


What is Extracorporeal Shockwave Therapy (ESWT)?

Shockwave therapy is non-invasive modality used by therapists to use in combination with exercise prescription to return a tendon and/or muscle to normal function. A large amount of high quality studies have looked at what shockwave therapy is most effective at treating, which shockwave device to use and on which setting.
To just cover a few confusions within the area, “extracorporeal” is not a type of shockwave, the word just means “outside of the body” – therefore all types of shockwaves are extracorporeal. There are two main types of shockwave devices used in clinics:
1. Focus Shockwave
- 3 types (spark discharge, Piezo-electric, electro-magnetic)
- small focal area
- better for bones or deeper structures, spasticity
- more painful
2. Radial Pressure Wave (POGO’s device)
- half the price
- very versatile
- not as accurate or deep
- less painful
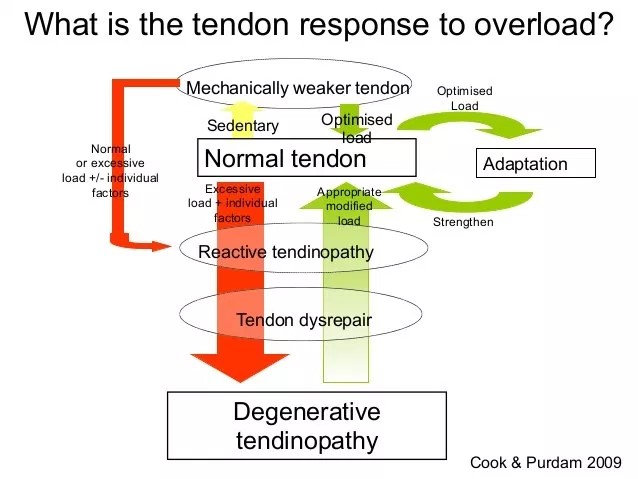
Degenerative Tendons
The timeline of an injured tendon starts with a normal tendon, if there is excessive load or individual errors the tendon may become a reactive. If this continues without altering load or training regime, this “reactive tendinopathy” can enter tendon dysrepair. Once at this stage it is harder to return to a normal tendon and after some time can descend further into chronicity and become a “degenerative tendon”. It is at this stage where ESWT is most effective and is believed to be the only way the tendon can be returned to normal.
Shockwave essentially breaks down this tendon and allows inflammation and remodelling to occur. It increases inflammation via pro-inflammatory neuro-peptides such as substance P and CGRP. This inflammation allows the tendon to attempt to heal at a cellular level. This combined with progressive loading/exercise that is aimed to eventually reach 70% of the client’s max effort – will return the chronic and seemingly helpless tendon back to normal function.
Pain relief
ESWT is well known for its pain relief benefits.Through research, we now know that ESWT has a role in returning a degenerative tendon into a reactive tendon. However, it also does have an analgesic effect. Pain relief by ESWT is best achieved when the machine is used a noxious stimuli via the “pain gate theory”. This means that in order to reduce the pain experienced from a tendinopathy, the shockwave session must be “uncomfortable” or involve a low-mid level of pain.
Shockwave increases inflammation
ESWT is pro-inflammatory, the reason behind its use is to change the cells of a degenerative tendon to a more acute, reactive tendon thus increasing blood flow and stimulating the body’s natural healing process. However, it is important to note that by being pro-inflammatory, non-steroidal anti-inflammatory medications such as mobic and ibuprofen will inhibit the effectiveness of ESWT. Furthermore, CS injections used in combination with ESWT is likely to produce poor outcomes due to the two acting against each other.
It is also recommended that when treating an acute and/or inflamed injury – ESWT is not indicated as the body will attempt to heal the injured structure itself. If this healing fails or “stalls” then ESWT becomes indicated and is a recommended adjunct therapy option.
Indications for shockwave (via the ISMST)
- Achilles
- Plantar fascia +/- heel sput
- Lateral epicondylitis (tennis elbow)
- Greater trochanteric pain syndrome (GTPS)
- Calcifying rotator cuff
- Bone pathologies (non-union)
- Wound healing (work around the wound)
Other indications
- RC tendinopathy without calcification
- Medial epicondylitis (golfer’s elbow)
- Adductors
- Pes anserinus
- Tib post tendon
- Bone marrow oedema (painful)
- Osgood Schlatter Disease (precaution)
- Sever’s Disease (precaution)
Muscle pathologies
- Myofascial pain and MTPs (use single shot not continuous)
- Muscle sprain with discontinuity
Contraindications for shockwave
- Malignant tumour in the treatment area
- Tumours
- Pregnancy/fetus in the treatment area
High energy
- Lung tissue in the treatment area
- Epiphyseal plate in the treatment area
- Brain or Spine in the treatment area
- Severe coagulopathy
Settings
Therapists using the shockwave machine must ensure that you have the correct transmitter attached to the bar. If you are treating a tendon that is superficial then the D20 is appropriate. When treating a deeper tendon or a myofascial trigger point it is recommended you used the D15 transmitter. When selecting the energy, increase the bar pressure setting from the default amount. The default amount is set at the lowest setting of clinical value. Raising it to around 3-5 bar pressure is suggested for majority of tendons and muscles. Research shows that the most beneficial energy (bar pressure) to use on the client is the highest amount that is tolerable. Furthermore, the more energy used per session, the quicker the injury will resolve.
Summary of evidence
When deciding between focus shockwave or radial pressure wave, there remains no statistical significance between the two in regards to treatment outcome, as long as the same EFD (energy) is being used. ESWT has been proven as effective and safe non-invasive treatment option for tendon and other pathologies of high quality RCTs with positive outcomes.
-
- 88.5% (23/26) of all RCTs on radial had significant results
- 81.5% (66 out of 81) of all RCTs on focus had significant results
Optimum treatment protocol for ESWT appears to be 3 treatment sessions at 1 week intervals, with 2000 impulses per session and the highest EFD (energy) that can be applied
-
- If client is unable to tolerate high energy then more sessions may be required
- When treating a tendon it is advised to wait 5 days minimum between sessions
- If after 3 weeks there is little to no improvement then reassess the client, check their injury and stage of healing
It is clear from the research that combining exercise with ESWT provides the best outcomes. Current evidence suggests ESWT may be a reasonable treatment to consider for management of chronic musculoskeletal conditions that fail to respond to conservative care given favourable safety profile and low risk of side effects.
In conclusion, seeking a medical professional that can accurately assess and diagnose your injury as well as deem it appropriate or not appropriate for ESWT is highly recommended.

Alec Lablache
POGO Physiotherapist
Featured in the Top 50 Physical Therapy Blog
References
NB: all information extracted from DJO ESWT course and supplied by shockwave expert and physiotherapist Cliff Eaton. For more information or to answer any question regarding electrotherapy visit www.electrophysicalforum.org or www.djoglobal.com.
- Korakakis, V., Whiteley, R., Tzavara, A., & Malliaropoulos, N. (2018;2017;). The effectiveness of extracorporeal shockwave therapy in common lower limb conditions: A systematic review including quantification of patient-rated pain reduction. British Journal of Sports Medicine, 52(6), 387. doi:10.1136/bjsports-2016-097347
- International Society for Medical Shockwave Treatment (n.d). Introduction and prerequisites and minimal standards of performing ESWT. Retrieved from https://www.shockwavetherapy.org/about-eswt/indications/
- van der Worp, H., Zwerver, J., Hamstra, M., van den Akker-Scheek, I., & Diercks, R. L. (2014). No difference in effectiveness between focused and radial shockwave therapy for treating patellar tendinopathy: A randomized controlled trial. Knee Surgery, Sports Traumatology, Arthroscopy, 22(9), 2026-2032. doi:10.1007/s00167-013-2522-z
- Zhang, L., Fu, X., Chen, S., Zhao, Z., Schmitz, C., & Weng, C. (2018). Efficacy and safety of extracorporeal shock wave therapy for acute and chronic soft tissue wounds: A systematic review and meta‐analysis. International Wound Journal, 15(4), 590-599. doi:10.1111/iwj.12902






