rehabilitation: this can include reassuring the patient that throughout rehabilitation you might occasionally have tendon pain (which is OK) and that if appropriate intervention is followed while the tendon cannot be ‘fixed’ per se (ie structurally unchanged on imaging) it can be returned to pain free full function.
For more information about the La Trobe Tendinopathy Head to Toe Symposium jump over to the La Trobe Symposium page.

Brad Beer (APAM)
APA Titled Sports & Exercise Physiotherapist (APAM)
B.Physio/ B. Ex. Sc
Author ‘You CAN Run Pain Free!’
Founder POGO Physio
Host The Physical Performance Show
Featured in the Top 50 Physical Therapy Blog
References:
(1) Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathyBritish Journal of Sports Medicine 2009;43:409-416.
(2) Cook JL, Rio E, Purdam CR, et al Revisiting the continuum model of tendon pathology: what is its merit in clinical practice and research?British Journal of Sports Medicine 2016;50:1187-1191.
(3) Murphy M, Travers M, Gibson W, Chivers P, Debenham J 4, DockingS, Rio E. Rate of Improvement of Pain and Function in Mid-Portion Achilles Tendinopathy with Loading Protocols: A Systematic Review and Longitudinal Meta-AnalysisSports Med. 2018 Aug;48(8):1875-1891. doi: 10.1007/s40279-018-0932-2.



