

Considering the limited literature targeted at loading management strategies in proximal hamstring tendinopathy, the most accepted model is to progress loads using a pain monitoring strategy (2). That approach to load progression in tendinopathy also makes sense considering pain can potentially inhibit corticospinal activity and alter motor control. Hence, disregarding pain signalling would likely limit motor control restoration and strength gains in the whole kinetic chain (6).
Goom, Malliaras (2), suggest a meaningful task to be monitored daily, at the same time, which will provide information regarding tendon irritability and capacity to withstand loads in 24 hours window by using pain levels as a parameter.
In the context of this case scenario, the initial meaningful task to assess the proximal hamstring response to the proposed exercise program is 3 repetitions of the short lever single leg bridge. The proposed system establishes a cut-off point at 3/10 on a pain scale where any score from 0-3, as assessed by the relevant meaningful task, is reflective of the tendon tolerance to the loading program. In contrast, scores ranging from 4-10 are interpreted as an inability of the pathological tendon to adapt to the loading program given.
In regards to proximal hamstring tendinopathy, adding more hip flexion means greater compressive forces are applied to the proximal insertion of the tendon, increasing tissue demands. Consequently, the exercise program degree of difficulty is not only measured by commonly accepted variables such as load and volume but also by degrees of hip flexion. Therefore, the pain monitoring meaningful task shall progress over time to movements which require greater hip flexion ranges, in order to accommodate for the increased capacity of the tendon to withstand loads throughout the exercise program.
Stage 1 – Isometric Hamstring Load (2, 6, 7)
That is the starting point of the program and the aim is to settle down an irritable tendon with the use of exercises that do not add compression to the proximal hamstring tendon. At the same time, initiating controlled force transmission through the musculotendinous junction and stimulating pain inhibitory mechanism.
The proposed exercises will be executed in 4-5 sets of 45 seconds holds 6 times per week and 3x per day for 4 weeks, starting with body weight only and progressing to elastic resistance. Rest between sets will be short, raging from 45 seconds to 1 minute (Figure 1). Those exercises will be timed according to her training schedule in other to maximise their analgesic potential (Appendix 1). At the end of training or between sessions are the most likely scenario. The isometric contraction will be sustained at 70% maximal voluntary isometric output, which was be determined by a hand held dynamometer during initial assessment.
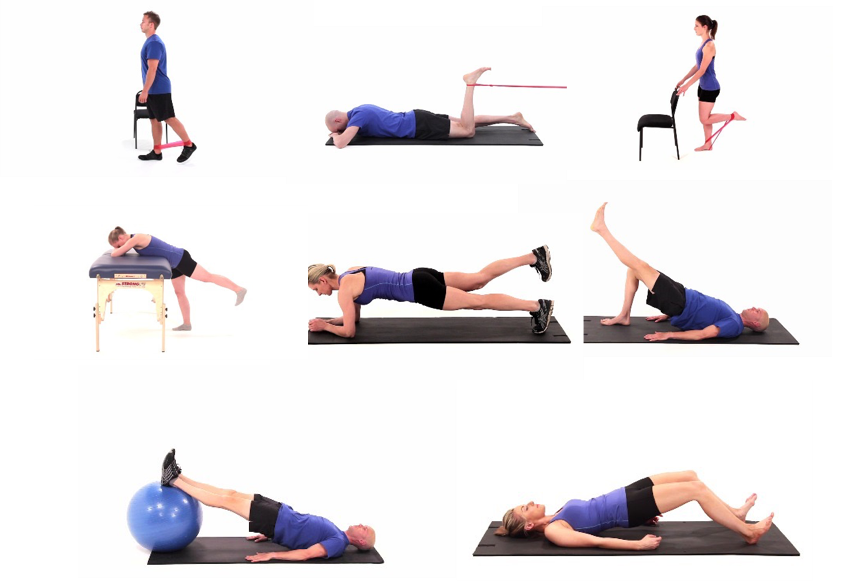
Figure 1 – isometric exercises from stage 1.
Stage 2 – Isotonic Hamstring Load with Minimal Hip Flexion (2, 6)
At this stage, apart from progression of hamstring exercises from isometric to isotonic, light cycling will also be re-introduced on the athlete’s training schedule (Appendix 1). A heavy slow resistance approach will be preferred given that there is some evidence to support its use due to improved collagen turnover in comparison to eccentric contraction in isolation. See Figure 2 for exercises.
The regime will consist of 3-4 bouts of 15 repetition maximum to start (15RM), performed every second day and progressed to 6-8RM accordingly. In order to appropriately restore possible motor control dysfunction, a set pace is recommended where 3 seconds are used for each muscle contraction phase. Calculations around 1RM and its subsets are available from the literature and will be used to determine initial loads which will be progressed taking into consideration meaningful task pain monitoring strategy (8).
The isometric exercises prescribed at stage one will still be used as needed, preferably in alternate days to avoid overloading the tendon. Also, as the main goal in stages 2 and 3 is to build muscle strength and hypertrophy, resting periods between sets are now increased to 2-3 minutes to allow for better muscle recovery (9).
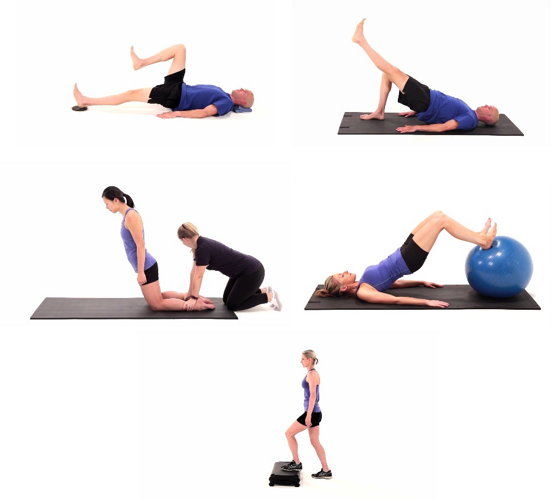
Figure 2 – Stage 2 exercises where further degrees of hip flexion are allowed and loads are progressed based on the meaningful task monitoring and RM calculations.
Stage 3 – Isotonic Exercises in Increased Hip Flexion Angles
Now its 10 weeks from the start of the program and this athlete can tolerate greater flexion ranges at the hip joint. Tendon compression loads are mostly non-provocative and exercises are progressed accordingly. There is not a great variation in sets and repetitions in comparison to stage 2. Also, resting periods in between sets still stand. The main objective now is to incorporate more functional movement patterns relevant to sports performance and also to continue building musculotendinous capacity at increased muscle tension-length ratios.
A greater focus on lumbopelvic control, hip stability and coordinating lower limb kinetic chain with upper torso is desired. Exercises are more dynamic and the complexity of neuromuscular control patterns is higher (Figure 3).
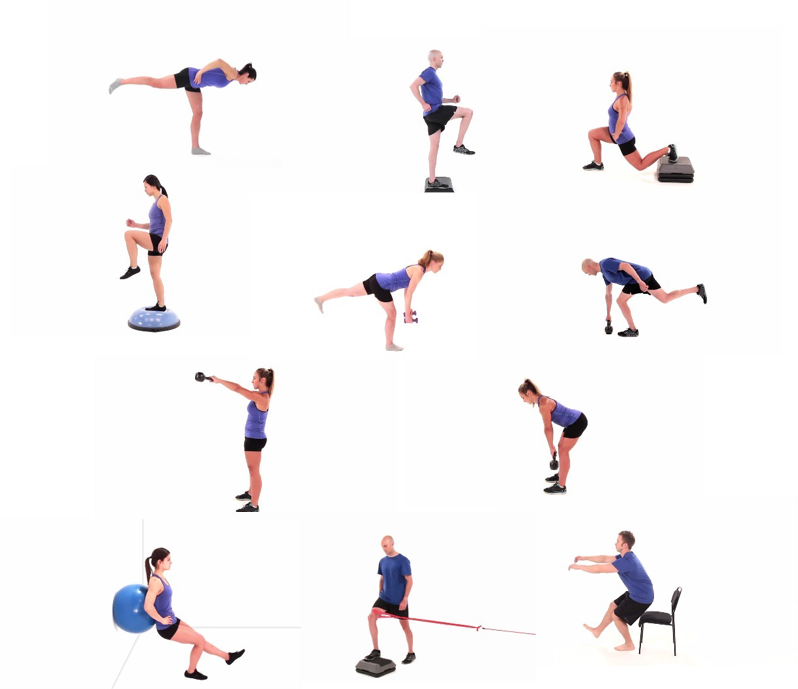
Figure 3 – examples of exercises demanding increased hip flexion angles, suitable for stage 3 proximal hamstring tendinopathy.
Stage 4 – Energy Storage Loading
According to Goom, Malliaras (2), a conservative approach should be taken at that stage. The authors suggest a cycle comprising of stage 4 exercises, followed by stage 2-3 exercises and a third day of stage 1 exercises, being repeated twice per week.
However, given the demands of the training routine for an elite level triathlete, such approach would likely have a great impact on this athletes overall training loads, leading to overtraining, fatigue, tissue breakdown and poor performance. Also, this athlete has reached all the required milestones for a safe transition to stage 4 exercises, which are bilateral strength in single leg tasks and good muscular control in more complex movements. At this point, sets, repetitions and number of exercises performed will be closely tailored to fit in with overall training routine. For instance, loaded split squats jumps and heavy single legged drills would be best avoided after a heavy cycling session with hills; sprinter leg curls, skipping or mountain climbers would be accepted.
Targeted heavy isometric exercises that were regularly used during stages 2 and 3, may still be used as needed in case of early signs of poor tendon adaptation but will not be incorporated in routine schedule in this scenario. Figure 4 provides a few examples.
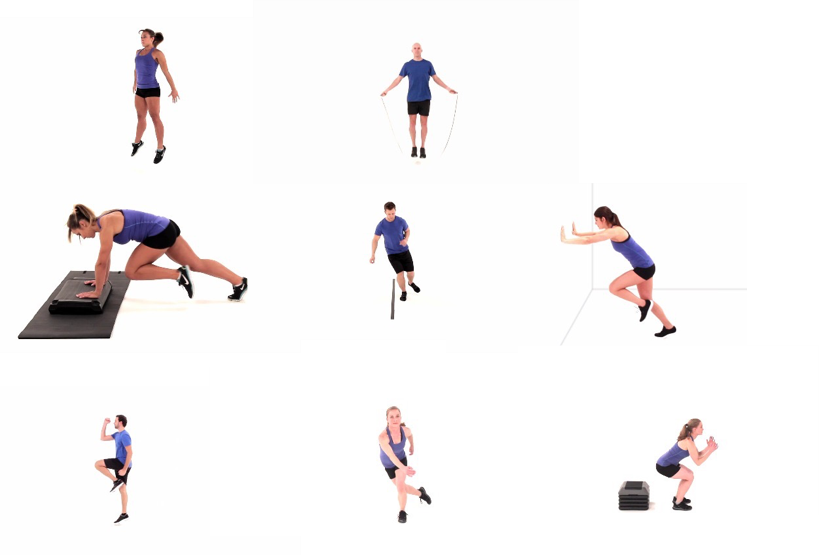
Figure 4 – energy storage exercise variations used in stage 4, also called plyometric exercises which rely on tendons capacity to store and release energy in a short period of time as when running and jumping.
Monitoring injury risk and fatigue
A well accepted concept used to monitor risky of injury is the Acute:Chronic Workload Ratio (10, 11). The acute:chronic workload ratio of this triathlete’s training plan can be found in Appendix 2. For this calculation 2 variables were used, activity duration and perceived rate of exertion (RPE). Subjective self-reported measures are encouraged in sports practice since their sensitivity to change is considered to be superior of other objective measures (12). A guide to interpret acute:chronic workload ratio is provided below (Table 3).

Table 3- extracted from Gabbett 2016.
As per available literature, fatigue levels in triathletes have been successfully measure using the Daily Analyses of Life Demands for Athletes (DALDA), 3km Time Trial Run and (3 KmTT) and Five-bound jump for distance (5BT). Particularly the use of 5BT has been advocated as a valid and reliable measure in the context of the triathlete in order to measure for lower limb muscular fatigue, that holds strong relevance to the context of the athlete (13). The battery of tests will be administered at 10, 16 and 22 weeks as per Appendix 1.
Bruno Rebello (APAM)
Physiotherapist
References
- Cacchio A, Borra F, Severini G, Foglia A, Musarra F, Taddio N, et al. Reliability and validity of three pain provocation tests used for the diagnosis of chronic proximal hamstring tendinopathy. British journal of sports medicine. 2012;46(12):883-7.
- Goom TS, Malliaras P, Reiman MP, Purdam CR. Proximal Hamstring Tendinopathy: Clinical Aspects of Assessment and Management. The Journal of orthopaedic and sports physical therapy. 2016;46(6):483-93.
- Magnusson SP, Langberg H, Kjaer M. The pathogenesis of tendinopathy: balancing the response to loading. Nature reviews Rheumatology. 2010;6(5):262-8.
- Westh E, Kongsgaard M, Bojsen-Moller J, Aagaard P, Hansen M, Kjaer M, et al. Effect of habitual exercise on the structural and mechanical properties of human tendon, in vivo, in men and women. Scandinavian journal of medicine & science in sports. 2008;18(1):23-30.
- Cook JL, Docking SI. “Rehabilitation will increase the ‘capacity’ of your …insert musculoskeletal tissue here….” Defining ’tissue capacity’: a core concept for clinicians. British journal of sports medicine. 2015;49(23):1484-5.
- Rio E, Kidgell D, Moseley GL, Gaida J, Docking S, Purdam C, et al. Tendon neuroplastic training: changing the way we think about tendon rehabilitation: a narrative review. British journal of sports medicine. 2016;50(4):209-15.
- Cook JL, Purdam CR. The challenge of managing tendinopathy in competing athletes. British journal of sports medicine. 2014;48(7):506-9.
- Reynolds JM, Gordon TJ, Robergs RA. Prediction of one repetition maximum strength from multiple repetition maximum testing and anthropometry. Journal of strength and conditioning research / National Strength & Conditioning Association. 2006;20(3):584-92.
- American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Medicine and science in sports and exercise. 2009;41(3):687-708.
- Blanch P, Gabbett TJ. Has the athlete trained enough to return to play safely? The acute:chronic workload ratio permits clinicians to quantify a player’s risk of subsequent injury. British journal of sports medicine. 2016;50(8):471-5.
- Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? British journal of sports medicine. 2016;50(5):273-80.
- Saw AE, Main LC, Gastin PB. Monitoring the athlete training response: subjective self-reported measures trump commonly used objective measures: a systematic review. British journal of sports medicine. 2016;50(5):281-91.
- Coutts AJ, Slattery KM, Wallace LK. Practical tests for monitoring performance, fatigue and recovery in triathletes. Journal of science and medicine in sport. 2007;10(6):372-81.



2 responses to “Proximal Hamstring Tendinopathy Exercise Protocol”
Hi Bruno,
Just read your article cause I have PHT. Best rehab article I’ve read yet on this topic. I would do just about anything at this point to get this pain in my butt to go away. I started exercising about 2 weeks ago and the tenderness deep in my glutes have increased but no sharp pain. But I have a question, by following this program at what point should I expect the tenderness in the lower glute to start to subside? In other words, how do I know I’m not hurting my self with these exercises? How do I know if the tenderness from exercising falls in the 0-3 range for pain measurement using the 3/10 rule? Currently, when I wake up in the morning I relatively pain-free, so I take this a good sign. But after the exercises, I start having mild pain which lasts for the rest of the day. Any tips or advice would be great.
Damon
Hi Damon,
Thank you for your query.
The time course for your pain/symptoms to reduce is really variable and therefore difficult to answer.
I normally however look for a decent reduction in symptoms inside several weeks.
Your guide for whether you are hurting yourself is of the pain of performing the exercise exceeds 3/10.
A simple test for proximal hamstring tendinopathy being to put a leg out straight on a couch while laying on the ground and lifting the other leg and hips to the ceiling-what is the pain level out of 10?
I also suggest listening to this podcast with tendon researcher Dr Peter Malliaras HERE>>
If you get stuck we offer SKYPE consultations which can be very effective for tendon rehabilitation.
Regards Brad Beer