


Bone stress injuries (BSI) occur when the interaction between the number, magnitude, and speed of bone tissue loading cycles exceeds the ability of the bone to resist the applied loads (Hoeing et al 2022). Consideration of a runner’s training workload, physiology, biomechanics, and psychology is warranted in managing BSI in the running athlete (Willy, 2023).
Tibial bone stress injuries are a common running related injury. They are categorised as low risk BSI due to their ability to heal well without complication. The exception to this being tibial BSI occurring in the anterior tibial cortex which may be high risk. Tibia BSI incidence is as high as 10-20% in runners (Feldman et al 2016).
This case study outlines the assessment and management of a low risk tibial BSI with the recently proposed optimal loading management approach (Warden et al 2021), combined with the more traditional MRI informed time based approach to deload periods and return to sport. Diagnosis of a tibial BSI was made combining clinical history, with physical examination, and radiological findings.
The athlete was managed through run deloading, dietetic support, progressive strength and conditioning, and progressive return to run programming.
Following a progressive return to run program the athlete experienced a recurrence in tibial symptoms at the end of the fourth week of running. Despite contemporary science informed BSI management principles being utilised and a comprehensive risk factor evaluation being conducted, the recurrence of symptoms highlights the complexity of managing BSI in running athletes.
Introduction
This case describes the assessment and management of JF, a national level U23 triathlete who presented with posterior mid-tibial pain, and subsequent diagnosis of a posterior tibial BSI. It considers differential diagnoses and a combination of an optimal loading approach combined with a radiological informed deload period as management strategies. The case study highlights the individualised approach required to both identify and address BSI risk factors. The role of the multidisciplinary team in managing BSI is highlighted.
Low risk BSI’s account for greater than 50 percent of all running related injuries (Lopes et al 2012). Sufficient time must be allowed to heal the affected bone, and safely return to sport. BSI tend to be season ending injuries resulting in significant training and competition time loss (Warden et al 2021, Nattiv et al 2013).
Traditionally low risk BSI such as the posterior tibia have been managed with radiological findings informing return to sport timelines (Nattiv et al 2013). More recently an optimal loading management paradigm for BSI based on clinical symptoms has been proposed (Warden et al 2021). This approach is symptom driven and guided by knowledge of BSI biological processes.
No prospective data supports a faster return to running or improved outcomes for an optimal loading management approach compared to a prescribed period of non or protected weight bearing (Warden et al 2021). However, clinically an optimal loading approach may present several benefits including less reduction in regional bone density, better maintenance of cardiovascular fitness, and maintenance of muscle properties such as muscle mass.
BSI risk factors need to be considered as part of the rehabilitation process. These factors include biological and biomechanical factors as shown in Figure 1. Approaches to both rehabilitate and prevent BSI aim to improve the ability of the skeleton to resist load through exercise mediated mechanoadaptive processes of skeletal mass (bone mineral density increases), structure (bone geometry changes), and material quality (bone mineral content increases) (Warden et al 2021). Loads being applied to the athletic skeleton also need to be monitored and manipulated in order to reduce bone microdamage accrual (Warden et al 2021).
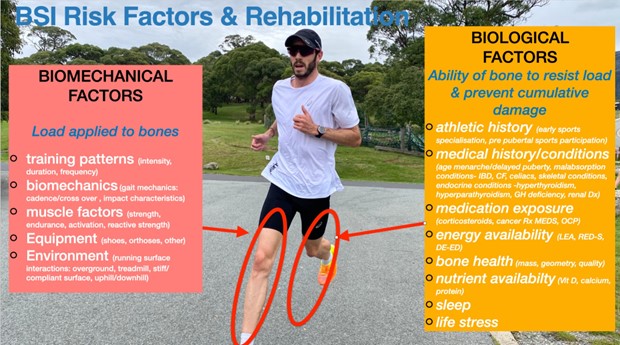
Fig 1. Biological and biomechanical BSI risk factors.
Case Presentation
The patient consented to participate in this case study.
JF, a 22 year old male triathlete presented for assessment of right sided posterior calf pain of five days origin. JF would present to the clinic for athlete monitoring as a Triathlon Australia categorised athlete.
JF’s goal was to represent Australia as an U23 athlete at the World Championships scheduled for four months post the date of symptom onset.
Figure 2 shows symptom location, nature, aggravating, and easing factors. JF described band-like pain in the location of the posterior mid calf. Initial symptoms occurred insidiously 15 minutes into a scheduled 25 minute low intensity run. JF denied any acute mechanism of injury that resulted in the onset of symptoms.
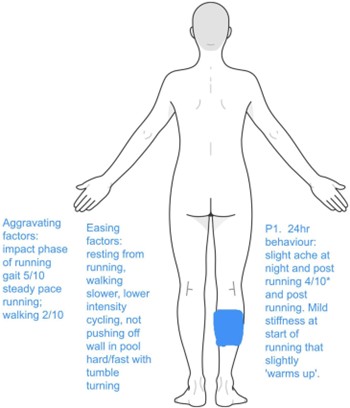
Figure 2. Body Chart *Numerical Pain Rating Scale (NPRS)
Following symptom onset the next day JF completed an intensity run session totalling 7km. JF reported 4/10 pain following this run, described as feeling ‘full’. During a 16 km run 2 days after symptom onset JF stopped 35 minutes into the run experiencing a ‘thudding’ sensation in the posterior calf. JF jogged home at a reduced pace aware of symptoms. Across the next 2 days of training JF experienced 4/10 pain during an 8km training run, and a 35 minute training run that JF cut short due to symptoms at 20 minutes. Following initial warm up JF reported that symptoms increased with further continued minutes of running. This failure to warm up across multiple runs raised clinical suspicion of a potential BSI.
JF had a prior history of lower leg injuries as is shown in Figure 3.
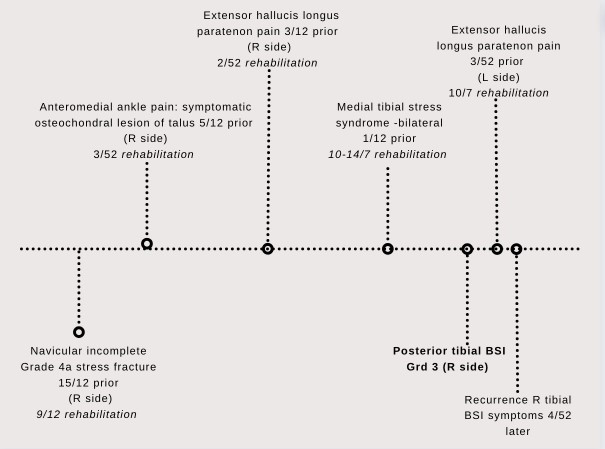
Figure 3. JF lower limb injury history prior to tibial BSI onset
JF reported no general health concerns. No yellow or red flags were obtained through subjective examination. JF had been working with a Sports Dietitian to assist with optimising energy availability (EA) and micro/macronutrient availability in order to optimise bone health following his prior navicular BSI (Barrack et al 2014, Mountjoy et al 2018). Low energy availability (LEA)/relative energy deficiency in sport (RED-s) had been identified as a contributing factor for JF’s prior navicular BSI. There had been no exposure to medications that would impair bone health, nor were any medications being used for the presenting concern. JF’s athletic history consisted of triathlon specialisation from the age of 15 years (Tenforde et al 2011), with rugby league and cricket participation prior. There was no reported family history of BSI including JF’s father who had competed at a high level in long course triathlon across 20 years with no BSI history (Varley et al, 2016).
JF’s weekly training schedule comprised 10-25 hrs of training of swim, bike, run, and strength & conditioning sessions. JF’s coach emphasised that intensity running had been judiciously and sparingly programmed as a way of reducing known BSI risk (Warden et al 2021) following the prior navicular BSI. Table 1 illustrates the intensity distribution and total volume of running across the 12 month period prior to tibial BSI onset compared with the
same metrics for the 12 months prior to the historical navicular BSI. It can be noted that both overall running volume and intensity running had been significantly less leading into the tibial BSI, however it is well accepted that BSI causation is multifactorial (Hoeing et al, 2022).
Even though JF’s total run workload had been less leading into his tibial BSI, other factors aside from run workload included possible low caloric intake/ energy availability, footwear, run terrain, and regional osteopenia as a corollary to the deload time that was prescribed by the Team Sports Physician.
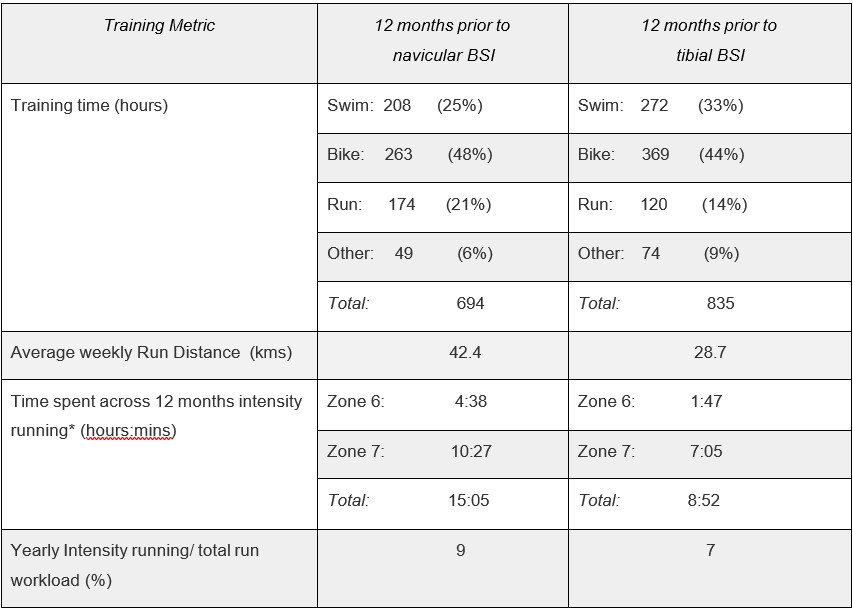
Table 1. Comparative key training metrics 12 months prior to tibial BSI and navicular BSI. [*Intensity running: Zone 6 & 7 heart rate]
Table 2 details key differential diagnoses examination findings.
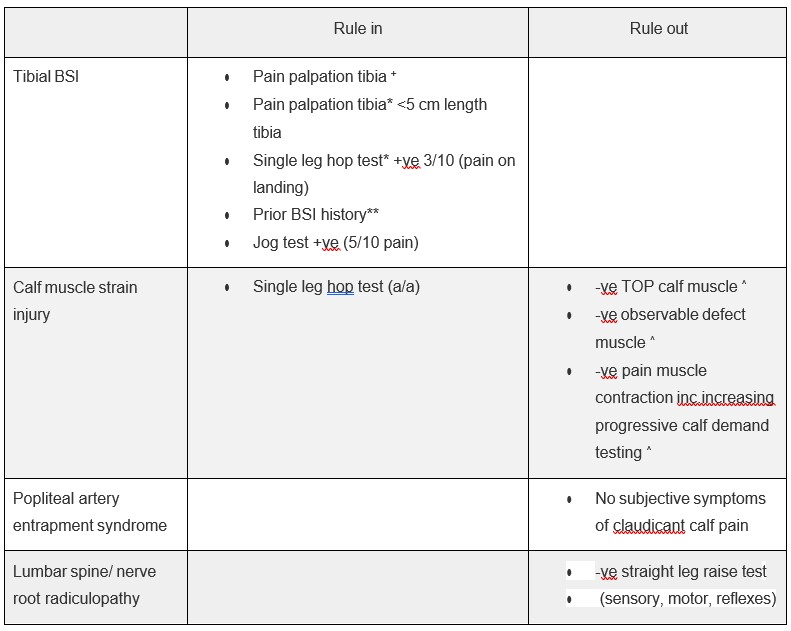
Table 2. Examination right posterior lower leg (^ Green et al 2022, *Milgrom et al 2020, +Yates et al 2004, ** Tenforde et al 2013)
The following was also noted:
- Reduced muscle mass plantar flexors bilaterally (Bennell et al 1996)
- Ankle dorsiflexion ROM (knee to wall test) 10 cm bilaterally
Impression
A provisional diagnosis was made of a tibial BSI. The chief differential diagnosis was that of a soleus muscle strain injury due to the reported insidious onset with low intensity running (Green et al, 2022). Predictive modelling shows that BSI risk for the upcoming season of sport to be 6-8 fold greater for the male athlete who has had a prior BSI (Tenforde et al 2013). JF’s prior navicular BSI heightened the risk of another running related BSI developing (Popp et al, 2021). Knowledge of this elevated risk combined with a positive single leg hop test which has been shown to be an excellent screening tool for tibial BSI with no false negatives (Milgrom et al 2020), added weight to the suspicion of a tibial BSI.
JF underwent MR imaging (Nattiv et al 2013) for his posterior tibial pain the same day as he initially presented for assessment. Radiology reported that JF had incurred a posteromedial mid diaphyseal tibial bone stress injury consistent with a Grade 3 BSI (Fredericson Scale, [Tenforde, et al 201] ), see Figure 4. The posterior location of injury was of clinical interest as posterior tibial BSI tend to present less commonly than posteromedial symptoms.
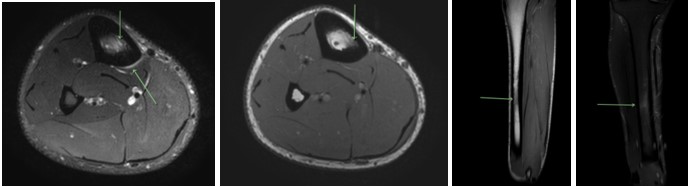
Figure 4. MRI imaging posterior tibial BSI (T1 & T2 weighted images)
Management
The management approach for JF’s tibial BSI combined an optimal loading approach (Warden et al 2021), with a radiology informed (Nattiv et al 2013) deload period aimed at resolving symptoms and returning to sport in a safe and timely manner. Risk factors identified through the assessment were targeted as part of the rehabilitation. Primarily these included optimising EA and micro/macronutrient availability for bone health, and run workload load monitoring. Return to run programming incorporated strategies to reduce bone workload using advances in bone science (Warden et al 2021, Hegedus et al 2023).
JF’s rehabilitation goals were to minimise training time and cardiovascular fitness loss due to injury, return to running safely, and ultimately to return safely to national and international U23 elite triathlon competition.
The stages of JF’s rehabilitation are outlined below:
0-2 weeks
Given JF’s injury history and the known heightened risk of incurring a further BSI (Tenforde et al 2013), a traditional time based deloading approach of minimum 6 weeks non impact loading was recommended (Swenson et al 1997). Following this initial deload period an optimal loading approach (Warden et al 2021) was used to guide rehabilitation progression and decision making. JF was placed in a CAM walker boot non weight bearing for week 1, and partial weight bearing with CAM boot for week 2. The aim being to optimise early BSI healing and achieve pain free gait and activities of daily living (ADLs) as soon as possible.
JF was advised to continue swim training with modifications (no kicking, wall pushing, or fins) in order to maintain cardiopulmonary fitness (Fredericson et al 1995). JF was advised to cease cycling in order to reduce the bone loading effect of calf muscle contractions.
2-6 weeks
After 2 weeks JF was pain free with walking and ADL’s. In aiming to keep cumulative bone loading low to optimise early bone healing, JF was advised to limit ambulation beyond ADL’s for weeks 3-4. JF was advised to use rocker bottom cushioned shoes with orthoses to assist with dissipation of internal bone loads and reduce plantar flexor demands (Ekenman et al 2002, Milgrom et al 2001, Sinclair et al 2016). JF commenced low intensity aerobic cycling not exceeding 30-40% of typical weekly volume aimed at limiting cardiovascular fitness losses. Swim training continued with recommencement of kicking and pushing off the wall.
For weeks 1- 4 weeks post injury JF ceased performing strength exercises on his affected leg as a way of reducing muscle contractions and optimising healing time-frames (Warden et al 2021). JF continued with home and gym based leg strength exercises for the unaffected leg in order to promote a cross training strength effect for the injured leg (Carrol et al 2006). The home exercise program (HEP) included osteogenic bone loading exercises for the unaffected leg in order to reduce downregulation of skeletal health that can accompany deloading (Popp et al 2021). Progressive plantar flexor strength exercises commenced from week 2 for the HEP, and from week 5 in the gym under the supervision of a strength & conditioning coach. Hamstring curls were delayed due to the potential tensile loading effect on the posterior tibia until week 6 onwards (Warden et 2021).
JF was advised that the return to run program could commence when the following criteria were met: pain free for 5 days consecutively with ADLs, perform a series of single leg hops without pain, and able to complete dedicated 30-45 minute walks with no symptoms.
6 weeks
At 6 weeks JF was able to complete both ADL and dedicated walking without concern. JF had been swimming and cycling with reduced volume but tolerating progressive intensity. JF consulted a Sports Dietitian who reviewed caloric availability, increased protein intake to 140gm per day, and recommended updated bloodwork. Blood testing was facilitated through a Sports Physician with surrogate indicators of RED-S including iron studies and sex hormone profile all returning normal values (Mountjoy et al 2018). On examination however JF reported 2-3/10 pain at the site of the diagnosed BSI on single leg hop testing. A further 2 weeks of non impact loading was recommended.
8 weeks +
By 8 weeks of non impact loading return to run criteria were satisfied. JF was categorised as moderate risk on the RED-S Clinical Assessment Tool (RED-S CAT) for returning to participation (running) due to a prior history of one BSI that had low energy availability as a driver. The RED-S CAT requires a moderate risk athlete’s return to participation to be under the guidance of a medical team (Mountjoy et al 2015).
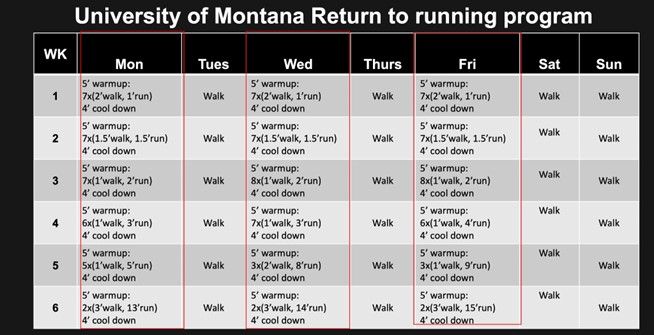
Progressive walk-run programs are standard for returning an athlete with a low risk BSI to running (Warden et al 2021). Table 3 outlines JF’s return to run program (Willy 2023). JF had successfully returned from prior navicular BSI utilising a similar walk-jog progression. The intensity of running was advised to be low in order to reduce bone workload and minimise the risk of creating bone fatigue (Warden et al 2021). JF and coach were reminded that all sessions needed to be symptom free both during and post.
10 weeks +
JF continued to progress through the return to run program, returned to normal swim training workload, while continuing to build cycling workload. A focus on addressing calf muscle mass was a key aim for strength and conditioning (HEP and gym) due to the known risk of reduced muscle mass on BSI (Warden et al 2021). Osteogenic bone loading exercises were added for the symptomatic leg from week 10 onwards (Warden et al 2021). These exercises included countermovement jumps progressing along a continuum of difficulty to single leg deadlift jumps.
12 weeks +
JF reported a 3/10 ‘throbbing’ pain in the posterior mid diaphyseal region of his right tibia, consistent with the original site of injury after completing the final run of week 4 (see Table 3). On examination a 2 cm region of posterior tibia was painful to palpate raising the strong suspicion of recurrent tibial bone stress symptoms (Milgrom et al 2020). Triathlon Australia’s Sports Physician ordered an MRI of the tibia which revealed a periosteal reaction and subtle bone marrow oedema of the mid tibia posteriorly (Grade 2 Fredericson scale). JF was advised to deload the symptomatic leg for a 2 week period of CAM boot use and PWB with crutches.
Given JF’s recurrence of symptoms 4 weeks into the return to run program a bone mineral density (BMD) assessment was performed via a DXA scan. Z-scores (<50yr age athlete) were within normal ranges (AP Spine L1-4 Z-score 0.1, Femur Total Left Z -score 1.4, Femur Total Right Z-score 1.6).
Rehabilitation was planned for completion at around 20 weeks post injury diagnosis. This would allow for 8 weeks to return to running, and a further 12 weeks to build up to safe and repeatable run workouts that incorporated intensity.
Discussion
The assessment and management of JF’s BSI was consistent with evidence-informed practices (Hoeing et al 2022, Warden et al 2021). Interventions were individualised and a long term BSI risk mitigation program was established for JF. The program comprised: regular sports dietetic monitoring (Mountjoy et al 2018), strength and conditioning targeting osteogenic bone loading and kinetic chain enhancements (Warden et al 2021), and run workload periodisation to assist with skeletal mechanosensitivity (Warden et 2021). As a season progresses for distance runners, skeletal mechanosensitivity reduces elevating BSI risk (Krabak et al 2019, Warden et al 2020). As such JF is to be scheduled ongoing for 1 week of no running following every 12 weeks of run training. This ‘skeletal reset’ week is to serve as a strategy for improving skeletal mechanosensitivity and conceptually decreasing BSI risk (Warden et al 2021).
The re-emergence of symptoms raised clinical suspicion that JF may have developed some deload induced regional osteopenia in his symptomatic leg. Clinical suspicion was heightened given the extensive deload period required for rehabilitation of the prior navicular stress fracture. While the BMD examination scores were within normal limits, one interesting finding was that there was a larger relative reduction in BMD for the symptomatic leg (-1.6% Z-score change for Femur Total) compared with the unaffected leg (Femur Total Z-score change of +0.2%) compared with prior BMD assessment performed 17 months earlier.
However one limitation of BMD assessment being that local BMD of the tibia itself is not specifically assessed.
On reflection repeat MR imaging could have been ordered before the recommencement of running. This did not occur as JF cleared established return to run criteria (Warden et al 2021). It took 8 weeks to return to running under the optimal loading management approach used to manage JF’s injury. This is consistent with the generally accepted deload periods for
a Grade 3 Fredericson Scale BSI of the tibia (Nattiv et al 2013). This case is an example of the optimal loading approach to managing low risk BSI not necessarily returning athletes to running sooner than a traditional time based deload period (Warden et al 2021).
On further reflection:
- Extracorporeal shockwave therapy (ESWT) could have been used to potentially accelerate healing (Schmitz et al 2015, Beling et al 2023, Hoeing et al 2022).
- A gait analysis could be performed as a means of potentially reducing bone loading, through cadence optimisation, and screening for cross over gait (Willy 2023, Warden et al 2021).
- AlterG anti-gravity treadmill could have been used in return to run programming which commenced 8 weeks post injury . The Alter-G reduces bone workloads through the reduction of impact forces and shortened ground contact times (Harrast 2020).
- Education regarding the effect of sleep quality on BSI risk could also have been conducted (Tenforde et al, 2022)
Conclusion
This case study illustrates the complex interplay in causation and recovery from a low risk tibial BSI. The recurrence of symptoms highlights the complexity of managing BSI. The case study reinforces the role that multidisciplinary teams play in the management of BSI. Clinicians need to utilise a comprehensive and individualised strategy when rehabilitating BSI in the running athlete guided by the findings of comprehensive risk factor analysis.

Brad Beer
APA Titled Sports & Exercise Physiotherapist (APAM), POGO Founder
Book an Appointment with Brad here.
Featured in the Top 50 Physical Therapy Blog
References
- Barrack MT, Gibbs JC, De Souza MJ, Williams NI, Nichols JF, Rauh MJ, Nattiv A. Higher incidence of bone stress injuries with increasing female athlete triad-related risk factors: a prospective multisite study of exercising girls and women. Am J Sports Med. 2014 Apr;42(4):949-58. doi: 10.1177/0363546513520295. Epub 2014 Feb 24. PMID: 24567250.
- Beling A, Saxena A, Hollander K, Tenforde AS. Outcomes Using Focused Shockwave for Treatment of Bone Stress Injury in Runners. Bioengineering (Basel). 2023 Jul 25;10(8):885. doi: 10.3390/bioengineering10080885. PMID: 37627770; PMCID: PMC10451564.
- Bennell KL, Malcolm SA, Thomas SA, Reid SJ, Brukner PD, Ebeling PR, Wark JD. Risk factors for stress fractures in track and field athletes. A twelve-month prospective study. Am J Sports Med. 1996 Nov-Dec;24(6):810-8. doi: 10.1177/036354659602400617. PMID: 8947404.
- Carroll TJ, Herbert RD, Munn J, Lee M, Gandevia SC. Contralateral effects of unilateral strength training: evidence and possible mechanisms. J Appl Physiol (1985). 2006 Nov;101(5):1514-22. doi: 10.1152/japplphysiol.00531.2006. PMID: 17043329.
- Ekenman I, Milgrom C, Finestone A, Begin M, Olin C, Arndt T, Burr D. The role of biomechanical shoe orthoses in tibial stress fracture prevention. Am J Sports Med. 2002 Nov-Dec;30(6):866-70. doi: 10.1177/03635465020300061801. PMID: 12435654.
- Feldman JJ, Bowman EN, Phillips BB, Weinlein JC. Tibial Stress Fractures in Athletes. Orthop Clin North Am. 2016 Oct;47(4):733-41. doi: 10.1016/j.ocl.2016.05.015. PMID: 27637660.
- Fredericson M, Bergman AG, Hoffman KL, Dillingham MS. Tibial stress reaction in runners. Correlation of clinical symptoms and scintigraphy with a new magnetic resonance imaging grading system. Am J Sports Med. 1995 Jul-Aug;23(4):472-81. Doi: 10.1177/036354659502300418. PMID: 7573660.
- Fredericson M, Jennings F, Beaulieu C, Matheson GO. Stress fractures in athletes. Top Magn Reson Imaging. 2006 Oct;17(5):309-25. doi: 10.1097/RMR.0b013e3180421c8c. PMID: 17414993.
- Green B, McClelland JA, Semciw AI, Schache AG, McCall A, Pizzari T. The Assessment, Management and Prevention of Calf Muscle Strain Injuries: A Qualitative Study of the Practices and Perspectives of 20 Expert Sports Clinicians. Sports Med Open. 2022 Jan 15;8(1):10. doi: 10.1186/s40798-021-00364-0. PMID: 35032233; PMCID: PMC8761182.
- Harrast, MA. Clinical Care of the Runner. Assessment, Biomechanical Principles, and Injury Management. Elsevier; 2020.
- Hegedus EJ, Mulligan EP, Beer BA, Gisselman AS, Wooten LC, Stern BD. How Advancement in Bone Science Should Inform the Examination and Treatment of Femoral Shaft Bone Stress Injuries in Running Athletes. Sports Med. 2023 Jun;53(6):1117-1124. doi:
10.1007/s40279-022-01802-z. Epub 2023 Jan 4. PMID: 36598744. - Hoenig T, Ackerman KE, Beck BR, Bouxsein ML, Burr DB, Hollander K, Popp KL, Rolvien T, Tenforde AS, Warden SJ. Bone stress injuries. Nat Rev Dis Primers. 2022 Apr 28;8(1):26. doi: 10.1038/s41572-022-00352-y. PMID: 35484131.
- Krabak BJ, Tenforde AS, Davis IS, Fredericson M, Harrast MA, d’Hemecourt P, Luke AC, Roberts WO. Youth Distance Running: Strategies for Training and Injury Reduction. Curr Sports Med Rep. 2019 Feb;18(2):53-59. doi: 10.1249/JSR.0000000000000564. PMID: 30730342.
- Lopes AD, Hespanhol Júnior LC, Yeung SS, Costa LO. What are the main running-related musculoskeletal injuries? A Systematic Review. Sports Med. 2012 Oct 1;42(10):891-905. doi: 10.1007/BF03262301. PMID: 22827721; PMCID: PMC4269925.
- Milgrom C, Finestone A, Ekenman I, Simkin A, Nyska M. The effect of shoe sole composition on in vivo tibial strains during walking. Foot Ankle Int. 2001 Jul;22(7):598-602. doi: 10.1177/107110070102200713. PMID: 11503988.
- Milgrom C, Zloczower E, Fleischmann C, Spitzer E, Landau R, Bader T, Finestone AS. Medial tibial stress fracture diagnosis and treatment guidelines. J Sci Med Sport. 2021 Jun;24(6):526-530. doi: 10.1016/j.jsams.2020.11.015. Epub 2020 Dec 3. PMID: 33298373.
- Mountjoy M, Sundgot-Borgen J, Burke L, Carter S, Constantini N, Lebrun C, Meyer N, Sherman R, Steffen K, Budgett R, Ljungqvist A, Ackerman K. The IOC relative energy deficiency in sport clinical assessment tool (RED-S CAT). Br J Sports Med. 2015 Nov;49(21):1354. PMID: 26764434.
- Mountjoy M, Sundgot-Borgen JK, Burke LM, Ackerman KE, Blauwet C, Constantini N, Lebrun C, Lundy B, Melin AK, Meyer NL, Sherman RT, Tenforde AS, Klungland Torstveit M, Budgett R. IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Br J Sports Med. 2018 Jun;52(11):687-697. doi: 10.1136/bjsports-2018-099193. PMID: 29773536.
- Nattiv A, Kennedy G, Barrack MT, Abdelkerim A, Goolsby MA, Arends JC, Seeger LL. Correlation of MRI grading of bone stress injuries with clinical risk factors and return to play: a 5-year prospective study in collegiate track and field athletes. Am J Sports Med. 2013 Aug;41(8):1930-41. doi: 10.1177/0363546513490645. Epub 2013 Jul 3. PMID: 23825184; PMCID: PMC4367232.
- Popp KL, Ackerman KE, Rudolph SE, Johannesdottir F, Hughes JM, Tenforde AS, Bredella MA, Xu C, Unnikrishnan G, Reifman J, Bouxsein ML. Changes in Volumetric Bone Mineral Density Over 12 Months After a Tibial Bone Stress Injury Diagnosis: Implications for Return to Sports and Military Duty. Am J Sports Med. 2021 Jan;49(1):226-235. doi: 10.1177/0363546520971782. Epub 2020 Dec 1. PMID: 33259223.
- Schmitz C, Császár NBM, Milz S, et al. . Efficacy and safety of extracorporeal shock wave therapy for orthopaedic conditions: a systematic review on studies listed in the PEDro database. Br Med Bull. 2015;116:115–138.
- Sinclair J, Richards J, Selfe J, Fau-Goodwin J, Shore H. The Influence of Minimalist and Maximalist Footwear on Patellofemoral Kinetics During Running. J Appl Biomech. 2016 Aug;32(4):359-64. doi: 10.1123/jab.2015-0249. Epub 2016 Mar 8. PMID: 26959346.
- Swenson JE, DeHaven KE, Sebastianelli WJ, et al. The effect of a pneumatic leg brace on return to play in athletes with tibial stress fractures. Am J Sports Med. 1997;25:322–328.
- Tenforde AS, Fredericson M. Bone Stress Injuries. Diagnosis, Treatment, and Prevention. [1st Edition.] New York Demos Medical; 2022.
- Tenforde AS, Fredericson M. Influence of sports participation on bone health in the young athlete: a review of the literature. PM R. 2011 Sep;3(9):861-7. doi: 10.1016/j.pmrj.2011.05.019. PMID: 21944303.
- Tenforde AS, Kraus E, Fredericson M. Bone Stress Injuries in Runners. Phys Med Rehabil Clin N Am. 2016 Feb;27(1):139-49. doi: 10.1016/j.pmr.2015.08.008. PMID: 26616181.
- Tenforde AS, Sayres LC, McCurdy ML, Sainani KL, Fredericson M. Identifying sex-specific risk factors for stress fractures in adolescent runners. Med Sci Sports Exerc. 2013 Oct;45(10):1843-51. doi: 10.1249/MSS.0b013e3182963d75. PMID: 23584402.
- Varley I, Greeves JP, Sale C, Friedman E, Moran DS, Yanovich R, Wilson PJ, Gartland A, Hughes DC, Stellingwerff T, Ranson C, Fraser WD, Gallagher JA. Functional polymorphisms in the P2X7 receptor gene are associated with stress fracture injury. Purinergic Signal. 2016 Mar;12(1):103-13. doi: 10.1007/s11302-016-9495-6. Epub 2016 Jan 29. PMID: 26825304; PMCID: PMC4749527.
- Willy R . Restoring Load Capacity to the Injured Runner Course. Melbourne, Australia 22-23rd April, 2023.
- Yates B, White S. The incidence and risk factors in the development of medial tibial stress syndrome among naval recruits. Am J Sports Med. 2004 Apr-May;32(3):772-80. doi: 10.1177/0095399703258776. PMID: 15090396.



