


Different Types of Ankle Sprains and Implications for Recovery

Different Types of Ankle Sprains and Implications for Recovery
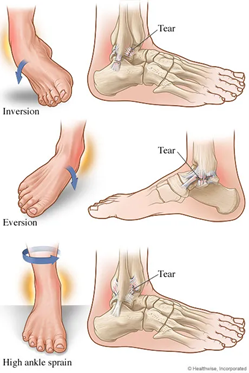
A Lateral ankle sprain is the most common musculoskeletal injury in a physically active population (1). A lateral ankle injury also known as an inversion sprain occurs when the foot plants and the ankle rolls outwards causing injury to numerous tissues of the foot and ankle. Whilst many sprains are often considered minor and innocuous, unfortunately many individuals will experience significant pain and impairment initially, many have injury recurrence, with some going on to develop chronic ankle instability and ongoing pain. It is important to recognise and understand the large variety of injuries that can occur from an ankle sprain and the implications for a successful recovery.
Incidence and Mechanism of Injury
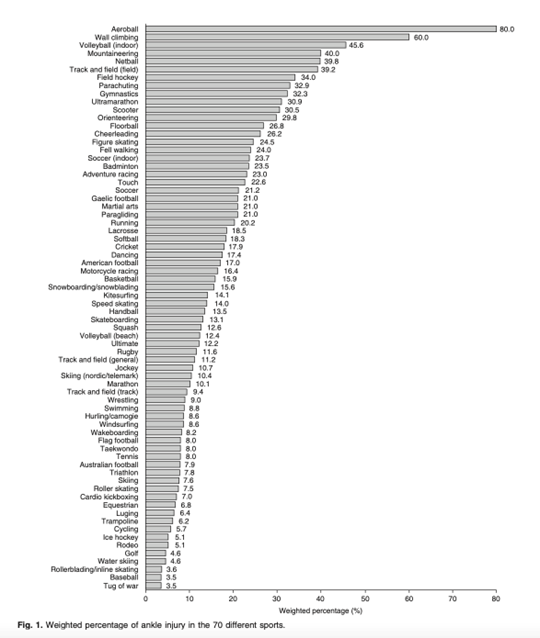
Lateral ankle sprains are the most common musculoskeletal injury and typically occur with forced plantar flexion and inversion of the foot. The different injuries that occur from this common mechanism differ depending upon the degree of plantar flexion, the speed of sprain, twisting or rotation forces and if the sprain occurs with a fall from height or impact. Individuals who suffer an ankle sprain are more likely to reinjure the same ankle (1- 4) which can result in disability and can lead to chronic pain or instability in 20–50% of these cases (5). In addition to recurrent sprains and ease of giving way other residual problems include pain (30.2%), instability (20.4%), crepitus (18.3%), weakness (16.5%), stiffness (14.6%) and swelling (13.9%). For ankles sprained one to four times, the major residual problem is pain (24–28%). For ankles sprained more than five times, instability problems arise, and become a precursor to further injury (2). The figure below shows the percentage of injuries that happen at the ankle in numerous sports.
Anatomy
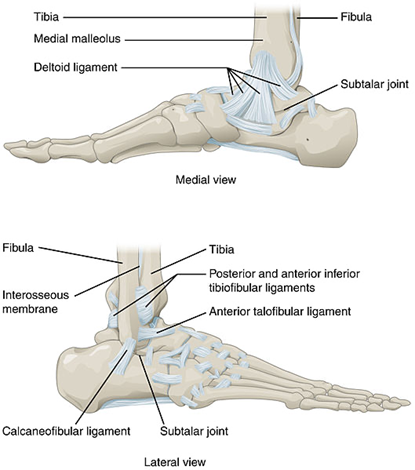
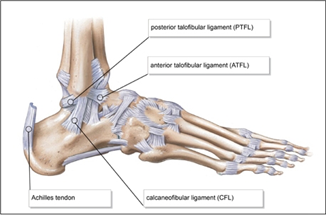
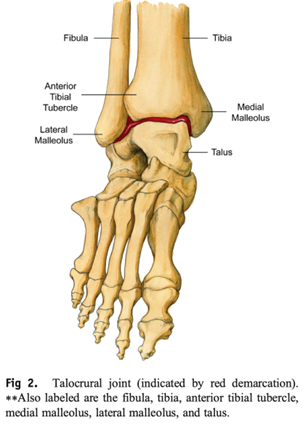
The ankle joint connects the shin to the foot and consists of 2 separate joints: the talocrural joint (TCJ) (ankle mortise) and the subtalar joint (STJ). The TCJ consists of the articulation of the distal aspect of the tibia and fibula with the talus. The distal aspect of the tibia and fibula forms a protective housing that surrounds and articulates with the superior aspect of the body of the talus, the trochlea. The medial border of the housing consists of the medial malleolus, the distal portion of the tibia; the superior border consists of the tibia horizontally; and the lateral border consists of the lateral malleolus, the distal portion of the fibula. The lateral ankle has 3 primary stabilising ligaments; the anterior talofibular ligament which branches from the front of the ankle on the talus to the front of the fibula. The Calcaneofibular ligament which travels from the calcaneus to the bottom of the fibula. The third ligament is the posterior talofibular ligament travels from the back of the fibula to the back of the talus. On the inside of the ankle is the thickened fan shaped deltoid ligament. This is illustrated in the images below.
Anterior Talofibular Ligament Sprain
The Anterior Talofibular Ligament (ATFL) is the first structure injured in the majority of ankle sprains. The ATFL resists pathological inversion and plantar flexion of the ankle joint and is the weakest of the lateral ligaments (2, 7). Estimates are 70-80% of sprains involve the ATFL (2). Injuries to the ATFL are often what many consider a typical ankle sprain with anterolateral pain and swelling, stiffness and positive clinical test (anterior drawer). Sprains can be diagnosed as grade 1 – small tear of the ligament, grade 2 – moderate tear of the ligament or grade 3 – rupture of the ligament. Grade 1-3 sprains can often be treated very similarly with higher grades requiring longer to return to full strength. Standard management will look like the following:
- Acute Pain Management
- Rest – a short period of relative unloading of the ankle joint which may include use of a boot or brace
- Ice – pain relief and reduction of selling
- Compression – compression bandaging, taping or a boot can provide additional support and aid in reducing ankle swelling and discomfort
- Elevation – elevation of the ankle assists to decrease swelling
- Progressive Range of Ankle Movement Exercises – this is vital for normal ankle functioning, from activities as simple as standing and walking to more complex tasks your ankle needs to be able to move through its normal ranges.
- Progressive Proprioception Exercises – proprioception is the body’s awareness of its position and its joints position in space, balance training (e.g. single leg stability exercises, change of direction work and hops) is vital to redevelop proprioception in injured ligaments.
- Progressive Strength – restoring optimal strength to ankle ligaments and muscles
- Addressing contributing factors – this may include, but is not limited to strengthening and stretching muscles at the hip or knee, the use of orthotics and alteration of footwear. This is important in reducing risk of recurrence.
- Functional and sport specific training – whether you’re returning to work, running or sports with quick changes in direction (eg. netball, basketball, football), readying your ankle for these impacts and movements is an essential component in ankle rehabilitation and prolonging the health of your ankle. The use of ankle taping or bracing can also be very beneficial.
Calcaneofibular Ligament Sprain
The addition of CFL injury alongside ATFL injury is common with more severe sprains and associated with longer recovery (9). The CFL resists excessive inversion of the ankle joint and is further stressed at the end ranges of dorsiflexion (2, 7). Higher energy is needed to injure the tissue and often other concomitant injuries that can occur, leading to a poorer prognosis for combined ATFL and CFL injury, this is most notable for rupture (Grade 3 sprain) of both ligaments (9). Whilst it is not clear if combined injury leads to greater risk of chronic ankle instability versus ATFL injury alone (9, 10), greater caution during rehab and longer prognosis is expected. It is much more common to utilise strapping, bracing or a boot for rehabilitation with these injuries. It is recommended that a brace or boot utilised for 10 days for grade 3 injuries (10, 11, 12). However, Lamb et al32 reported that patients who wore a below-knee cast for 10 days had recovered function more rapidly by 3 months post injury as compared with patients treated with an elastic bandage. They also reported that the Aircast brace produced similar results to the below-knee cast for ankle function at 3 months.
Deltoid Ligament Sprain
The medial deltoid ligament is a broad, strong, fan-shaped ligament, extending medially on the ankle and is composed of a deep and superficial layer. The medial deltoid ligament becomes taut in ankle eversion, thus becomes injured if excessive eversion forces and external rotation (abduction) of the foot coupled with internal rotation of the lower leg may result in a medial ankle sprain involving the deltoid ligament (13). The deltoid ligament can also become injured in severe lateral sprains with an inversion mechanism. This leads to medial ankle pain and swelling alongside lateral ankle injury. Treatment of deltoid ligament sprain depends in part on concomitant injury, if it happens through an inversion mechanism it is often managed along a similar path to grade 2 and 3 ATFL/CFL sprains. As the deltoid ligament can also be injured with excessive eversion it can occur alongside syndesmosis injuries which is discussed below/
Peroneal Tendon Tear
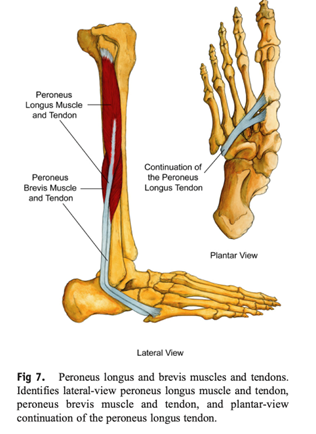
The peroneus longus and peroneus brevis muscles are located on the outside of the leg, and their tendons pass behind the lateral malleolus. The peroneus longus tendon travels diagonally underneath the foot, inserting onto the plantar surface of the medial cuneiform bone and the base of the first metatarsal, whereas the peroneus brevis tendon inserts onto the dorsal surface of the tuberosity of the fifth metatarsal bone (14). Peroneus longus and peroneus brevis evert the foot and provide dynamic support to the lateral ligaments of the ankle. During an inversion ankle sprain with sufficient force (or due to pre-injured lateral ligaments) the peroneus brevis (or longus) muscle and tendon can become rapidly stretched causing injury. This often presents as a split tear (strain) of the tendon behind the lateral malleolus or in some cases the force can cause an avulsion fracture of the 5th metatarsal located on the outside of the foot (15). Similar to a sprain these strains can be classified as grade 1 to 3, with 3 being rupture of the tendon. Rehabilitation for a peroneal tendon injury will look similar to previous discussions on ATFL and CFL rehabilitation with greater emphasis on the various strength deficits (eccentric and concentric) that come from peroneal injury (15). Peroneal Tenosynovitis is another common occurrence after lateral ankle sprain but reflects inflammation of the peroneal tendons and not true damage to the muscle or tendon.
Talar Dome Lesion
The talus is the bone forming the base of the ankle joint that the shin bones sit (tibia and fibula). An osteochondral lesion of the talus or talar dome lesion is a defect in the articular cartilage and underlying cancellous bone on the top surface of the bone (17). The cause of this injury has been debated, but there appears to be a strong link with trauma to the talus during inversion ankle injury, particularly with higher energy sprains or with greater impact forces. A comprehensive review of OLT lesions showed that 76% reported trauma ; 56% of the lesions were medial, and 44% were lateral (24). The mechanism for thelateral talar dome is axial load combined with inversion and dorsiflexion, whereas axial load combined with plantarflexion, inversion, and possibly external rotation results in medial talar dome impaction (26). It is often only detectable with imaging and whilst detectable on x-ray, CT may better show the extent of bone injury. However due to the wide range of other injuries to assess typically associated with this injury MRI is preferred as the initial tool (17).
Management of osteochondral lesions depend on the size of the lesion, with larger lesions associated with poorer outcomes (26). Patients with acute symptomatic lesions that are nondisplaced often are managed with a trial of nonoperative management. This generally consists of a period of 6 weeks of immobilisation with a short leg cast or walking boot followed by a slow progression of return to activity (25, 26). Lesions that become refractory to nonoperative treatment and remain symptomatic for more than 3 to 6 months should be considered for operative treatment. In contrast, acute lesions with displaced fragments should be considered for operative management without a trial of conservative treatment, as they have a lower chance for spontaneous resolution of symptoms (26). Many operative techniques have been described to treat OLTs. They can be grouped into cartilage repair, cartilage regeneration, and cartilage replacement strategies (26).
Syndesmosis
The syndesmotic ligaments consist of the anterior inferior tibiofibular ligament (AITFL), interosseous ligament, posterior inferior tibiofibular ligament (PITFL), and the transverse ligament. The function of the syndesmotic ligaments is to hold the fibula tight to the tibia, thereby preventing abnormal widening of the ankle mortise (14). The AITFL originates from the lateral malleolus of the fibula across the front of the ankle to the tiba, whilst the PITFL connects the tibia and fibula from the back. The interosseous ligament (or interosseous membrane) lies underneath the AITFL and connects the borders of the tibia and fibula. Ankle sprains that produce tenderness proximal to the ankle joint and do not show signs of fracture or diastasis are commonly referred to as syndesmotic or high ankle sprains (16).
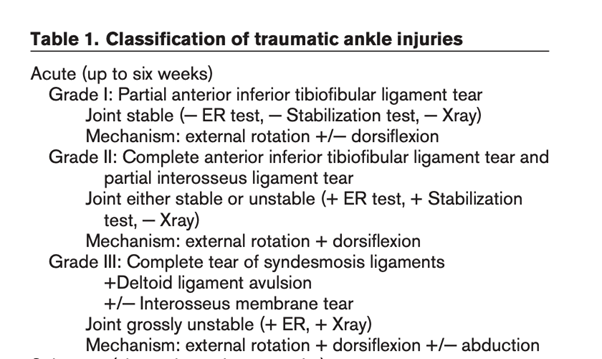
Syndesmotic ankle sprains are generally caused by hyperpronation (external rotation, eversion, and abduction), hyperdorsiflexion or hyper plantar flexion, or another athlete falling onto the fixed ankle (13, 14, 17). Syndesmotic injury can also occur in athletes enduring chronic inversion and axial loading (13, 17). Syndesmotic ankle sprains account for 1% to 11% of all ankle sprains ; however, in athletes, the prevalence rate may range from 40% to 74% of all ankle sprains (17, 18). Most commonly syndesmotic injury involves injury to the AITFL and/or interosseus ligament. Syndesmotic injuries present with symptoms higher up the ankle and medial pain. Often notably swelling and difficulty to weight bear occurs, whilst clinical tests such as squeeze test and external rotation test are positive. These sprains are treated more conservatively than lateral ankle sprains. Classification into Grade 1 to 3 is based on degree of injury and also presence of instability (see table 1) (24).
Acute management requires immobilisation (non weight bearing, walking boot, casting, or bracing) for a time period sufficient to allow healing and functional return (17, 19 , 20). This may be up to 3 weeks (non-weight bearing for some of this time) for grade 1 injuries and stable grade 2 (20, 23). Weight bearing x-ray should be used to assess for widening of the ankle mortise, which often occurs with grade 3 injuries. Surgical fixation should be considered for syndesmotic ankle sprains that demonstrate widening of the ankle mortise greater than 2 mm or joint incongruity on standard or stress radiographs (21). There is a challenge in assessing and determining differences between Grade 1 and 2 injuries and it is advocated towards early imaging with MRI to determine this (17). Using this information and clinical assessment of instability may better determine those athletes who would have quicker return to sport with early surgery for unstable grade 2 injuries (23, 17). In an elite sporting context some athletes have returned to sport at 6 weeks post surgery (22, 23), however expected time to recovery is typically longer (9-12 weeks).
Fracture
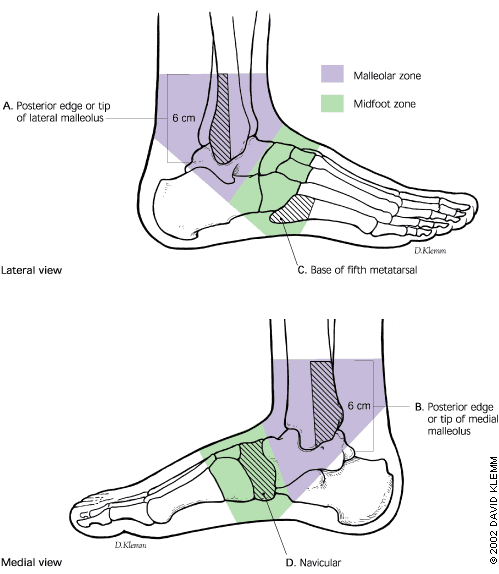
During an inversion ankle sprain, fracture of the shin or foot occurs in up to 15% of cases (28). The most common locations are the lateral malleolus of the fibula, medial malleolus of the tibia, the 5th metatarsal and the navicular. The Ottawa ankle rules were developed to help identify individuals with potential fracture or fractures (28). The ankle assessment covers the ability to walk four steps (immediately after the injury or at the emergency department) and notes localised tenderness of the posterior edge or tip of either malleolus, tenderness of the navicular or the base of the fifth metatarsal (28, 29).
Fracture management requires immobilisation in a cast or brace. Fractures are often referred to an orthopaedic specialist as specific fractures may benefit from surgery versus conservative management. This may be due to poor blood supply (navicular), avulsion injury needing fixation (5th metatarsal, lateral malleolus or medial malleolus) or fixation.
Navicular fractures can be surgical or nonsurgical. Small avulsion fractures, tuberosity fractures, and nondisplaced body fractures can be managed nonoperatively, with the use of a weight-bearing short leg cast and ultimately a walking boot. Displaced navicular body fractures typically require operative intervention, with the use of open reduction and internal fixation. The goals of operative intervention are anatomic fracture reduction and creation of a rigid bony structure which would allow for early range of motion (30).
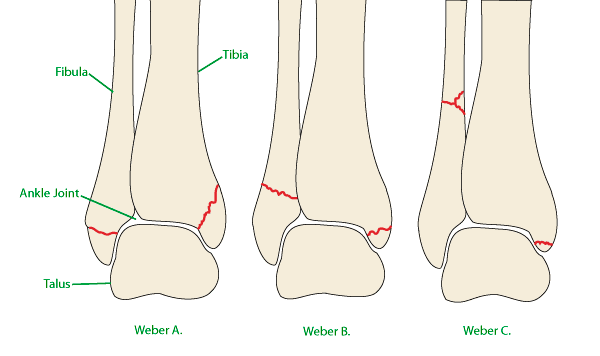
Malleolar fractures are often described with the Danis- Weber classification system (31). Type A is characterised by a transverse fibula fracture at or below the ankle joint and no syndesmotic injury. Type B involves a spiral fibula fracture beginning at the level of the joint and a partial syndesmotic injury. With type C injuries, the fibula fracture is proximal to the ankle joint with associated disruption of the syndesmosis to this level. Type A and B can occur with deltoid ligament injury and fracture of the medial malleolus. Type C includes an avulsion fracture of the medial malleolus or rupture of the deltoid ligament (31). Weber A and B fractures are often treated conservatively in a cast or high top moonboot. Weber C are often referred for surgical management to stabilise the syndesmosis and associated fractures. Recovery after operative management can take up to 6 months with many surgical protocols advocating 6 weeks non-weight bearing before a progressive rehabilitation program.
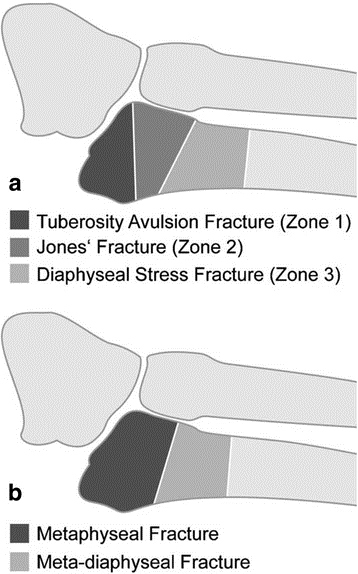
5th metatarsal fractures occur traumatically with the force of the peroneus brevis tendon. Avulsion fractures (zone 1) of the base of the fifth metatarsal are typically treated conservatively with moonboot for 6-8weeks. Fractures that are displaced greater than three millimetres or comminuted are typically realigned and operatively fixed (32). Similarly zone 2 fractures (Jones fractures) are typically referred for orthopaedic opinion as both displaced and nondisplaced fractures may have better resolution and shorter recovery (33, 34). Following resolution of the fracture, typical lateral ankle rehabilitation continues with focus on restoration of range of motion, strength, proprioception and return to sport skills.
Bifurcate Ligament Sprain
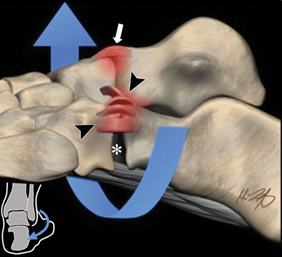
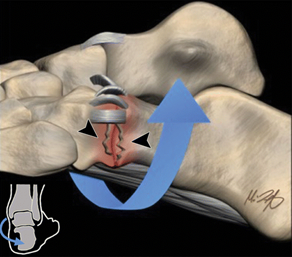
The bifurcate ligament is a ligament that sits on the outside of your foot and assists in stabilising the midfoot. It is a key ligament forming the midtarsal or midfoot. It is attached to the calcaneus (heel bone) with two arms in a Y shape: one that attaches to the cuboid bone (calcaneocuboid ligament), and the other to the navicular bone (calcaneonavicular ligament) (35). Ankle inversion is the most common mechanism implicated in midtarsal sprains accounting for approximately 73% (36). Ankle inversion causes distraction across the anterolateral ankle, stressing the lateral collateral ligaments, commonly causing rupture or avulsion of the ATFL and can also rupture the bifurcate ligament. Ankle eversion is a less common mechanism of injury overall but is a known cause of midtarsal sprains. It creates an opening force on the medial inside of the ankle joint and laterally compression can cause comminuted impaction fractures at the calcaneocuboid joint, sometimes referred to as a “nutcracker-type” fracture whilst injuring the bifurcate ligament (35).
Bifurcate ligament injuries are often overshadowed or mistaken for lateral ankle injury. Reports estimate midfoot sprain is more common, occurring in up to 33% of inversion ankle injuries and in isolation in up to 24% of inversion injuries (36). Clinically, detection of acute midtarsal sprain requires a high index of suspicion. Assessing for swelling, point tenderness or apprehension with ligament stress tests can aid diagnosis. Midtarsal ligament findings on MRI combined with evidence of lateral ankle sprain is associated with a longer time of return to play compared to isolated lateral ligament injuries. A recent study looking at football players revealed time was almost double (47 days versus 24 days) for lateral ankle sprains that were combined with midtarsal joint injury (37).
Summary
It is clear to see that a rolled ankle can be a very simple or very complex injury. The potential for numerous structures to be combined for any ankle sprain can extend and change the rehabilitation path, prognosis or requirement of surgery. Ankle sprains may result in one or more of;
- ATFL Sprain
- CFL Sprain
- Peroneal Tendon Strain
- Deltoid Ligament Sprain
- Syndesmosis Injury
- Osteochondral Lesion of the Talus
- Fracture
- Bifurcate Ligament Sprain

Lewis Craig (APAM)
POGO Physiotherapist
Masters of Physiotherapy
Featured in the Top 50 Physical Therapy Blog
References
- Gribble, P. A., Bleakley, C. M., Caulfield, B. M., Docherty, C. L., Fourchet, F., Fong, D. T. P., … & Delahunt, E. (2016). 2016 consensus statement of the International Ankle Consortium: prevalence, impact and long-term consequences of lateral ankle sprains. British journal of sports medicine, 50(24), 1493-1495.
- Fong DTP, Hong YL, Chan LK, et al. A systematic review on ankle injury and ankle sprain in sports. Sports Med 2007;37:73–94.
- Fong DT, Man CY, Yung PS, et al. Sport-related ankle injuries attending an accident and emergency department. Injury 2008;39:1222–7.
- Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train 2007;42:311–19.
- Nelson AJ, Collins CL, Yard EE, et al. Ankle injuries among United States high school sports athletes, 2005–2006. J Athl Train 2007;42:381–7.
- Waterman BR, Owens BD, Davey S, et al. The epidemiology of ankle sprains in the United States. J Bone Joint Surg Am 2010;92:2279–84.
- Beumer A, van Hemert WLW, Swierstra BA, Jasper LE, Belkoff SM. A biomechanical evaluation of the tibiofibular and tibiotalar ligaments of the ankle. Foot Ankle Int 2003;24 (5):426-9.
- Dubin, J. C., Comeau, D., McClelland, R. I., Dubin, R. A., & Ferrel, E. (2011). Lateral and syndesmotic ankle sprain injuries: a narrative literature review. Journal of chiropractic medicine, 10(3), 204-219.
- Pacheco, J., Guerra-Pinto, F., Araújo, L., Flora, M., Alçada, R., Rocha, T., … & Consciência, J. G. (2021). Chronic ankle instability has no correlation with the number of ruptured ligaments in severe anterolateral sprain: a systematic review and meta-analysis. Knee Surgery, Sports Traumatology, Arthroscopy, 29(11), 3512-3524.
- Crema MD, Krivokapic B, Guermazi A, Gravilovic P, Popovic N, D’Hooghe P, Roemer FW (2019) MRI of ankle sprain: the association between joint effusion and structural injury severity in a large cohort of athletes. Eur Radiol 29(11):6336–6344
- Beynnon BD, Renstrom PA, Haugh L, Uh BS, Barker H. A prospective, randomized clinical investigation of the treatment of first-time ankle sprains. Am J Sports Med. 2006;34(9):1401–1412.
- Lamb SE, Marsh JL, Hutton JL, et al. Mechanical supports for acute, severe ankle sprain: a pragmatic, multicentre, randomised controlled trial. Lancet. 2009;373(9663):575–581.
- Kaminski, T. W., Hertel, J., Amendola, N., Docherty, C. L., Dolan, M. G., Hopkins, J. T., … & Richie, D. (2013). National Athletic Trainers’ Association position statement: conservative management and prevention of ankle sprains in athletes. Journal of athletic training, 48(4), 528-545.
- Dubin, J. C., Comeau, D., McClelland, R. I., Dubin, R. A., & Ferrel, E. (2011). Lateral and syndesmotic ankle sprain injuries: a narrative literature review. Journal of chiropractic medicine, 10(3), 204-219.
- Egol K, Walsh M, Rosenblatt K, Capla E, Koval KJ. Avulsion fractures of the fifth metatarsal base: a prospective outcome study. Foot Ankle Int. 2007;28(5):581–583.
- Nussbaum ED, Hosea TM, Sieler SD, Incremona BR, Kessler DE. Prospective evaluation of syndesmotic ankle sprains without diastasis. Am J Sports Med. 2001;29(1):31–35.
- Amendola A, Williams G, Foster D. Evidence-based approach to treatment of acute traumatic syndesmosis (high ankle) sprains. Sports Med Arthrosc. 2006;14(4):232–236.
- Veenema KR. Ankle sprain: primary care evaluation and rehabilitation. J Musculoske Med September 2000:563-76.
- Kim S, Huh Y, Song H, et al. Chronic tibiofibular syndesmosis injury of ankle: evaluation with contrast-enhanced fat-suppressed 3D fast spoiled gradient-recalled acquisition in the steady state MR imaging. Radiology. 2007;242(1):225–235.
- Lin CF, Gross ML, Weinhold P. Ankle syndesmosis injuries: anatomy, biomechanics, mechanism of injury, and clinical guidelines for diagnosis and intervention. J Orthop Sports Phys Ther. 2006;36(6):372–384.
- Beumer A, Valstar ER, Garling EH, et al. Effects of ligament sectioning on the kinematics of the distal tibiofibular syndesmosis: a radiostereometric study of 10 cadaveric specimens based on presumed trauma mechanisms with suggestions for treatment. Acta Orthop. 2006;77(3):531–540.
- Taylor, D. C., Tenuta, J. J., Uhorchak, J. M., & Arciero, R. A. (2007). Aggressive surgical treatment and early return to sports in athletes with grade III syndesmosis sprains. The American journal of sports medicine, 35(11), 1833-1838.
- Wolf BR, Amendola A. Syndesmosis injuries in the athlete: when and how to operate. Curr Opin Orthop. 2002;31:151–154.
- Tol JL, Struijs PA, Bossuyt PM, Verhagen RA, van Dijk CN. Treatment strategies in osteochondral defects of the talar dome: a systematic review. Foot Ankle Int. 2000;21(2):119–126.
- Zengerink M, Szerb I, Hangody L, Dopirak RM, Ferkel RD, van Dijk CN. Current concepts: treatment of osteochondral ankle defects. Foot Ankle Clin. 2006;11:331–359
- Berndt, AL, Harty, M. Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am. 1959;41A:988–1020.
- Steele, J. R., Dekker, T. J., Federer, A. E., Liles, J. L., Adams, S. B., & Easley, M. E. (2018). Osteochondral lesions of the talus: current concepts in diagnosis and treatment. Foot & Ankle Orthopaedics, 3(3), 2473011418779559.
- Bachmann, L. M., Kolb, E., Koller, M. T., Steurer, J. & Gerben ter, R. (2003). Accuracy of Ottawa ankle rules to exclude fracture of the ankle and mid-foot: a systematic review. British Medical Journal, 326, 417.
- Stiell, I. G., McKnight, R. D., Greenberg, G. H., et al. (1994). Implementation of the Ottawa Ankle Rules, JAMA, 271, 827-832.
- Rosenbaum AJ, Uhl RL, DiPreta JA. Acute fractures of the tarsal navicular. Orthopedics. 2014 Aug;37(8):541-6
- Harper, M. C. (1992). Ankle fracture classification systems: a case for integration of the Lauge-Hansen and AO-Danis-Weber schemes. Foot & ankle, 13(7), 404-407.
- Quill GE. Fractures of the proximal fifth metatarsal. Orthop Clin North Am. 1995;26:353–361
- Baumbach, S. F., Prall, W. C., Kramer, M., Braunstein, M., Böcker, W., & Polzer, H. (2017). Functional treatment for fractures to the base of the 5th metatarsal-influence of fracture location and fracture characteristics. BMC Musculoskeletal Disorders, 18(1), 1-7.
- Bowes, J., & Buckley, R. (2016). Fifth metatarsal fractures and current treatment. World journal of orthopedics, 7(12), 793.
- Walter WR, Hirschmann A, Tafur M, Rosenberg ZS. Imaging of Chopart (midtarsal) joint complex: normal anatomy and posttraumatic findings. AJR Am J Roentgenol 2018;211(2):416–425.
- Walter, W. R., Hirschmann, A., Alaia, E. F., Garwood, E. R., & Rosenberg, Z. S. (2018). JOURNAL CLUB: MRI evaluation of midtarsal (Chopart) sprain in the setting of acute ankle injury. American Journal of Roentgenology, 210(2), 386-395.






