


Bone stress injuries (BSI) are common amongst runners. 0.7-20% of all sports medicine injuries that present to clinicians are bone stress injuries (Bennell, et al 1999).
When it comes to running various papers agree that the annual incidence of BSI is in the vicinity of 20%. Tenforde et al (2015) reported an annual incidence of BSI amongst collegiate track and field and cross country runners to be 20% for both male and female athletes. Meanwhile Benell, et al (1997) reported a 4.9-21% annual incidence in elite track and field athletes.
Pathophysiology of BSI
When bone is subjected to mechanical forces the forces cause adaptive changes in the internal architecture of bone (trabecular), followed by secondary adaptive changes in the external architecture of bone (bone cortex).
In trabecular bone the initial response to mechanical forces is micro damage of the trabecular which is repaired by a microcallus.
In cortical bone (bone’s ‘casing’) the initial response to an increase in mechanical forces is osteoclastic activity (bone break down) which leads to resorption of bone. Osteoblastic cellular activity fills the resorption cavities with what is known as lamellar bone.
However bone formation is slower than bone resorption.
Pathology continuum
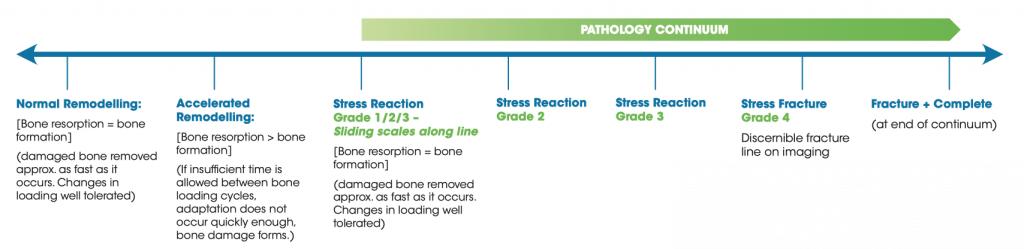
Bone stress injury exists along a pathology continuum.
On the far left of the continuum bone is accruing micro damage following mechanical forces from loading, for example from running. Microdamage accrues proportionate to the number of loading cycles, rate of loading, and strain magnitude of the bone. When the bone is given sufficient time between loading cycles to recover bone the rate of bone resorption is met by the rate of bone repair and remodelling.
However when insufficient time is given for the bone to adapt to external mechanical forces, an imbalance can occur between bone remodelling and microdamage to the bone., resulting in bone structural deformation and fatigue This accumulative micro damage may continue to advance and result in further pathology. The accumulation of microdamage may progress from the bone being in a state of stress reaction through to stress fracture, and at times even frank cortical fracture.
The below timeline summarises the pathology continuum:
Risk factors for BSI
Many runners and clinicians alike attribute the onset of a running related bone stress injury to be due to training loads exceeding the body’s capability. This is in essence accurate AS all running related injuries can conceptually be explained this way. However when it comes to BSI to only consider the external training loads the runner was subjected to ignores the consideration that needs to be given to other known BSI risk factors including the ‘bone health’ of the injured athlete.
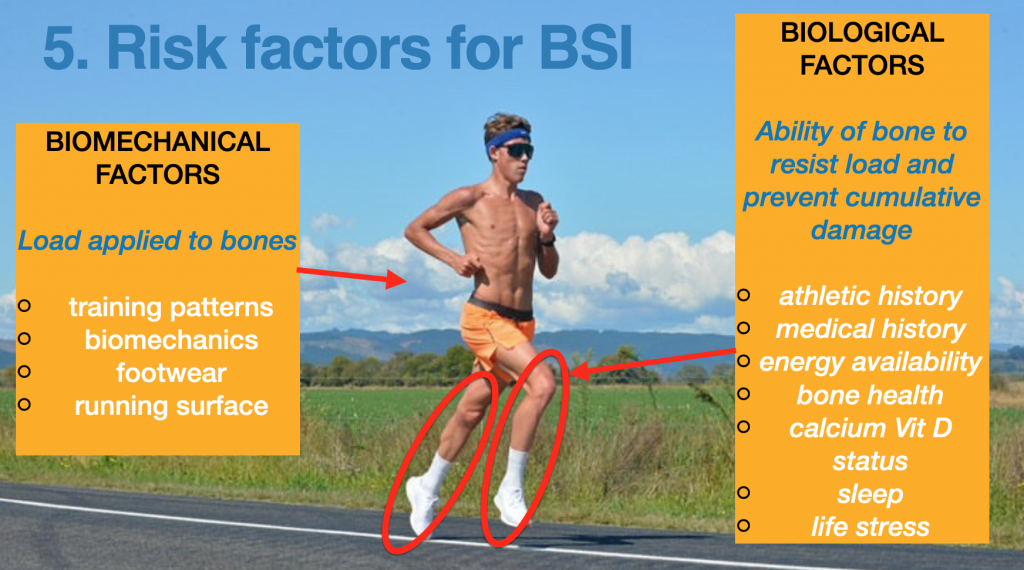
Warden et al proposed that bone stress injury risk factors could be grouped into two categories.
(1) factors that modify and affect the load applied to a bone/skeleton (biomechanical factors)
(2) factors that modify how bone resists strain and the resultant accumulation of damage (biological factors)
The below image depicts the two categories of risk factors:
Let’s explore the biomechanical and biological risk factors.
(1) Factors that modify and affect the load applied to a bone
BIOMECHANICAL FACTORS
While overall in the literature the relationship between the onset of running related injuries and biomechanics is poor (Harrast M.A, 2019). Runner’s gait and their biomechanics can alter bone strain magnitudes, and loading rates and therefore can influence the risk of a BSI. While as a practitioner I do not give static alignment too much consideration with respect to the onset of bone stress injuries in athletes. I am aware that a focus on static alignment can trigger anxieties in athletes, largely because they cannot control their alignment and ‘frame’. Research has validated the following as influencing bone stress injury risk through altering the magnitude and/or direction of bone loading:
- pes cavus and planus feet
- leg length discrepancies
- smaller calf girth
- greater external rotation at the hip (Harrast, M, 2019)
Dynamic biomechanical loading patterns correlated with BSI risk include:
- Greater average vertical loading
- Higher peak acceleration
- Grater peak free mass
- Higher pak adduction, knee internal rotation, tibial internal rotation, rear foot eversion during gait (Tenforde, et al, 2016)
Training patterns and loads
Hreljac et al (2005) reported that approximately 60% of all running related injuries are due to training errors.
Increased training volume, intensity, and/or frequency of training loads increases the number of bone loading cycles.
When a runner progresses their training the result can be a shift in load magnitude, rate, and acceleration of bone fatigue. Increases in running speed increase ground reaction forces, muscle contraction forces and therefore internal bone loads (Zelik et al, 2019).
As training loads are elevated the recovery time required for the accumulated bone microdamage also increases. However when the frequency of loading cycles, ie number of times a runner runs in a week is increased, or running sessions become longer, compromising of bone recovery can occur. This can result in insufficient repair time for the bone and result in accelerated bone remodelling and elevated bones stress injury risk.
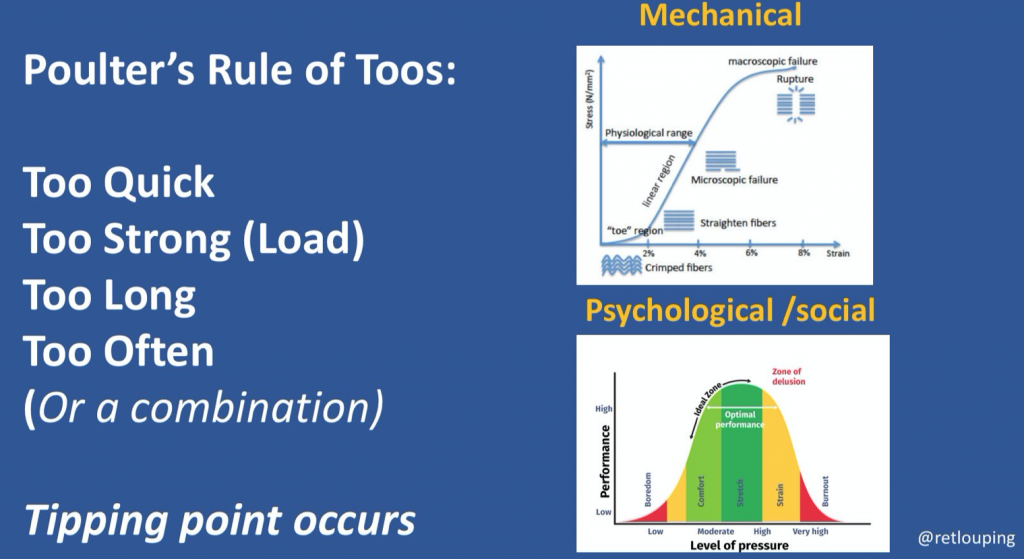
A nice way to summarise training errors is to think of David Poulter’s ‘Rule of Toos’. Simply put with regards to training: too quick, too strong, too long, too often, or a combination can result in a training error occurring (see below).
The ‘error’ occurs as the increase in training loads exceeds the tissue’s mechanical tolerance point, and injury occurs.
It’s also worth considering that psychological stress can represent a ‘load’ of sorts which can contribute to an athlete’s ability to recover from training cycles and absorb the training load.
In the literature adolescent runners who ran greater than 32km week had an increased risk of BSI (Tenforde, et al, 2013). While athletes who trained more than 700 hours during a year (>13hrs week) had 2.1-fold risk for an overuse injury compared to the others (Ristolainen et al, 2014).
Muscle factors
Muscle is protective against BSI. During loading muscle acts as an active shock attenuator assisting with the attenuation of loads on the skeleton as they are transmitted proximally. Interestingly muscular contractions on bones have been shown to produce large internal bone loads. Zelik et al (2019) reported compressive tibial forces equivalent to 6-14x body weight, and surmised that it is the increase in compressive loads on bone with faster running speeds that is a greater consideration for BSI risk than what was prior believed to be the increase in ground reaction forces.
Even though Zelik et al findings reported that muscle forces increased bone loading it is well established that when muscles surrounding bones become weakened or fatigued their ability to attenuate impact bone loads is lessened (Mercer et al, 2014) , resulting in increases in skeletal bone loading (Clancy et al, 2012, Mizrahi et al , 2000) and heightened BSI risk (Fyhrie et al, 1998, Milgrom et al, 2007).
Furthermore muscle fatigue may result in altered running kinematics which may affect the direction of bone loading and therefore bone strain at less accustomed bone sites (Yoshikawa et el, 1994).
Muscle size (Beck et al, 2000 ) and strength (Hoffman, et al, 1999) have also been correlated with a protective role of muscle in stress fracture development.
Running surfaces
Running surfaces may represent a possible BSI risk factor. The influence of running surfaces and terrain is however controversial, as a runner inherently adjusts their overall leg stiffness when running on different surfaces compliances in effect manipulating and controlling the loading rates on the bone. This manipulation of leg stiffness allows the runner to maintain a constant vertical excursion of their centre of mass (Dixon et al, 2000)
For example when running on concrete (a stiff surface) ground reaction loading forces are increased, however a runner will decrease their leg stiffness to accommodate to the increase in ground reaction force, and invariably internal bone loads.
It can be helpful to note if a runner has had any sudden change in running surface as a potential bone stress injury risk factor.
Changes may include:
- increased running time on stiff (less compliant) surfaces such as the pavement, which may increase bone strain magnitudes and the rate of strain (Milgrom et al, 2003)
- Increased time running on very compliant (not stiff) surfaces such as sand or grass, which may increase the energy cost of running, and therefore possibly affect muscle fatigue levels and kinematics which may negatively influence bone loading rates.
- Running downhill which may result in less shock attenuation, and increase bone loading rates and magnitude (Mizrahi et al, 2000), (Gottschall et al, 2015)
- A shift in running routes and therefore terrain which may alter running kinematics and increase bone loads on less accustomed bone sites
Running footwear
This is an enormous area of debate and speculation. When self assessing for bone stress injury causation many runners will attribute footwear as a likely contributing factor for injury onset. Saragiotto, et al 2014 reported that ‘wearing the wrong shoes’ was cited as a reason for running injury onset.
Running shoes and inserts theoretically attenuate ground impact forces, and potentially influence the motion of the foot and kinetic chain.
Via these two mechanisms shoes and orthoses may influence bone loading and therefore serve as possible risk factors for running related bone stress injury.
For more on the role of running shoes and orthoses refer to the below Expert Editions of The Physical Performance Show:
- Foot Orthoses: fact and fiction-Ian Griffiths HERE>>
- Running Shoe Masterclass: Bartold Clinical HERE>>
(2) Factors that modify the ability of the bone to resist strain and the accumulation of damage
BIOLOGICAL FACTORS
- Athletic/physical activity history
An athlete who has a history of bone stress injury is at elevated risk for a subsequent bone stress injury (Wright et al, 2015). Furthermore both male and female runners with a prior stress fracture were shown to have heightened risk for further bone stress injury (Kelsey, et al 2007). It has been documented that 10.3-12.6% of runners who have a history of BSI sustained a second BSI within 2yrs (Bennell et al 1996, Kelsey et al 2007).
Consideration also needs to be given to an athlete’s recovery status. Ristolainen et al (2013) reported that athletes with less than 2 rest days per week during the training season had 5.2-fold risk for an overuse injury.
Likewise male endurance runners with greater than five years of training history were shown to have a 30% reduction in testosterone levels compared to athletes with fewer years of training (Hackney et al, 2018). This reduction in sex hormone levels may have an adverse effect on bone helath and therefore enhance risk of bone stress injury for the athlete.
Adolescents with a history of participation in high impact multidirectional bone loading sports such as basketball or soccer may improve bone density and bone geometry compared with children who participate in repetitive low impact sports such as distance running (Tenforde et al, 2015).
- Medical history
A family history of bone stress injury or osteoporosis/osteopenia may represent elevated bone stress injury risk for an athlete. It has been estimated that 60-80% of peak bone mass is determined by genetics.
Pubertal and menstrual history for female athletes is key. This can include the age of menarche, with delayed onset of menarche > 15years being a notable risk factor for bone health. The missing of menstruation cycles may indicate low energy availability status for a female runner which may impact on bone health.
Prior history of medication that can influence bone health is important and can include use of oral steroids, hormone therapies, cancer treatment medications, or methotrexate use for rheumatic conditions such as psoriatic arthritis, lupus or juvenile arthritis.
An athlete with celiacs disease, hyperparathyroidism, or hyperthyroidism, or hypogonadism may also be at heightened risk of bone stress injury development.
- Energy availability/ RED-S
Runners require adequate fuelling and energy availability for both the training workload and also their daily life function and physiological processes.
Athletes can underestimate the energy cost of basic daily physiological processes. This oversight can create an environment of low energy availability. Elevated training loads that are not matched with an increase in energy intake can also create a situation of low energy availability. The goal is to achieve a state of energy balance whereby energy intake is adequate to fuel the physiological and training related demands of the athlete’s body.
Low energy availability can be the result of reduced caloric intake through either intentional or unintentional means. Intentional means can include Disordered Eating (DE) or Eating Disorders (ED), while unintentional means can be as outlined above where fuelling is insufficient for the athlete’s workload and daily processes, or training loads are excessive.
The below image from Nicky Keay outlines how athletes need to match the energy required to support life processes as well as their training load by the appropriate energy intake. It also illustrates how energy requirements may not met in situations of excessive training, and insufficient energy intake.
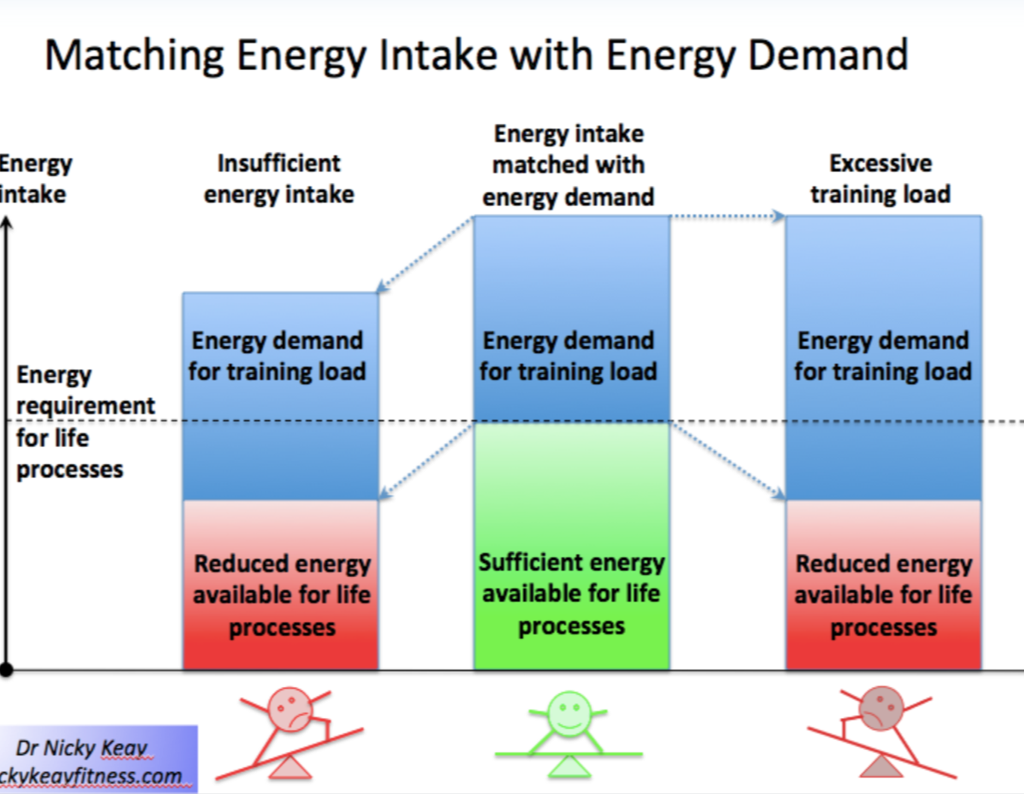
As energy availability decreases physiological changes occur in order to conserve energy. Specific for female athletes studies have reported that proper reproductive (hypothalamic-pituitary-ovarian axis) physiological functioning is achieved with an energy availability of 30kcal/kg of fat free mass per day, while 45kcal/kg of fat free mass is required daily in order to maintain bone metabolism.
In the early 90’s the interrelationship between energy availability, menstrual function, and bone mineral density was described by the phrase ‘Female Athlete Triad’. While female athletes may have one or more of the three components at suboptimal levels, low energy availability appears to be the key factor. Each factor of the Triad spans the gamut ranging from optimal to pathological. At one end a female athlete has adequate energy availability, normal menstruation cycles (eumenorrhea), and optimal bone health. Towards the pathological end of the spectrum a female athlete may have reduced energy availability, menstrual disorders such as oligomenorrhea (infrequent menstrual periods), and sub optimal bone health (e.g. low bone mineral density). The greater the number of Triad risk factors the more heightened the risk of bone stress injury (Tenforde, et al, 2013).
In 2014 the International Olympic Committee (IOC) recognised that the Female Athlete Triad’s limitations were that male athletes are also affected by low energy availability. They introduced the term Relative Energy Deficiency in Sport (RED-S).
RED-S is common in both male and female middle and long distance runners. Koehler et al. (2013) reported RED-S to be more common in female (58%) than male (51%) endurance athletes. In elite athletics the prevalence of clinical low energy availability was 31% and 25% in female and male middle- and long-distance athletes (Heikura et al., 2017)
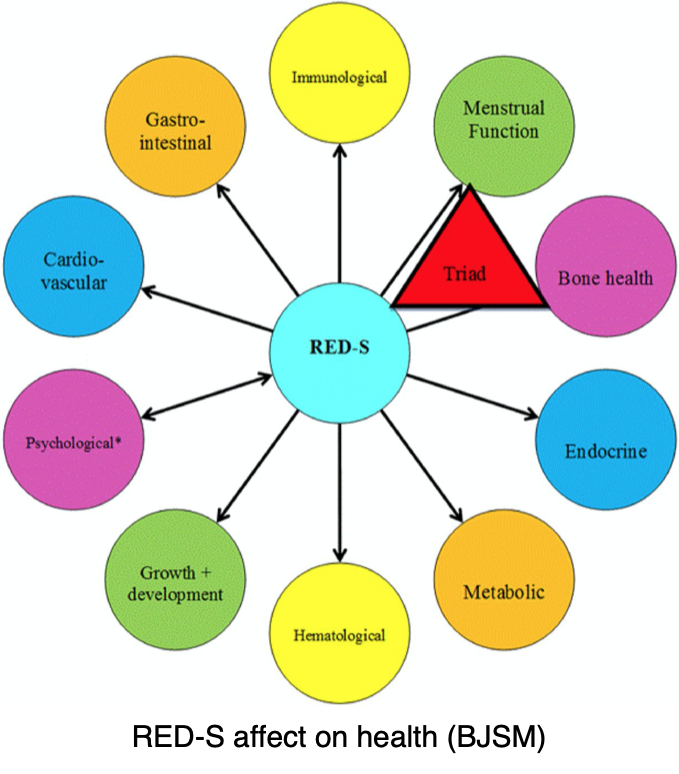
The key driver of RED-S is low energy availability. The effects of RED-S on the athlete can be both performance and health related and are depicted in the below diagrams (Mountjoy et al, 2018):
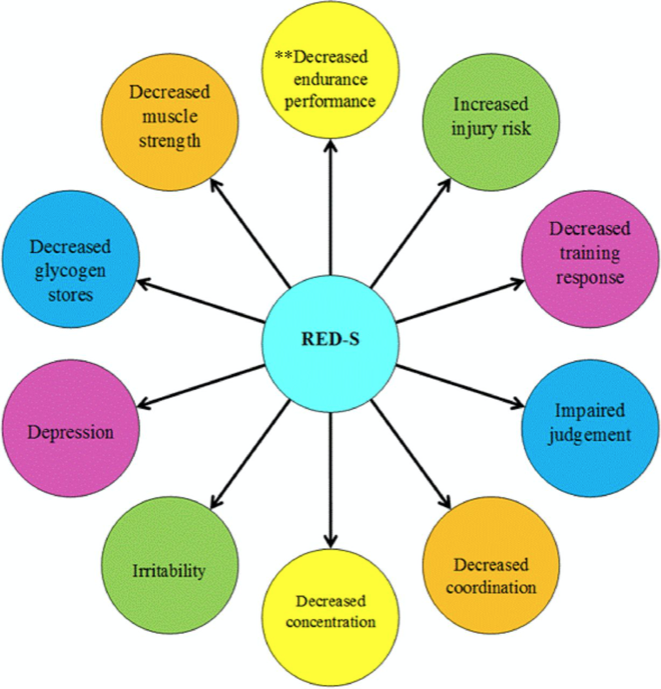
Potential effects of RED-S on performance
There exists a known increased risk of low bone mineral density and reduced bone health for athletes with low energy availability. Low energy availability may be reflected by low body mass index* (BMI), whereby BMI <17.5kg/m2, and or >10% weight loss in a month (Gibbs et al, 2014).
*Body Mass Index: Calculated by weight (kg)/ square of height in metres
It is important to screen runners with a bone stress injury for RED-S, for optimal recovery, and health and performance of the athlete.
For male runners low testosterone levels have been associated with low bone mineral density (Hind et al, 2006). A 30% reduction in testosterone levels has been reported in athletes with at least five years of endurance running compared to athletes with fewer years of training (Hackney et al, 2018).
Tenforde et al (2018) reported that male runners are at 6.1 times heightened risk of low bone mineral density compared with non runners. While male runners with bone stress injury in high risk anatomic sites (femoral neck, anterior tibia, navicular) are at further risk of low bone mineral density compared with runners that incurred a BSI in a low risk region (eg medial tibia, or femoral shaft).
However it is challenging for an athlete to know if they are in a state of energy balance as measuring caloric intake and energy expenditure is difficult in sophisticated laboratories let alone ‘real life’. Screening for RED-S/Female Athlete Triad is difficult as symptoms are subtle.
Screening tools such as the Low Energy Availability in Females Questionnaire (LEAF-Q) can be used to give an indication of whether a female athlete may be in a state of low energy availability. No equivalent exists as of the time of writing for male athletes, however work is underway on the Low Energy Availability in Males Questionnaire (LEAF-M).
The IOC published the RED-S Clinical Assessment Tool (RED-S CAT) as a screening tool and as a guide for clinicians in making return to sport decisions for athletes.
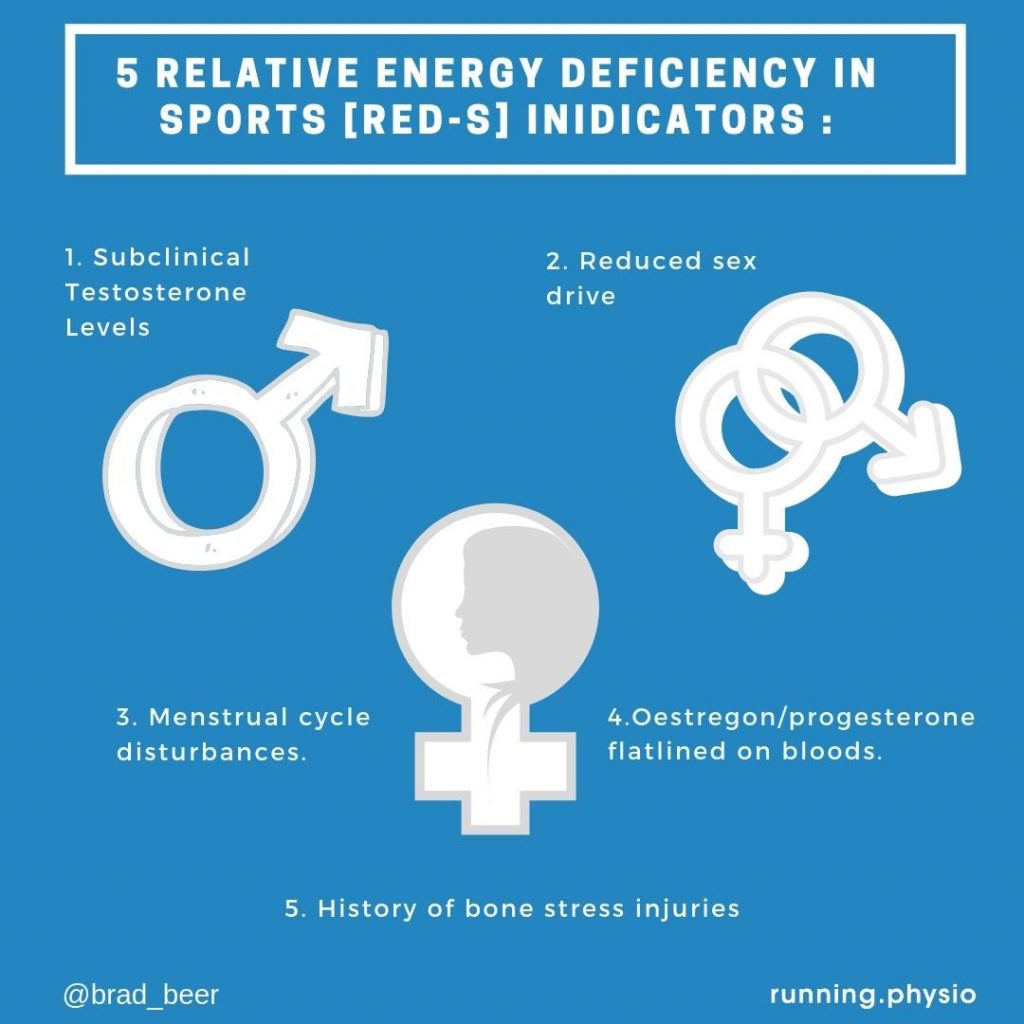
The best indicators of whether an athlete is not in a state of energy balance but rather experiencing low energy availability are secondary indicators. These can include:
- Males:
- absence of morning erections
- reduced libido
- Sub clinical testosterone hormone levels on blood testing
- Females:
- Absence of menstrual cycle
- Sub clinical oestrogen hormone levels on blood testing
The below infographic summarises these secondary indicators of low energy availability:
Bone health
One of the key yet sometimes overlooked bone stress injury risk factors is the health of the athlete’s bone. The bone health of an athlete plays a key role in resisting the strain and resultant accumulation of damage that occurs with endurance running.
Lower bone mineral density is correlated with heightened risk of bone stress injury.
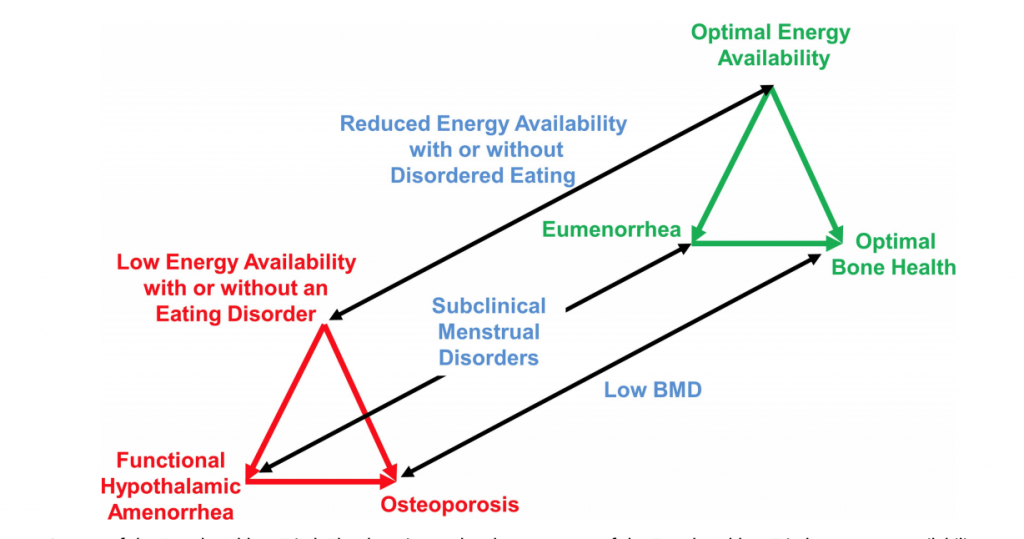
The below figure (Spectra of the Female Athlete Triad) as published by De Souza et al (2014) depicts the 3 components of the Female Athlete Triad: menstruation status, energy availability, and bone health. Optimal health exists at one end of the spectrum: eumenorrhea, energy availability, and optimal bone health. At the other end of the spectrum: amenorrhea, energy deficiency, and pathological bone health i.e. osteoporosis.
Bone health of athletes can be determined by dual energy x-ray absorptiometry (DXA) scanning which determines an athlete’s bone mineral density (BMD). Weight bearing sites of the lumbar spine, total hip, and femoral neck are assessed in the adult athlete. While children, adolescents, and young women (<20yrs) bone mineral content (BMC) may be assessed for in order to account for maturation delays. Repeat DXA scans can be performed every 1-2years to ascertain for bone status, and the effectiveness of any interventions being used to attempt to improve bone health.
DXA scans will give results for the sites assessed for and be reported in terms of Z-scores and T-scores.
Interpreting DXA scores are as follows according to The American College of Sports & Medicine:
Low BMD Z-score* for premenopausal female athletes Z score -1.0 to -2.0, and osteoporosis < -2.0 SD.
The International Society for Clinical Densitometry (ISCD) a Z-score of < -2.0 SD is interpreted as being ‘below age expected range’, while osteoporosis is diagnosed when in addition to a Z-score of <-2.0 SD there are risk factors for fracture. Likewise for children and adolescents osteoporosis is only diagnosed when there has been a clinically significant fracture history.
Clinically if there has been a history of bone stress injury for an athlete an index of suspicion should exist regarding the status of the athlete’s bone health.
While there exists no definitive method in determining when an athlete should have a BMD study performed, the 2014 Female Athlete Triad Coalition Consensus Statement of Treatment and Return to Play (De Souza MJ, et al 2014) provide guidelines for when BMD testing for athletes may be warranted.
When there are 1 or more ‘high risk’ Female Athlete Triad factors which include: two prior BSI’s, one high risk BSI, prior Z-score -2.0, history of 50% of menstruation cycles over 12 months, menarche > 16yrs of age, a diagnosed eating disorder, or > 10% body weight loss in 1 month, DXA testing should be performed.
When there are > 2 ‘moderate risk’ Female Athlete Triad factors which include: one prior BSI, Z-score of between -1.0 and -2.0, weight loss of 5-10% in one month, history of disordered eating of > 6 months duration, and a current history of 6-8 menstruation cycles over a 12 month window.
The Consensus Statement also recommends athletes taking medications for 6 months or more that may impact bone health.
Calcium and Vit D status
Calcium gives strength to the bone matrix. Meanwhile the role of Vitamin D is to facilitate absorption of calcium to ensure bone growth and remodelling.
There exists a high prevalence of Vitamin D deficiency in runners, with low Vitamin D levels having been associated with increased incidence of BSI (Ruohola, et al, 2006).
Female runners who consumed less than 800mg calcium per day, were found to have a 600% greater stress fracture rate than female runners who consumed greater than 1500mg of calcium per day (Nattiv et al, 2013).
Dietary calcium intake recommendations are:
Adults need to have an intake of 1,000 mg calcium (recommended daily intake, RDI). This should increase to 1,300mg for women over 50yrs of age, and men over 70yrs. Athletes daily intake would ideally be greater given the large amount of calcium that is lost in sweat.
It has been suggested that amenorrheic female runners and males with BSI risk factors may require an additional 500mg of daily calcium intake to assist with required calcium homeostasis (Harrast, M, 2019).
Related: Calcium levels for runners: a dairy -free example of meeting the calcium RDI
Meanwhile bone health experts recommend between 1000 and 2000 IU/day for maintenance of optimal Vitamin D levels.
Upcoming blog
In the next blog in this bone stress injury series I will outline the best evidence based clinical rehabilitation pathways in returning runners with bone stress injury back to running.
Related
The Physical Performance Show: Nicky Kaey-RED-S, hormone health and performance HERE>>
The Physical Performance Show: Clare Minahan-Considerations of the Female Athlete HERE>>
Preventing Bone Stress Injuries in Triathletes: Triathlon Victoria presentation HERE>>

Brad Beer (APAM)
APA Titled Sports & Exercise Physiotherapist (APAM)
B.Physio/ B. Ex. Sc
Founder POGO Physio
Author ‘You CAN Run Pain Free!’
Host The Physical Performance Show
Featured in the Top 50 Physical Therapy Blo
References
- Ground reaction force metrics are not strongly correlated with tibial bone load when running across speeds and slopes: Implications for science, sport and wearable tech. Emily S. Matijevich , Lauren M. Branscombe, Leon R. Scott, Karl E. Zelik. Published: 2019 Jan 17;14(1):e0210000. doi: 10.1371/journal.pone.0210000. eCollection 2019.
- Mercer JA, Bates BT, Dufek JS et al. Characteristics of shock attenuation during fatigued running. J Sports Sci 2003;21(11):911–9. 26. Mizrahi J, Verbitsky O, Isakov E.
- Fatigue-induced changes in decline running. Clin Biomech (Bristol, Avon) 2001;16(3):207–12. 27.
- Clansey AC, Hanlon M, Wallace ES et al. Effects of fatigue on running mechanics associated with tibial stress fracture risk. Med Sci Sports Exerc 2012;44(10):1917–23. 28.
- Mizrahi J, Verbitsky O, Isakov E. Fatigue-related loading imbalance on the shank in running: a possible factor in stress fractures. Ann Biomed Eng 2000;28(4):463–9. 29.
- Fyhrie DP, Milgrom C, Hoshaw SJ et al. Effect of fatiguing exercise on longitudinal bone strain as related to stress fracture in humans. Ann Biomed Eng 1998;26:660–5. 30.
- Milgrom C, Radeva-Petrova DR, Finestone A et al. The effect of muscle fatigue on in vivo tibial strains. J Biomech 2007;40(4):845–50.
- Yoshikawa T, Mori S, Santiesteban AJ et al. The effects of muscle fatigue on bone strain. J Exp Biol 1994;188:217–33.
- Beck TJ, Ruff CB, Shaffer RA et al. Stress fracture in military recruits: gender differences in muscle and bone susceptibility factors. Bone 2000;27(3):437–44
- Hoffman JR, Chapnik L, Shamis A et al. The effect of leg strength on the incidence of lower extremity overuse injuries during military training. Mil Med 1999;164(2):153–6.
- Dixon SJ, Collop AC, Batt ME. Surface effects on ground reaction forces and lower extremity kinematics in running. Med Sci Sports Exerc 2000;32(11):1919–26.
- Milgrom C, Finestone A, Segev S et al. Are overground or treadmill runners more likely to sustain tibial stress fracture? Br J Sports Med 2003;37(2):160–3.
- Mizrahi J, Verbitsky O, Isakov E. Shock accelerations and attenuation in downhill and level running. Clin Biomech (Bristol, Avon) 2000;15(1):15–20.
- Gottschall JS, Kram R. Ground reaction forces during downhill and uphill running. J Biomech 2005;38(3):445–52.
- De Souza MJ, Nattiv A, Joy E, et al2014 Female Athlete Triad Coalition Consensus Statement on Treatment and Return to Play of the Female Athlete Triad: 1st International Conference held in San Francisco, California, May 2012 and 2nd International Conference held in Indianapolis, Indiana, May 2013British Journal of Sports Medicine 2014;48:289.
- Saragiotto BT, Yamato TP, Lopes AD. What do recreational runners think about risk factors for running injuries? A descriptive study of their beliefs and opinions. J Orthop Sports Phys Ther. 2014;44(10):733‐738. doi:10.2519/jospt.2014.5710
- Ristolainen et al (2014) Training related risk factors in the aetiology of overuse injuries in endurance sports. J Sports Med Phys Fitness. 54 (1), 78-97.
- Kelsey, Jennifer & Bachrach, Laura & Procter-Gray, Elizabeth & Nieves, Jeri & Greendale, Gail & Sowers, Maryfran & Brown, Byron & Matheson, Kim & Crawford, Sybil & Sainani, Kristin. (2007). Risk Factors for Stress Fracture among Young Female Cross-Country Runners. Medicine and science in sports and exercise. 39. 1457-63. 10.1249/mss.0b013e318074e54b.
- Hackney AC, Lane AR. Low testosterone in male endurance-trained distance runners: impact of years in training. Hormones (Athens). 2018;17(1):137‐139. doi:10.1007/s42000-018-0010-z
- Tenforde AS, Sainani KL, Carter Sayres L, Milgrom C, Fredericson M. Participation in ball sports may represent a prehabilitation strategy to prevent future stress fractures and promote bone health in young athletes. PM R. 2015;7(2):222‐225. doi:10.1016/j.pmrj.2014.09.017
- Tenforde AS, Sayres LC, McCurdy ML, Sainani KL, Fredericson M. Identifying sex-specific risk factors for stress fractures in adolescent runners. Med Sci Sports Exerc. 2013;45(10):1843-1851. doi:10.1249/MSS.0b013e3182963d75.
- Mountjoy M, Sundgot-Borgen JK, Burke LM, et alIOC consensus statement on relative energy deficiency in sport (RED-S): 2018 updateBritish Journal of Sports Medicine 2018;52:687-697.
- Gibbs JC, Nattiv A, Barrack MT, et al. Low bone density risk is higher in exercising women with multiple triad risk factors. Med Sci Sports Exerc. 2014;46(1):167-176. doi:10.1249/MSS.0b013e3182a03b8b.
- Koehler K, Achtzehn S, Braun H, Mester J, Schaenzer W. Comparison of self-reported energy availability and metabolic hormones to assess adequacy of dietary energy intake in young elite athletes. Appl Physiol Nutr Metab. 2013;38(7):725-733. doi:10.1139/apnm-2012-0373.
- Harrast, M.A, Clinical Care of the Runner. Assessment, Biomechanical Principles, and Injury Management (2020).
- Heikura, Ida & Uusitalo, Arja & Stellingwerff, Trent & Bergland, Dan & Mero, Antti & Burke, Louise. (2017). Low Energy Availability is Difficult to Assess But Outcomes Have Large Impact on Bone Injury Rates in Elite Distance Athletes. International Journal of Sport Nutrition and Exercise Metabolism. 28. 1-30. 10.1123/ijsnem.2017-0313.
- Hind K, Truscott JG, Evans JA. Low lumbar spine bone mineral density in both male and female endurance runners. Bone. 2006 Oct;39(4):880-885. DOI: 10.1016/j.bone.2006.03.012.
- Hackney AC, Aggon E. Chronic Low Testosterone Levels in Endurance Trained Men: The Exercise- Hypogonadal Male Condition. J Biochem Physiol. 2018;1(1):103.
- Tenforde AS, Parziale AL, Popp KL, Ackerman KE. Low Bone Mineral Density in Male Athletes Is Associated With Bone Stress Injuries at Anatomic Sites With Greater Trabecular Composition. Am J Sports Med. 2018;46(1):30-36. doi:10.1177/0363546517730584
- Ruohola JP, Laaksi I, Ylikomi T, et al. Association between serum 25(OH)D concentrations and bone stress fractures in Finnish young men. J Bone Miner Res. 2006;21(9):1483-1488. doi:10.1359/jbmr.060607




