


Introduction
Patellar dislocations account for 2-3% of knee injuries, and tend to affect younger, active individuals, with the highest incidence in the second and third decades of life. Females in their adolescent years are the group with the high incidence rates (1). Over the long term, if untreated, patellar dislocations can result in patella instability, recurrent dislocations / subluxations, pain and a reduction in sporting activity (2). Acute patellar dislocations usually occur as a result of trauma, such as a non-contact twisting injury of the knee, or direct blow to the patella that knocks it out (1). This blog will focus on the management and rehabilitation of acute first-time / primary dislocations.
Patellofemoral Joint Anatomy
Patellofemoral stability results from complex interactions between active and dynamic stabilisers. Recent studies have investigated the role of the medial patellofemoral ligament (MPFL) and found it to be the most significant passive stabiliser of the patella (2). Neighbouring soft tissues, such as the patellomeniscal and patellotibial ligaments, as well as the medial retinaculum also make contributions to stability.
Predisposing Factors
Primary factors
- Trochlear Dysplasia
- Elevated TT-TG distance
- Patella Alta
- Patellar tilt
Secondary factors
- Elevated Q angle with tibial tubercle lateralisation and genu valgum
- Elevated femoral anteversion with compensatory lateral tibial torsion
- Vastus medialis hypoplasia
- Ligament laxity
- Patellar dysplasia
(5)
Patellar dislocations can also occur in populations with hypermobility or generalised ligament laxity under less traumatic conditions, however these populations generally tend towards recurrent subluxation episodes, rather than frank dislocations (1).
Mechanism of Injury
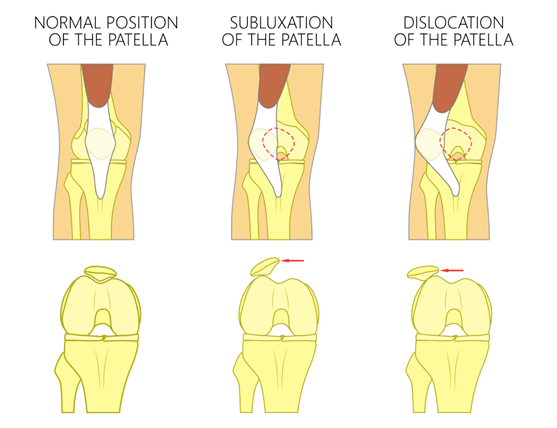
Patellar dislocation occurs when the patella completely disengages from its normal position in the trochlear groove, where subluxations involve only partial movement of the patella.
(6)
Lateral patellar dislocations, whereby the patella dislocations outwards, are by far the most common, with medial dislocations (dislocation inwards) being considered exclusively iatrogenic. Intra-articular dislocations are also possible, however they are rare.
It is estimated that 90% of lateral patellar dislocations occur during a non-contact twisting injury, such as a sudden lateral cut. The most common dislocation pattern starts with the knee nearly straight, at the start of knee flexion, and when a rotational / valgus force is applied the patella dislocates as the knee moves into further flexion. In addition to this, there are two less common dislocation mechanisms, where the patella dislocation occurs with the knee starting in a greater range of flexion. From a squat starting position the dislocation occurs during deceleration, with the dislocation occurring as the knee moves further into flexion, or during acceleration where dislocation occurs as the knee extends. Incidents causing acceleration dislocations are typically lower energy traumas, with some examples as described by patients including taking off to jump, standing from a seated position or lifting from a bent knee position (4).
Patients typically describe pain and deformity of the knee post dislocation incident, often describing a “pop” and a feeling of the knee giving way. Swelling / joint effusion and hemarthrosis (bleeding into the knee joint) are common for primary dislocations, however less common in those with recurrent episodes.
Early Management
Reduction
Patellar dislocations usually reduce spontaneously or with simple manipulation in the emergency department. If required, the reduction process involves flexing the hip, applying gentle medially directed pressure to the lateral patella while slowly moving the knee into extension (1).
Imaging
Plain film X-ray imaging should include a weight-bearing AP view in extension, Merchant view – weight-bearing in 45˚ flexion (also known as femoropatellar axial view) and lateral view in 30˚ flexion. CT imaging assesses osseous predisposing factors (as listed above). MRI can be used to precisely determine the injured structures, which guides treatment.
Dislocation Sequelae
When the patella dislocates, this can result in damage to the surrounding bony surfaces and soft tissues.
In a patellar dislocation an MRI may reveal;
- Haemarthrosis – bleeding into the joint
- Bone oedema and osteochondral lesions of the medial patellar facet and anterolateral aspect of the lateral femoral condyle due to impaction during dislocation
- Concave deformity of the inferomedial patella due to impaction
- Medial capsulo-ligamentous tears
- Osteochondral fractures
Conservative vs Surgical Management
Multiple systematic reviews and meta-analyses have been conducted attempting to determine whether conservative or surgical management is superior. Common to all studies is the report that the current level of evidence is low and further studies are required to determine definitive conclusions. A 2020 systematic review (9) revealed no significant difference between conservative and surgical management over the following domains; subluxation rate, Kujala score (Kujala Anterior Knee Pain outcome measure), patient satisfaction and frequency of reoperation. Tegner activity scores were higher in the conversative group, however recurrent dislocation rates were also higher in the conservative group.
Surgical Management
Indications for surgical management;
- Osteochondral fracture
- Intra-articular knee joint disorder
- Major tear of the medial soft tissue structures (i.e. MPFL)
- Failed conservative management / recurrent dislocations, particularly in those with joint abnormalities
Arthroscopy
In the case of an osteochondral fracture an arthroscopic procedure may be necessary for removal of loose fragments, depending on the size. If there is sufficient bone available for fixation an osteochondral fragment repair is favoured (1).
MPFL Repair or Reconstruction
There is good emerging evidence to support medial patellofemoral ligament reconstruction. When performing MPFL reconstruction evidence suggests that double-bundled repair is superior to single-bundled (7). A 2016 study investigated the outcomes following isolated MPFL reconstruction and reported excellent outcomes, both subjectively and clinically. A high percentage of young participants successfully return to sport, with a low incidence of recurrent instability, post-operative apprehension and re-operations (8).
Lateral Release
A lateral release involves cutting the retinaculum on the lateral knee joint, with the aim to improve patella alignment by reducing lateral pull. Lateral releases have historically been performed in combination with other realignment procedures (1). However, the literature suggests that the addition of a lateral release to other procedures does not improve clinical outcomes, with the outcomes of an isolated MPFL being superior. There is emerging evidence to suggest that lateral releases can also lead to post operative patellar instability, and increase the risk of medial patellar dislocations (8).
Osseous Procedures
An osteotomy is used when there is abnormal anatomy that contributes to poor patella tracking. Most commonly during these procedures the patella’s attachment is moved medially and distally to correct patella tracking, which reduces the Q angle and patella alta, which are predisposing factors for dislocations. Trochleoplasties can be indicated in recurrent dislocations with a flat or convex trochlea, whereby the trochlear groove is deepened to create a deeper groove for the patella to glide through. This procedure is not common, however may be considered in severe cases. Both osteotomies and trochleoplasties are not appropriate in patients with open growth plates.
Conservative Management
Patients should initially be immobilised in a knee brace in 20˚ of knee flexion for a short term period (2-4 weeks) to allow soft tissues to heal. Throughout this period analgesia, ice and NSAIDs can be employed to reduce pain and swelling. Weight bearing is allowed as soon as pain tolerates. Early mobilisation is important to regain range of motion and joint cartilage trophicity.
Physiotherapy Rehabilitation
Whether surgical or conservative management is undertaken, a period of rehabilitation is required for a full return to normal function as well as any sporting endeavours. Research suggests that physiotherapy management should focus on muscle strengthening and proprioception. Physiotherapist’s will prescribe a progressive strengthening exercise programme targeting muscles that cross the knee joint as well as the wider kinetic chain. Vastus medialis strengthening has traditionally been a focus in rehabilitation, as it was thought that insufficiency contributes to a lateral dislocation. However, this theory is not supported in the literature and therefore vastus medialis strengthening constitutes one element of a rehabilitation program, as part of a global quadriceps strengthening regime.
Return to Sport
During the final phase of the rehabilitation programme, sports specific activities should be also considered. The athlete needs to be prepared for the individual demands of their chosen sport, and exercise programs will target specific needs. In particular cutting manoeuvres, changes of direction and running on uneven ground are the three activities that pose the greatest risk of patellar dislocation. Therefore, in the final stages of rehabilitation the athlete must be prepared to perform these tasks, by use of specific exercises on different surfaces.
There is currently no validated evidence in the literature with specific timelines for a safe return to sport. It is therefore recommended to use criteria-based progression, instead of time-based for rehabilitation and return to sport, which requires patients to reach individual criteria for progression between stages and eventual return to sport. This allow for a more individualised approach, which can be more easily tailored to incorporate a patients specific progress and needs.
The following criteria for return to sport after patellofemoral instability were developed during the 2013 International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine meeting;
- Complete radiographic healing of bone (if bony surgery involved)
- Full or near full range of motion
- No knee effusion (swelling)
- No complaints of knee pain or instability
- Satisfactory core strength and endurance
- Completed neuromuscular training/proprioception
- Acceptable control with dynamic activities
- Limb Symmetry Index greater than 90% on hop tests
- Adequate performance with a physical therapist during sport-specific drills simulating the intensity and movement patterns of the given sport
- Athlete demonstrates a psychological readiness to return to sport (SANE score greater than 80/100)
These criteria can be applied to patients treated both surgically or conservatively.
(10).
Strength Testing
Isokinetic strength testing assesses the strength of knee flexion (hamstrings) and knee extension (quadriceps) in both legs using a dynamometer. The contralateral, unaffected limb is used as a control measure and a Limb Symmetry Index (LSI) is calculated. An LSI of at least 90% should be reached prior to return to sport (10).
Dynamic Stability
Common dynamic stability tests include; star balance excursion test, single leg squat, lateral hop, drop jump. Tests can be assessed both quantitatively and qualitatively. Test results are also interpreted using LSI and 90% is the benchmark. Video analysis can also be a useful tool for qualitative assessment of dynamic movements, both for the purposes of education and guidance during the rehabilitation process, as well as for return to sport testing (10, 11).
At POGO Physio we use ForceDecks, as well as video analysis, to obtain both qualitative and quantitative data for a variety of dynamic stability tests, including single leg squats, balance tasks and hop / jump tests.
Psychological Readiness
Psychological readiness is a significant factor in the return to sport process. A 2021 study investigated reasons behind a failure to return to sport in patients post lateral dislocation and MPFL reconstruction. The most common reason for failure to return to sport was a lack of psychological readiness, with a fear or re-injury or a lack of confidence in performance abilities as common reasons (10). A strong educational base and open communication between treating team and patients is required, with regular conversations surrounding confidence and psychological readiness.
Summary
Patella dislocations occur most commonly from a non-contact twisting injury to the knee. Patella dislocations are most common in active adolescents or those in their second or third decade. There are several anatomical factors that predispose individuals to patellar dislocations. Imaging should be undertaken to assess osteochondral structure and extent of injury following a patellar dislocation to determine best management. Surgical management should be considered in cases with osteochondral fractures, significant intra-articular joint disruption, major tear of the medial stabilisers, most importantly the MPFL, or in the case of recurrent dislocation. Surgical management is superior to conservative management in the sole domain of re-dislocation rate, however there is no significant difference between all other outcomes in the long term. Physiotherapy management following patellar dislocation aims to restore muscular strength, proprioception and neuromuscular control, with the goal of a full return to regular activities, including sport. End stage rehabilitation focuses on preparing athletes for the specific demands of their chosen sport. Return to sport testing involves meeting the listed criteria for a safe return to sport.

Eliana Lonsdale (APAM)
POGO Physiotherapist
Book an appointment with Eliana today
Featured in the Top 50 Physical Therapy Blog
References
- Hayat Z, El Bitar Y, Case JL. Patella Dislocation. [Updated 2021 Jul 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538288/
- Stefancin, J. J., & Parker, R. D. (2007). First-time Traumatic Patellar Dislocation: A Systematic Review. Clinical Orthopaedics and Related Research®, 455. Retrieved from https://journals.lww.com/clinorthop/Fulltext/2007/02000/First_time_Traumatic_Patellar_Dislocation__A.16.aspx
- Hing, C. B., Smith, T. O., Donell, S., & Song, F. (2011). Surgical versus non‐surgical interventions for treating patellar dislocation. Cochrane Database of Systematic Reviews(11). doi:10.1002/14651858.CD008106.pub2
- Nikku, R., Nietosvaara, Y., Aalto, K., & Kallio, P. E. (2009). The mechanism of primary patellar dislocation. Acta Orthopaedica, 80(4), 432-434. doi:10.3109/17453670903110634
- Duthon, V. B. (2015). Acute traumatic patellar dislocation. Orthopaedics & Traumatology: Surgery & Research, 101(1, Supplement), S59-S67. doi:https://doi.org/10.1016/j.otsr.2014.12.001
- Bailey, Chris., (2022). Kneecap Disorders. Retrieved from https://www.chrisbaileyorthopaedics.com/conditions/kneecap-disorders/
- Lee, D.-Y., Park, Y.-J., Song, S.-Y., Hwang, S.-C., Park, J.-S., & Kang, D.-G. (2018). Which Technique Is Better for Treating Patellar Dislocation? A Systematic Review and Meta-analysis. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 34(11), 3082-3093.e3081. doi:https://doi.org/10.1016/j.arthro.2018.06.052
- Schneider, D. K., Grawe, B., Magnussen, R. A., Ceasar, A., Parikh, S. N., Wall, E. J., Colosimo, A. J., Kaeding, C. C., & Myer, G. D. (2016). Outcomes After Isolated Medial Patellofemoral Ligament Reconstruction for the Treatment of Recurrent Lateral Patellar Dislocations: A Systematic Review and Meta-analysis. The American journal of sports medicine, 44(11), 2993–3005. https://doi.org/10.1177/0363546515624673
- Xing, X., Shi, H., & Feng, S. (2020). Does surgical treatment produce better outcomes than conservative treatment for acute primary patellar dislocations? A meta-analysis of 10 randomized controlled trials. Journal of Orthopaedic Surgery and Research, 15(1), 118. doi:10.1186/s13018-020-01634-5
- Ménétrey, J., Putman, S., & Gard, S. (2014). Return to sport after patellar dislocation or following surgery for patellofemoral instability. Knee Surgery, Sports Traumatology, Arthroscopy, 22(10), 2320-2326. doi:10.1007/s00167-014-3172-5
- Sherman, S. L., Deasis, D. P., Garrone, A. J., Voss, E. E., & Oliver, H. A. (2018). Return to Play after Patellar Stabilization. Current reviews in musculoskeletal medicine, 11(2), 280-284. doi:10.1007/s12178-018-9484-1




