


The big toe is a common site of forefoot pain from acute injury or a gradual onset. The big toe termed ‘hallux’ serves an extremely important role for the stability of the foot and ankle. During standing, it assists to provide a solid base of support. During walking and running, the foot must be stable at foot-strike then during mid-support, the foot must become a mobile adaptor and attenuate loads (McKeon 2014). As we move into push-off the foot must again become stable to deliver force through the big toe and off the ground. Here we discuss some of the common causes of acute and long standing big toe pain and management including turf toe, bunions, sesamoiditis, bone stress injury and more.
Anatomy and Function
The big toe or hallux is composed of 2 bones, the proximal phalanx and distal phalanx. The base of the big toe (proximal phalanx) then connects to the 1st metatarsal at a joint termed the 1st metatarsophalangeal joint (MTPJ). On the underside of this joint are 2 small bones called sesamoids which are embedded within a key toe flexor muscle – flexor hallucis brevis (FHB). The medial or tibial sesamoid is on the inside of the foot, whilst the fibular sesamoid is closer to toes 2-5. These bones function to protect the FHB tendon, absorb weight bearing load on the inside of the forefoot and increase the mechanical advantage for the intrinsic muscles of the big toe.


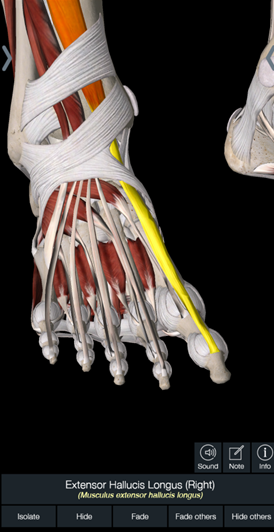


The big toe has multiple muscular attachments including the flexor hallucis longus (pushes the big toe towards the ground along with FHB), extensor hallucis longus (lifts the big toe) and abductor hallucis (pulls the big toe away from the lesser toes).
A good challenge is to attempt to do these actions independently without moving the other toes. Across the plantar surface of the foot is a fibrocartilaginous pad called the plantar plate which connects with the joint capsule surrounding the proximal phalanx and 1st metatarsal. During running the big toe, its ligamentous structures, capsule and surrounding muscles contribute to providing a rigid structure to deliver force from the calf and lower leg into the ground, known as the windlass mechanism.
Common Injuries:
Fractures
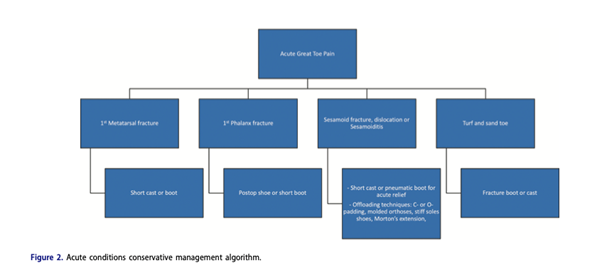
The distal phalanx is a common fracture site from crushing type injuries or stubbing type injuries (1). Stubbing injuries which when involving more force may damage the interphalangeal joint as well as the distal phalanx. This mechanism may also occur alongside dislocations of the hallux and or intra-articular fractures (fracture along the joint line) (1,2). Mechanism of injury, force and visual signs will assist in suspicion of a fracture. Obvious deformity or point tenderness are also common and If there is significant pain upon compression, a fracture is more likely to be present (2). X-ray or CT can be used to confirm diagnosis and guide management. Typical management for a non-displaced, extra-articular fracture is non-surgical with a rigid sole or post-op shoes (3, 4). Any intra-articular fracture, dislocation, or fracture of the metatarsal head should be referred to an orthopaedic surgeon for further evaluation (3, 4).
Turf Toe
Turf toe is used to classify injuries to the hallux plantar capsule, plantar muscles, and the sesamoid complex caused by forceful hyperextension of the great toe (5). Typically, turf toe injuries are most common in athletes and are important to recognise and manage early. Patients typically have pain at the plantar surface of the first MTP joint that tends to increase with passive extension or resisted flexion of the great toe (1, 4). Turf toe injuries will present with pain, swelling and occasional redness at the base of the big toe (1st MTP Joint). Often there is difficulty walking or weight-bearing, and will likely have a history of an inciting injury or event. Pain is worse with localised joint palpation and passive flexion and extension of the great toe (movements done relaxed without active use of the muscles). Turf toe injuries are graded on severity with grade 1 injuries are identified as sprains of the plantar capsular ligament complex (mild), while Grade 2 injuries are characterised by partial rupture of the plantar capsular ligament complex (moderate). Grade 3 injuries are complete tears in the plantar capsular complex/plantar plate along with possible sesamoid fracture, subchondral bruising and or injury to the FHL/FHB muscles (6). Risk factors can include pes planus foot posture, decreased pre-injury big toe and/or ankle dorsiflexion ROM and soft flexible footwear (7).
Management of turf toe injuries is dependent upon grade of injury with grade 1 injuries often having a short reduction in weight bearing or utilising stiff toed shoes until asymptomatic and returning to activity often within a week. Turf toe taping is a common technique used to help protect the toe during return to sport. Grade 2 injuries can be more aggressively offloaded with a CAM boot and crutches if needed, followed by taping to help facilitate return to play over the next 2-4 weeks. Grade 3 injuries should warrant orthopaedic referral especially if additional structures are injured. Depending on severity, surgery may be indicated to repair the plantar plate, including the capsule and ligamentous supports of the 1st metatarsal. It is also important to evaluate the potential of retraction injury to the sesamoids, loose bodies or chondral injury. Non-surgical cases would otherwise require long cast immobilisation in a cast of boot (7) if appropriate. Return to play and sport can be 6-12 weeks dependent on activity and demands of the sport.
Sesamoid Injuries
As described above there are 2 small bones called sesamoids on the plantar side of the first MTPJ. These are embedded within the tendons of the flexor hallucis brevis (FHB). These bones function to protect the FHB tendon, absorb weight bearing load on the inside of the forefoot and increase the mechanical advantage for the intrinsic muscles of the big toe.
Sesamoid injuries include sesamoiditis, fracture (acute or stress fracture) or dislocation. Acute single trauma resulting in fracture or dislocation are typically a large crush force or fall injury onto the forefoot (1). Obvious deformity, tenderness to palpation point to this as a diagnosis and imaging findings (x-ray) help to confirm diagnosis and referral to orthopaedic surgeon for opinion and management.
Sesamoiditis is typically the result of a sudden increase in forefoot loading such as running, jumping or dancing particularly with increased flexion at the first MTPJ (such as wearing heels). When inspecting the area, there is rarely ever any swelling or discoloration. Upon physical examination, there will be poorly localised pain around the MTP joint. In addition, applying direct pressure to the plantar surface over one of the sesamoid bones below the 1st MTP joint will elicit pain and allow the clinician to differentiate between tibial and fibular sesamoid disorders. The picture from Andrews et al shows palpation of the tibial (medial) sesamoid.
 Active or passive flexion and extension of the great toe, as well as resistance to these motions, will not often elicit pain. However, if the examiner applies pressure to the sesamoid and asks the patient to extend the great toe, pain may be produced (1). Plain radiographs will show no signs of fracture in sesamoiditis. Treatment typically involves relative rest from aggravating activity, for runners this may be removing hills, speedwork or running altogether in the short term. Unloading pressure around the sesamoid can be done with podiatry assistance with C- or O-shaped padding, rocker shoes and or moulded orthoses. In some cases there may be benefit from stiff soled shoes, orthotics, or in more symptomatic cases a pneumatic boot. Strength and conditioning around the foot in non-provocative positions can also be completed to assist in restoring strength around the big toe.
Active or passive flexion and extension of the great toe, as well as resistance to these motions, will not often elicit pain. However, if the examiner applies pressure to the sesamoid and asks the patient to extend the great toe, pain may be produced (1). Plain radiographs will show no signs of fracture in sesamoiditis. Treatment typically involves relative rest from aggravating activity, for runners this may be removing hills, speedwork or running altogether in the short term. Unloading pressure around the sesamoid can be done with podiatry assistance with C- or O-shaped padding, rocker shoes and or moulded orthoses. In some cases there may be benefit from stiff soled shoes, orthotics, or in more symptomatic cases a pneumatic boot. Strength and conditioning around the foot in non-provocative positions can also be completed to assist in restoring strength around the big toe.
In runners and jumping athletes or other athletes where there is repetitive forced dorsiflexion (gymnastics and dance) and sesamoiditis is given as a diagnosis it is important to have suspicion for stress fractures of the tibial or fibular sesamoid. These injuries comprise around 1–3% of all stress fractures with the tibial sesamoids most commonly affected (75%) (8, 9). Stress fractures are the result of repetitive microtrauma on the bone that overload the capacity of the tissue to cope with this stress. There are a large number of potential contributing factors to any bone stress injury (discussed previously here). Specific to the foot and sesamoids there may be foot, 1st MTPJ and lower limb mechanics that result in increased levels of stress over this site. These are not conclusively studied but could include limited 1st MTPJ range, limited ankle dorsiflexion range, weakness of FHB, FHL and or plantar flexors. Due to the loading pattern there may be a callous present over the site of the 1st MTPJ (1). Suspicion of stress reaction will need imaging with MRI or CT. Management of these bone stress injuries are 4-6 weeks in a non weight bearing cast – avoiding toe dorsiflexion followed by 2 weeks weight bearing in a boot then graded loading (10, 11). If unsuccessful acute management with a screw or more commonly excision can be completed by an orthopaedic specialist (10). Return to sport times across the various management options are approximately 14 weeks (12).
Hallux Limitus
Hallux limitus is defined as a restriction in dorsiflexion of the hallux at the first MPTJ secondary to osteoarthritis of the joint. This can be thought of as a stiff or restricted big toe joint and is commonly considered an early restriction towards hallux rigidus described below. The big toe is designed to bend during gait, with 60 degrees considered normal for gait (7). Restrictions at this joint will often present with gait changes to avoid loading through the big toe due to pain or the limited range of movement. Pain and tenderness are present with attempts to flex and bend the 1st MTPJ (13).
Common causes are trauma (secondary to cartilage damage), excessive pronation leading to increased joint stress and promoting bony exostoses, repetitive 1st MTP joint stress, autoimmune or metabolic conditions (rheumatoid and psoriatic arthritis), hypomobile first ray or muscle weakness (13). Common management is a combination of relative rest from aggravating activities, footwear modification and padding and or orthotics, correct footwear prescription (wider toe box, rocker, reducing height of heels/wedges), big toe and intrinsic foot strength.
Hallux Valgus (“Bunions”)
Hallux valgus (HV), also known as a bunion, is one of the most common forefoot deformities. HV manifests with the proximal phalanx deviating laterally and the first metatarsal head deviating medially and due to the adduction of the first metatarsal (7, 14). HV deformity is most likely a result of multiple contributing factors, including genetics, short first metatarsal, dorsiflexed first metatarsal, flexible or rigid forefoot varus, rigid or flexible pes planovalgus, gastrocnemius equinus, abnormal foot mechanics, and joint hypermobility (7, 14).
Furthermore, HV deformity is more commonly seen in connective tissue disorders such as Marfan syndrome and Ehlers-Danlos syndrome, gouty arthritis, psoriatic arthritis, and rheumatoid arthritis. HV deformity is common in people who wear tight shoes and heels, which is regularly cited as the cause. However, men who wear sensible footwear often have marked HV deformity, while women who wear footwear that significantly compresses their feet have no deformity. This fact has given rise to the thought that footwear exacerbates an underlying bony abnormality rather than acting as the primary cause (14).
Assessment of the big toe in these cases will involve visual assessment of the toe and assessment of range of motion which is quite restricted and often accompanied by grinding or crepitus (1). Commonly, the MTP joint is swollen and tender on the dorsal aspect. If the dorsomedial cutaneous nerve is compressed, a positive Tinels sign may also be elicited by tapping at the site of the nerve. These cases will often be accompanied by complaints of numbness or paresthesias on the medial aspect of the hallux. Patients can present with abnormal gait patterns due to their effort taken to walk on the lateral border of their foot to avoid engaging the great toe and causing pain (1).
There are multiple grading scales used to assess severity. X-ray imaging helps evaluate the structural status of the foot for this. The AP projection helps assess the intermetatarsal angle, hallux abductus angle, metatarsus adductus angle, hallux rotation, and the condition of the first MTP joint. The lateral projection primarily serves to assess the first metatarsal position (elevated or plantar-flexed) and dorsal exostosis/osteophytes (14). This assists in assessment of severity and surgical decision making/
Degree: Hallux valgus angle (HVA) / Intermetatarsal angle (IMA)
- Normal: less than15 degrees / 9 degrees
- Mild: 15 to 30 degrees / 9 to 13 degrees
- Moderate: 30 to 40 degrees / 13 to 20 degrees
- Severe: over 40 degrees / over 20 degrees
Typical non surgical management aims to reduce symptoms, without correcting the change in angle. Most common measures include use of wide toe box shoes with low heels, orthotics, simple analgesic medications, medial bunion padding and mobility exercises for the toe and ankle (14). Additional options that may also be used to reduce pain and pressure include hallux valgus splints, bunion shields, toe spacers or spreaders, and night splints (1). Some individuals’ symptoms and function can prompt referral to an orthopaedic foot and ankle surgeon for opinion. This may result in continued non-surgical pathway or one of the various surgical options; cheilectomy, osteotomy, excision arthroplasty, arthrodesis or joint replacement. Cheilectomy involves the removal of bone spurs at the top of the joint and typically resection of part of the metatarsal head and is typically reserved for early stages (17). A Moberg Osteotomy (dorsiflexion phalangeal osteotomy) is performed in some cases alongside a cheilectomy which involves taking a small wedge out of the first bone of the big toe, the proximal phalanx, and inserting a small screw to change bony alignment and thereby affect pain and function. Excision arthroplasty also known as the Keller procedure where the base of the proximal phalanx is removed and replaced with soft tissue to decompress the joint and create a new pseudo-joint (18). This is not as commonly used due to higher incidence of great toe weakness, deformity and metatarsalgia (15, 16).
Arthrodesis or fusion is one of the most commonly used procedures for end stage hallux rigidus and has higher reported success than other procedures over long term follow up (17, 19). Post surgical care typically involves a period of non weight bearing of 6 weeks followed by protected weight bearing in a post surgical shoe. Other aspects at this treatment stage include protected lower limb strength, upper limb and trunk exercises, non-impact cardiovascular exercises and ankle range of motion exercises. Progression towards normal gait and footwear can commence from the 12 week mark alongside strength exercise and other cardiovascular exercise options (riding, walking).
The final surgery is a big toe joint replacement which may replace part of the joint as a hemiarthroplasty (HemiCap) or an additional component to replace both aspects of the joint. Typical post-operative care will commence early with use of a post surgical shoe, range of motion exercises followed by transition to a stiffer supportive shoe and gait retraining at 4 weeks. Progressing this range of motion, continued gait retraining and the addition of strength occurs at the 4-6 week mark.

Lewis Craig (APAM)
POGO Physiotherapist
Masters of Physiotherapy
Featured in the Top 50 Physical Therapy Blog
References
- Nicholas A. Andrews, Jessyca Ray, Aseel Dib, Whitt M. Harrelson, Ankit Khurana, Maninder Shah Singh & Ashish Shah (2021) Diagnosis and conservative management of great toe pathologies: a review, Postgraduate Medicine, 133:4, 409-420, DOI: 10.1080/00325481.2021.1895587
- York PJ, Wydra FB, Hunt KJ. Injuries to the great toe. Curr Rev Musculoskelet Med. 2017;10(1):104–112.
- Hatch RL, Evaluation HS. Management of Toe Fractures. Am Fam Physician. 2003;68(12):2413–2418.
- Bica D, Sprouse RA, Armen J. Diagnosis and management of com- mon foot fractures. Am Fam Physician. 2016;93(3):183–191.
- Pinter ZW, Farnell CG, Huntley S, et al. Outcomes of chronic turf toe repair in nonathlete population: a retrospective study. Indian J Orthop. 2020;54(1):43–48.
- Chiou D, Stupay KL, Waryasz G. Turf Toe Review. Foot Ankle Spec. 2020;13(2):161–168.
- Brukner and Kahn’s Clinical Sports Medicine 4th Edition
- Ribbans W, Hintermann B. Hallucal sesamoid fractures athletes: diagnosis and treatment. Sports Orthopaed Traumatol. 2016;32:295–303.
- Iwamoto J, Sato Y, Takeda T, et al. Analysis of stress fractures in athletes based on our clinical experience. World J Orthop. 2011;2:7–12
- Castricum A – Stress Fracture Diagnosis and Management 2021
- Fredericson M, Jennings F, Beaulieu C, Matheson GO. Stress fractures in athletes. Top Magn Reson Imaging. 2006;17(5):309–325.)
- Robertson, G. A. J., Goffin, J. S., & Wood, A. M. (2017). Return to sport following stress fractures of the great toe sesamoids: a systematic review. British Medical Bulletin, 122(1), 135-149.
- Grady JF, Axe TM, Zager EJ, Sheldon LA. A retrospective analysis of 772 patients with hallux limitus. J Am Podiatr Med Assoc. 2002 Feb;92(2):102-8. doi: 10.7547/87507315-92-2-102. PMID: 11847262.
- Kuhn J, Alvi F. Hallux Valgus. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553092/
- Perler AD, Nwosu V, Christie D, Higgins K. End-stage osteoarthritis of the great toe/hallux rigidus: a review of the alternatives to arthrodesis: implant versus osteotomies and arthroplasty techniques. Clin Podiatr Med Surg 2013;30:351–395.
- Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg 2012;20:347–358.
- Lau JT, Daniels TR. Outcomes following cheilectomy and interpositional arthroplasty in hallux rigidus. Foot Ankle Int 2001;22:462–470.
- Coughlin MJ, Shurnas PJ. Soft-tissue arthroplasty for hallux rigidus. Foot Ankle International. 2003 Sep;24(9):661-72.
- Stevens, J., de Bot, R. T. A. L., Witlox, A. M., Borghans, R., Smeets, T., Beertema, W., … Schotanus, M. G. M. (2020). Long-term Effects of Cheilectomy, Keller’s Arthroplasty, and Arthrodesis for Symptomatic Hallux Rigidus on Patient-Reported and Radiologic Outcome. Foot & Ankle International, 41(7), 775–783. doi:10.1177/1071100720919681




