


Navicular bone stress injuries are injuries not to be missed. Navicular bone stress injuries (BSI) carry a substantive greater risk of non union for stress fractures and frank fractures, and delayed healing for bony stress reactions of the navicular.
Navicular bone stress injuries account for 14-35% of all foot and ankle bone stress injuries, with the injury being common to track and field, and jumping sports such as basketball.
Clinically I have seen athletes across a variety of sports present with navicular bone stress injuries, however with my clinical bias being towards the running based endurance athlete that is where my greatest experience in the diagnosis of and subsequent treatment of navicular BSI has been garnered.
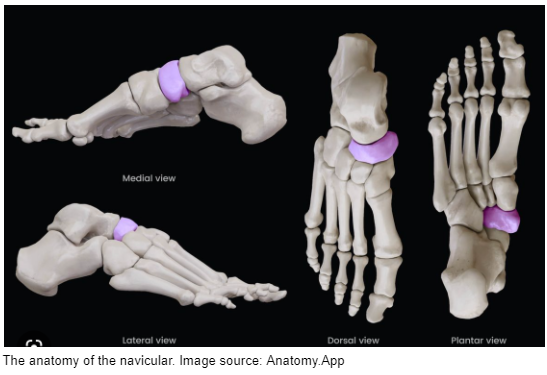
Anatomy of the navicular
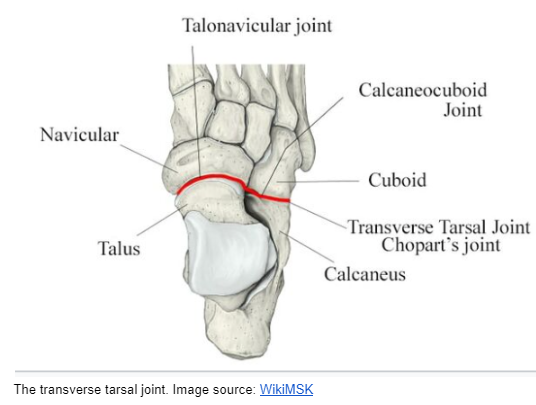
The navicular articulates with the talus, cuboid, and cuneiforms (see below). The navicular, talus, cuboid, and calcaneus make up the transverse tarsal joint. The transverse tarsal joint (also known as chopart’s joint) is made up of the talonavicular and calcaneocuboid joints, serving to separate the rearfoot from the midfoot.
Biomechanics of the navicular
The mechanics of the navicular bone provide an insight into the potential risk of BSI for this region of the runner’s skeleton. The navicular and transverse tarsal joint play important roles in allowing the foot to transition from a flexible structure -that allows the foot to absorb impact forces as it strikes the ground, to the rigid structure required for efficient toe off with gait (1).
Likewise the medial arch of the foot is supported by talonavicular structures. There is a delicate interplay between the passive support structures and muscle control across the transverse tarsal joint. In forefoot pronation the navicular has greater mobility. When the forefoot is in supination the navicular is in a closed pack position. When the heel is inverted as a result of the pull of the tibialis posterior and its associated tendon (ie hindfoot is supinated) the transverse tarsal joint becomes rigid in preparation for toe off, resulting in compression of the navicular. It is during this toe off phase when the internal bone loads of the navicular bone are the greatest, with a zone of tensile loading through the middle one -third of the navicular body and doming of the navicular superiorly.
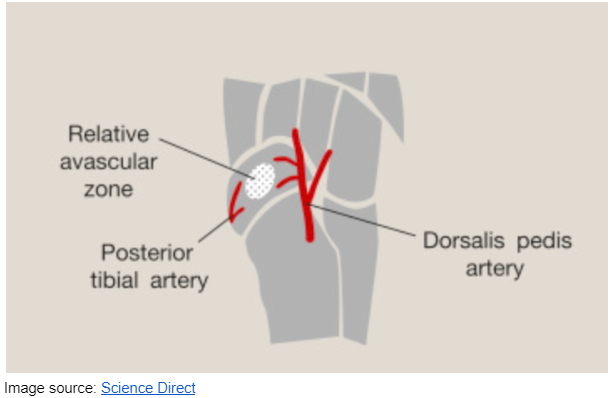
In conjunction with this high region of loading in the central third of the navicular it is also known that the central third of the navicular is a watershed area with poor arterial blood supply, heightening this region’s risk of developing a bone stress injury. This region corresponds to the most common site of stress fracture in the navicular. This watershed area of the navicular body makes the risk of nonunion or delayed union a risk for navicular stress fractures and bone stress injuries. For this reason the bone stress injuries to the navicular are considered high risk, making astute clinical management of the condition essential.
Risk factors for navicular bone stress injury
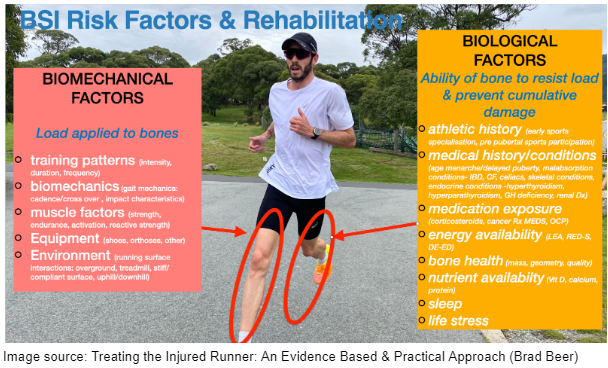
As with all running related bone stress injuries, risk factors can be divided into two categories: biological and biomechanical risk factors. Biological risk factors determine the health and ability of a runner’s skeleton to be loaded, while biomechanical risk factors include those factors that moderate the loading applied to the runner’s skeletal system. Biological and biomechanical risk factors are depicted below.
Specifically for the navicular Mandell et. al. (8) outlined patho-anatomical risk factors for navicular bone stress injuries to be: reduced ankle dorsi-flexion, cavus foot structure, and a morton foot structure. Corticosteroid use, Vitamin D insufficiency, and Relative Energy Deficiency in Sport (RED-S) were also listed as navicular bone stress injury risk factors.
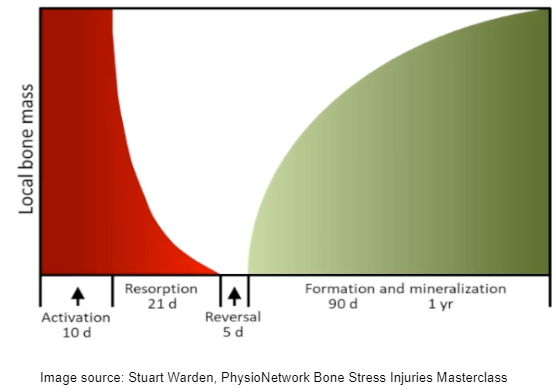
In particular attention needs to be given to training patterns of the runner who develops a navicular BSI. Training errors are typically involved whereby the error will occur approximately four weeks before symptoms may be experienced. This is due to a three week resorption phase of osteoclasts following bone loading compared with 3 months of bone formation time, which creates a window of ‘vulnerability’ for bone injury. If a runner has accrued microdamage (out paced normal bone targeted remodelling due to an increase in bone workload) and associated porosity around a microcrack that region may be susceptible to heightened bone stress/strain and subsequent pathology. Hence reviewing the training diary of a runner who presents with a navicular BSI, four weeks before symptom onset can often reveal a change in bone workload that may have contributed to injury onset. Keep a particular eye out for the amount/ or change in intensity running which carries with it heightened BSI risk.
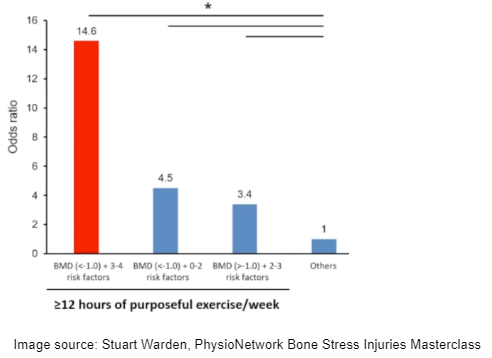
Biologically one of the most important risk factors to not miss is the injured athlete’s energy availability (EA). It is well established that states of low energy availability (LEA) heighten the risk of BSI through the resultant direct and indirect down regulatory effects on skeletal health. LEA is the key driver for relative energy deficiency in sports (RED-S) whereby athletes experience heightened BSI risk. In the presence of 2-3 risk factors for RED-S (menstrual dysfunction oligo-amenorrhea, elevated dietary restraint, participation in leanness sport, low BM1 < 21 kg/msq, ) female athletes who train > 12 hours week 3x risk of BSI independent of bone health.But when 3-4 risk factors are combined w low bone health (BMD<1.0) 15.6x more likely BSI (2).
Navicular specific risk factors may include a log 2nd ray, reduction in ankle dorsiflexion, a cavus foot, and stiffness in the subtalar joint (3).
Diagnosis of Navicular BSI
Runners with navicular bone stress injury will present with pain over the dorsum of the foot in the region of the navicular. The pain tends to be distributed and vague as opposed to a pin point location. The N-spot may be tender to palpate however the diagnostic value of this has not been scientifically determined. The N-spot is lateral to the tibialis anterior tendon but medial to the extensor hallucis tendon in the central region of the dorsum of the navicular (see below).

https://www.facebook.com/watch/?v=981190279237990
Loading the foot with running or hopping will typically produce pain. Single leg calf raises may also elicit pain in the region of the navicular
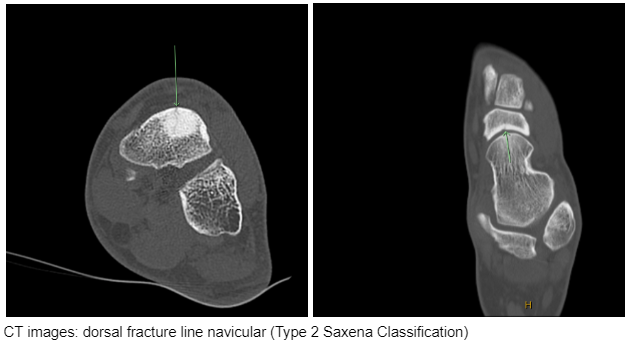
Imaging for suspected navicular bone stress imaging is key. Plain film radiographs (x-rays) have low sensitivity for detecting navicular bone stress injury, hence an MRI is key. While MRI is great at detecting bone stress MR may not be sensitive enough to detect cortical fractures. The sensitivity of MR imaging for navicular fracture has been reported as being 71.4% (4). A CT scan should be performed if there is suspicion of a navicular stress fracture following MR imaging. Repeat CT imaging may be indicated to evaluate fracture healing and union.

Classification of navicular stress fractures
In 2000 Saxena and colleagues (5) proposed a 3 tiered classification system of navicular stress fractures:
- Type I fractures occur on the dorsal side of the navicular.
- Type II fractures propagate into the navicular body
- Type III fractures extend to the opposite cortex
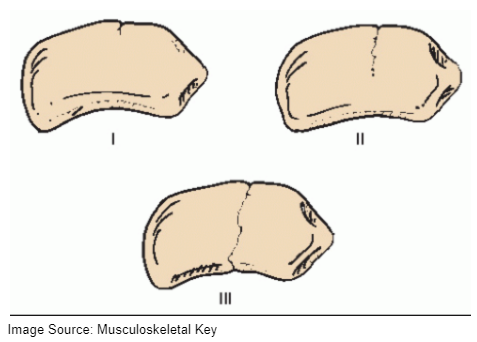
These three fracture types also involve modifiers including avascular necrosis (A), cystic changes to the fracture line (C) , and sclerosis of the fracture line (S).
Saxena et al (4) reported that Type I were most likely to receive conservative management, while Type III fractures took a greater time to heal than fracture types I & II. Type I fractures has an average return to activity of 3 months while Type II’s return to activity was 3.6 months. Meanwhile Type III fractures has a return to activity timeline of 6.8months. Surgery is indicated for Type II and III fractures particularly if modifiers are present.
Treatment
Conservative pathway
In order to optimise healing and decrease the risk of nonunion or associated possible sequelae, non weight bearing (NWB) for a minimum of 6 weeks is recommended. High CAM walker use is also strictly recommended-as they infer more stiffness for the lower leg, while keeping the talo-crural joint in neutral.
Partial weight bearing is associated with a high rate of nonunion or delayed bone union.
Research was performed in 2010 by Torg et al. which highlighted that less than 50% who were treated with partial weight bearing had successful returns to sport (6). The return to play timelines being 5.7months. This partial weight bearing approach was inferior compared with intervention that comprised 6 weeks of strictly no weight bearing in a cast, whereby the return to sport timelines were much shorter 3.7months and the success rate much greater 96% compared with the partial weight bearing group.
Surgical pathway
A surgical approach can be indicated when there is evidence of a displaced fracture, or avascular necrosis of the navicular. Meanwhile surgical intervention may furthermore be indicated when there is a recurrence of the fracture, non union, or a complete fracture (Type 3), or in the instance of an elite athlete who needs to minimise time loss.
Surgically percutaneous screw fixation can be performed for partial and non displaced fractures. Bone grafts may be required where there is sclerotic bone or fracture displacement, or avascular necrosis Hardware may be removed in some patients at or around 12 months post surgery.
Torg’s meta analysis (6) reported that 82% of patients had a successful outcome post surgery.
Post surgically rehabilitation requires 6 weeks non weight bearing in a tall CAM walker boot. Weight bearing as tolerated can commence from 6 weeks post surgery, with progressive strength and conditioning progressing from 6 weeks post surgery also.
Consideration and treatment of all possible BSI drivers (biomechanical and biological) is key while the athlete is recovering in the boot. This may include an assessment with a sports dietitian to ascertain and ensure sufficient energy and nutrients are available to the athlete.
Exercise therapy should focus on a progressive return to plantar flexor loading on the symptomatic side once the athlete is able to weight bear without a moon boot with nil aide. Plantar flexors (calf) exercises should be indexed up gradually from seated deload single leg calf raises , through until heavy loaded single leg calf raises which may commence once satisfaction of the bone stress injury or fracture has been arrived at (clinical signs and /or imaging results as indicated). In addition to calf exercise work, the remainder of the running kinetic chain can be targeted in a home and gym based exercise program. Exercises for the kinetic chain may include contralateral leg work while the athlete is healing their navicular BSI (this can include above and below knee single leg exercises), ahead of progressive programming for compound movements such as loaded barbell back squats and deadlifts, and finally progressive plyometric exercise prescription throughout mid-late stage rehabilitation. Standing calf raises may begin at around 8 weeks post injury. Return to running may commence at around 12 weeks if the athlete is void of pain on single leg hopping and has satisfactory healing on repeat CT imaging.
It is important to incorporate some single leg hopping (of various forms eg forwards, side to side, up onto a step etc) for the asymptomatic leg in order to enhance bone mineral density/ bone health in the unaffected leg. One of the known corollaries of significant deload periods for the skeleton can be regional bone density losses of up to 33% when an injury and subsequent deloading occurs, such as with navicular BSI. Incorporating single leg hopping over the healing months may serve to offset/reduce some bone health deficits in the opposite leg of the athlete.
Return to Run principles to note include:
- Commence with a walk/jog program and establish up to 30 mins accrued steady state jogging for example of a 4-6 week period.
- Utilise body weight supported running options if available such as the AlterG anti-gravity treadmill. (Rehabilitating running injuries with body weight supported treadmills-blog)
- Re-establish running minutes /volume/loading cycles first ahead of introducing intensity running later in the rehabilitation journey. Intensity running indexes greater risk for BSI, particularly a bone like the navicular.
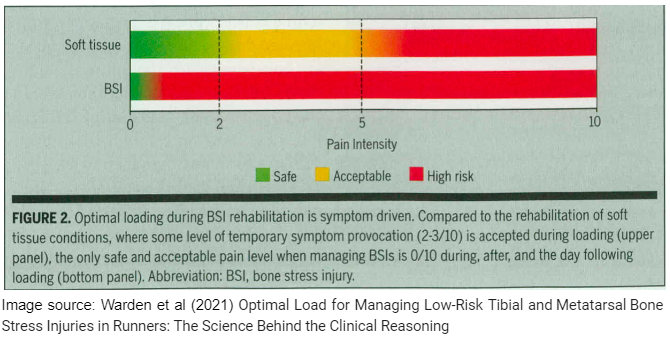
- Load monitoring with return to run programs should be pain free. Warden et al paper (2021) (7) outlines that with BSI return to run programming the aim is to not experience any soreness in the bone on return. If there is any soreness Warden et al recommend ceasing running for 3 days, and then resuming by regressing 1 week on the progressive return to run program.

Brad Beer
APA Titled Sports & Exercise Physiotherapist (APAM), POGO Founder
Book an Appointment with Brad here.
Featured in the Top 50 Physical Therapy Blog
References
- Sammarco VJ. The talonavicular and calcaneocuboid joints: anatomy, biomechanics, and clinical management of the transverse tarsal joint. Foot Ankle Clin. 2004 Mar;9(1):127-45. doi: 10.1016/S1083-7515(03)00152-9. PMID: 15062218.
- Barrack MT, Gibbs JC, De Souza MJ, Williams NI, Nichols JF, Rauh MJ, Nattiv A. Higher incidence of bone stress injuries with increasing female athlete triad-related risk factors: a prospective multisite study of exercising girls and women. Am J Sports Med. 2014 Apr;42(4):949-58. doi: 10.1177/0363546513520295. Epub 2014 Feb 24. PMID: 24567250.
- Pavlov, H., Torg, J. S., & Freiberger, R. H. (1983). Tarsal navicular stress fractures: radiographic evaluation. Radiology, 148(3), 641-645.
- Saxena, A., Behan, S. A., Valerio, D. L., & Frosch, D. L. (2017). Navicular stress fracture outcomes in athletes: analysis of 62 injuries. The Journal of Foot and Ankle Surgery, 56(5), 943-948.
- Saxena A, Fullem B, Hannaford D. Results of treatment of 22 navicular stress fractures and a new proposed radiographic classification system. J Foot Ankle Surg. 2000;39:96–103.
- Torg JS, Moyer J, Gaughan JP, Boden BP. Management of tarsal navicular stress fractures: conservative versus surgical treatment: a meta-analysis. Am Journal Sports Med. 2010; 38:1048-1053.
- Warden SJ, Edwards WB, Willy RW. Optimal Load for Managing Low-Risk Tibial and Metatarsal Bone Stress Injuries in Runners: The Science Behind the Clinical Reasoning. J Orthop Sports Phys Ther. 2021 Jul;51(7):322-330. doi: 10.2519/jospt.
- 2021.9982. Epub 2021 May 7. PMID: 33962529.
- Mandell JC, Khurana B, Smith SE. Stress fractures of the foot and ankle, part 2: site-specific etiology, imaging, and treatment, and differential diagnosis. Skeletal Radiol. 2017 Sep;46(9):1165-1186. doi: 10.1007/s00256-017-2632-7. Epub 2017 Mar 25. PMID: 28343329.




