


Persistent Pain Recovery is Possible

The broader medical field has made wonderful advances in the diagnosis and treatment of complex conditions over the past 100 years. Whether it’s the vaccine developed for Polio, that prevented millions of people experiencing its horrible irreversible neurological effects, or the discovery by Australian pathologist Dr Robin Warren that Stomach Ulcers were caused by a simple bacteria H. Pylori, which led to a revolution in treatment for the disabling condition that plagued many people for decades. Medical science and treatment can, and has done many wonderful things.
One thing however, that it has not done well is diagnose, understand and treat complex and persistent pain conditions. Whether it’s vague and still poorly understood diagnoses like ‘fibromyalgia’ and ‘failed back surgery syndrome’, or the ever burgeoning opioid epidemic, and rising rates of chronic pain globally despite enormous spending on different treatments. We aren’t very good at managing pain, and we’re starting to realise why.
Why it hasn’t worked so far
Medicine and Allied Health professions like Physiotherapy operate largely from what we can call a ‘reductionist worldview’. The Oxford dictionary defines ‘reductionist’ as “a person who believes that complicated things can be explained by considering them as a combination of simple parts” 1. Put simply, it’s the idea that we can understand and resolve problems in a system like the human body by finding the ‘faulty part/s’ and fixing or replacing them. We needn’t look far to see evidence of the ubiquity of this approach – from joint replacement surgeries to injections and nerve ablation procedures, we continually see that medicine assumes pain is an ‘issue in the tissue’ that can be fixed by zooming in on the problem.
Physiotherapy isn’t immune from this either. Throughout our history, we’ve been guilty of the same approach. ‘Strap it, massage it, strengthen it, and she’ll be right mate’. Whilst this approach isn’t without merit, it certainly has and continues to help many people. When it comes to complex and persistent pain, it simply does not work.
The reason why it doesn’t work is because complex and persistent pain is usually never just an issue with one tissue. The symptoms, and subsequent disability arise because of an emergent interaction between a range of factors; biological, psychological and social. Take for example the growing body of evidence 2-7 that adverse childhood experiences are associated with the subsequent development of persistent pain. Or the fact that people with lower socioeconomic status have a higher likelihood of experiencing chronic pain and poorer health outcomes8.
Even from a purely biological viewpoint, we now know many chronic pain conditions arise from complex changes across the nervous, immune and hormonal (endocrine) systems, in addition to the ‘original’ site/s of tissue damage, if there were any 9-10. I could write paragraphs listing out all the latest isolated biological theories about potential ‘causes’ of chronic pain, but I don’t believe it would be helpful. Because until there is ample evidence to prove otherwise, the answer to recovering from chronic or persistent pain lies not in finding an isolated cure, but in zooming out, seeing the system of you as a whole and how you interact with the many other systems of your life. And then making a few changes progressively in line with both your values and personal goals to make these systems work better in your favour.
How it can work
1. Know where you want to go, then get a good map and guide
The journey to persistent pain recovery is first and foremost unique to each individual, not just in how it looks or how long it takes, but what recovery even means to each individual. Pain Rehabilitation specialist Alison Sim expresses in this great blog about pain recovery tips from people who’ve walked the journey, that you first need to define what recovery means for you. Whilst it is possible to overcome debilitating pain, it doesn’t necessarily mean we can get rid of pain entirely. Recovery may not mean you want to go back to life as it was before you had persistent pain. One of the most important steps in Pain recovery we are learning more about each year, is the role of acceptance in healing11.
Acceptance is often misconstrued as giving up or accepting defeat, rather than its more optimistic and powerful meaning of meeting reality as it is. Only in doing that can any of us work to change for the better, and make goals that are achievable and in line with our values. This process usually requires the guidance and support of a skilled Pain Physiotherapist &/or Psychologist, to help you understand where you’re at and define clearly where you want to go, and what’s required to get you there.
Any good traveller always needs a reliable map before they head off on their journey. The ‘maps’ commonly provided to people experiencing persistent pain have been substandard at best, focusing on specific damaged tissues and the view of the human body as a machine, instead of the adaptive biological system it is. The better maps lie in the Biopsychosocial and enactive models of health and illness. Like the feeling you had using google maps for the first time after navigating using a phone book, understanding these models and what they mean for you can be liberating.
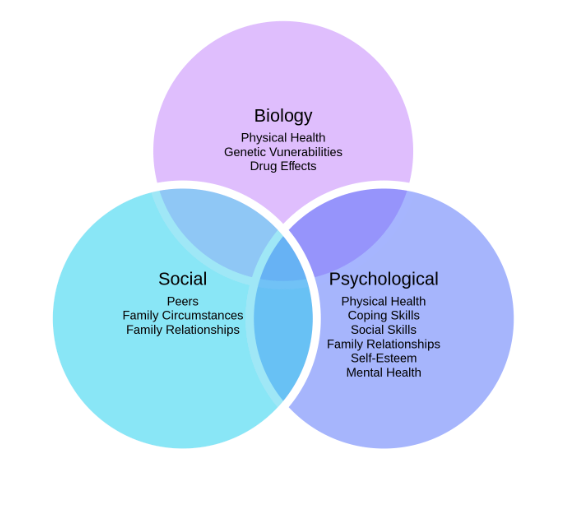
The Biopsychosocial (BPS) model of disease and health is a great place to start with building your new map for pain recovery. It helps you see beyond the particular injuries and tissue damage you’ve experienced to understand how social and psychological factors can alter your pain experience. However, like the eggs, flour and milk in a pancake, the biological, psychological and social factors that make up our pain experience all contribute, but can’t be separated once the pancake (pain experience) is made. But it does help us better understand how our pain behaves, and what we can do to better manage it in the future.
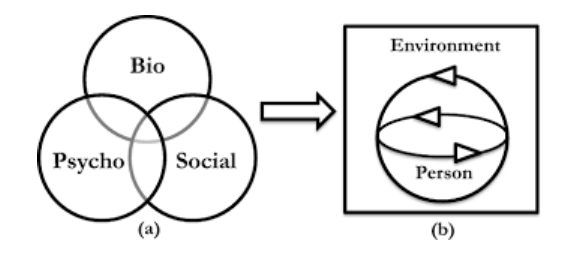
Another great map that pairs well with the BPS model for making sense of pain is the enactive model. Even zooming in on a person to see their biological, psychological and social factors still misses the fact that they are inseparable from their wider environment. Consider how differently you feel and behave when you move town or travel in a new country. The environment we find ourselves in, is from one perspective a continuous part of us, if we look at ourselves from a more embodied fluid perspective. Which the enactive model calls us to do.
On first glance these two models can be a tad overwhelming and confusing. The essential message of both is that health and illness arise from a combination of factors, from our environment, our job and family, to our thoughts and feelings and the specific state of our tissues. If you take the time to reflect on each aspect (especially with the guidance of a health professional) it can bring considerable insight into your symptoms and lifestyle, giving you many avenues to better manage and improve your health and quality of life.
But how exactly?
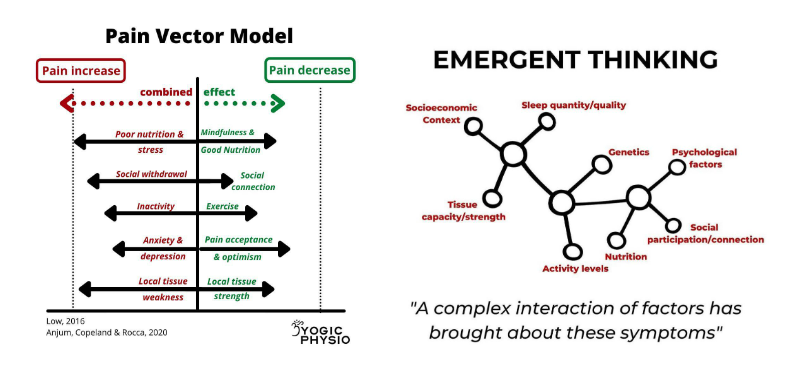
If we consider the fact that pain emerges as a protective mechanism from many bodily system interactions to indicate potential tissue damage, then it invites us to find out why our body feels we need protection. This can be due to a whole range of interacting factors, examples of which are listed below:
- Local tissue is inflamed or injured
- Local tissue weakness/poor capacity
- Consistent disturbed/reduced sleep
- Systemic inflammation/Autoimmune activity
- Heightened stress levels
- Anxiety &/or depression
- Low physical activity levels
These factors never work in isolation but together in a complex emergent pattern. But a picture speaks a thousand words as they say, see the images below for an example of how pain arises:
2. Learn & Practice Self-Regulation Skills
A good adventurer first organises their map, knows where they wish to go and how best to get there. Then they prepare their body for the journey and obtain the equipment they need. Similarly, someone on a recovery journey from persistent pain first understands their pain and context from a broader BPS perspective, clarifies some personal goals (small and big) before building the skills and capacity to go on the journey.
People often misperceive injury and pain rehabilitation as just massage and exercise. But there’s a lot more nuance to the process. And when it comes to Persistent Pain, there is a real need to develop specific skills around what I call self or auto-regulation; ‘the process by which a person adapts/adjusts their responses in the face of stressful situations or stimuli’.
As we know already, Persistent pain can be worsened, and even partly brought about by prolonged stressors. It can thus be really helpful to learn and develop newer and healthier coping mechanisms in the face of these stressors. Common skills and strategies include:
- Sleep ‘hygiene’ practices – e.g. keeping consistent and regular sleeping schedules, or avoiding certain foods/drinks within a few hours of bed time. Sleep quality and quantity can have an impact on our pain 12-13.
- Mindfulness practices – mindful walking, sitting &/or breathing is almost essential for people to live well in the face of the hustle and bustle of modern life these days, even more so for those in pain. It’s even been shown to help reduce pain in scientific research 14-15. These practices may help us relax and downregulate our stress, but their primary use in changing our relationship to pleasant and unpleasant sensory experiences, so we can develop less reactivity and more equanimity.
- Relaxation practices – sometimes we just need to give our bodymind time and space to be and relax without any commitments or to do lists bugging us. My favourite way to just relax and let things settle is ‘lying rest pose’ from yoga, or lying with my legs elevated and some relaxing music playing. Whatever this is for you, it’s about finding some time to just be still and let be.
- Stress management skills – whilst we can improve our state and tolerance to stress through mindfulness, breathing and relaxation techniques, seeing a psychologist for guidance and help in learning other cognitive strategies tailored to our unique situation can be immensely helpful. This may involve time management skills, or emotional regulation practices for example. Research shows learning these things can improve recovery from complex conditions like Whiplash 16.
- Appropriate nutrition – it can be immensely helpful to engage the help of an accredited practising dietitian to review your nutrition and optimise it for your goals and recovery.
- Breathing practices – originally arising from various Yoga traditions, breath regulation practices provide a direct window into the autonomic nervous system, that allows us to change and alter our state to be more in rest and digest/ parasympathetic nervous system dominance. This is important because it can not just make us feel more calm and grounded, but it has also been proven to reduce our pain intensity and unpleasantness 17-19.
3. Graded Exposure Plan towards Valued activities
Once we’ve learned some ideas and skills to better regulate our nervous system and wider physiology, we can then feel more equipped and ready to engage in what is probably the most important and well understood principle of pain recovery – graded exposure. From chronic low back pain, to the still poorly treated complex regional pain syndrome, we have evidence to suggest that graded activity or exposure has positive effects in the short, medium and long term in pain, quality of life and disability levels 20-22.
Graded exposure involves the slow, intelligent and progressive engagement in valued activities that we find painful. This is done under the guidance of an experienced Physiotherapist until you are independently completing your desired activity/ies without pain inhibiting you. Whilst this process is seemingly simple in principle, in practice it can be quite challenging and different for everyone. Nor is the process a simple linear progression from doing nothing to doing what you used to before in a few weeks or months time, as you can see in the image below.
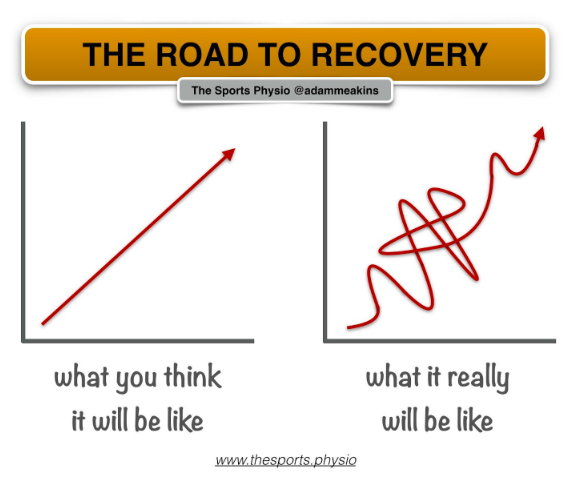
The beauty of the graded exposure process of rehabilitation is that it looks very different for everyone. One example may be pain limiting you walking upstairs. An experienced Physiotherapist will assess your current capacity and tolerance, and work with you to build an exercise plan that not only gets you walking more over time, but improves the sensitivity and strength of your legs and feet for example. Within the broader graded exposure/activity paradigm are a range of tools that are invaluable for recovery from persistent pain. Examples listed below include:
- Pacing – involves spacing out provocative activities across the day to limit or prevent pain aggravation. When spaced out over days/weeks it can also prevent the common pattern of boom and bust cycles where you overshoot your current capacity by doing too much, then find yourself unable to do basic daily activities due to a pain flare.
- Mirror therapy – a mirror is placed in a position so that the patient can view a reflection of a body part, which helps reduce the threat response associated with using the actual injured or painful limb, allowing graded exposure into different movements of the limb.
- Graded motor imagery – technically part of mirror therapy. Graded motor imagery involves using imagined movements of the painful part of your body, particularly types of movements and contexts that would be provocative if the movements were physically performed. It is thought to lead to neuroplastic changes in the central nervous system (brain and spinal cord) that help reduce sensitivity to these movements and allow them to be performed physically.
- Graded movement/exercise – finding some form of exercise if meaningful and valuable to you, performing it at a low and tolerable dosage. Then progressively working over a period of time to increase the dosage as tolerated.
Graded exposure works on a range of levels by inducing what we call bioplasticity; “the idea that any system or tissue in our body has the capacity to change and adapt to the stressors placed on it”. This plasticity can be seen simplistically from something like strength training, where we aim to improve the contractile force of our muscles, potentially growing them in size in the process. It can also be understood in a more complex way from the varied changes and interactions that occur across nervous, immune, endocrine (hormonal) and musculoskeletal systems when we ask our body to do a little more than it is used to. Ultimately it’s a flexible and individualised approach that gets you from where you are to where you want to be, working to stimulate and change your body in the process to be stronger, less sensitive and more able to do the things you love.
Where to now?
Persistent Pain is still a poorly understood and treated problem. Whilst we don’t have all the answers, we know enough to treat people with pain much much better than they are by standard medical interventions. Humans are complex biological organisms that require treatment approaches which fully appreciate this complexity, rather than mistakenly viewing us from a mechanical and reductionist perspective. By considering your personal context and biopsychosocial factors and experience, setting some clear attainable short and long term goals and learning ways to better regulate and expose your bodymind to stressors and valued activities, I believe recovery from Persistent pain is possible.
If you are experiencing complex or persistent pain and want a fresh approach to recovery – book in with our Pain Physiotherapist Oliver Crossley.

Oliver Crossley (APAM) POGO Physiotherapist
Book an appointment with Oliver here
Featured in the Top 50 Physical Therapy Blog
References
- Reductionist_1 noun – Definition, pictures, pronunciation and usage notes | Oxford Advanced Learner’s Dictionary at OxfordLearnersDictionaries.com. (2023). Oxfordlearnersdictionaries.com. https://www.oxfordlearnersdictionaries.com/definition/english/reductionist_1?q=reductionist
- Linton SJ. A population-based study of the relationship between sexual abuse and back pain: establishing a link. Pain. 1997;73(1):47–53. 21.
- Brown RC, Plener PL, Braehler E, Fegert JM, Huber-Lang M. Associations of adverse childhood experiences and bullying on physical pain in the general population of Germany. J Pain Res. 2018;11:3099–108. 22.
- You DS, Albu S, Lisenbardt H, Meagher MW. Cumulative childhood adversity as a risk factor for common chronic pain conditions in young adults. Pain Med. 2018;20(3):486–94. 23.
- Davis DA, Luecken LJ, Zautra AJ. Are reports of childhood abuse related to the experience of chronic pain in adulthood?: a meta-analytic review of the literature. Clin J Pain. 2005;21(5):398–405. 24.
- Sachs-Ericsson N, Kendall-Tackett K, Hernandez A. Childhood abuse, chronic pain, and depression in the National Comorbidity Survey. Child Abuse Negl. 2007;31(5):531–47.
- Hughes, K., Bellis, M. A., Hardcastle, K. A., Sethi, D., Butchart, A., Mikton, C., … & Dunne, M. P. (2017). The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. The Lancet Public Health, 2(8), e356-e366.
- Khalatbari-Soltani, S., & Blyth, F. M. (2022). Socioeconomic position and pain: a topical review. Pain, 163(10), 1855-1861.
- Kiverstein, J., Kirchhoff, M. D., & Thacker, M. (2022). An Embodied Predictive Processing Theory of Pain Experience. Review of Philosophy and Psychology, 1-26.
- Bonanni, R., Cariati, I., Tancredi, V., Iundusi, R., Gasbarra, E., & Tarantino, U. (2022). Chronic Pain in Musculoskeletal Diseases: Do You Know Your Enemy?. Journal of Clinical Medicine, 11(9), 2609.
- Veehof, M. M., Trompetter, H. R., Bohlmeijer, E. T., & Schreurs, K. (2016). Acceptance-and mindfulness-based interventions for the treatment of chronic pain: a meta-analytic review. Cognitive behaviour therapy, 45(1), 5-31.
- Sivertsen, B., Lallukka, T., Petrie, K. J., Steingrímsdóttir, Ó. A., Stubhaug, A., & Nielsen, C. S. (2015). Sleep and pain sensitivity in adults. Pain, 156(8), 1433-1439.
- Whibley, D., AlKandari, N., Kristensen, K., Barnish, M., Rzewuska, M., Druce, K. L., & Tang, N. K. (2019). Sleep and pain: a systematic review of studies of mediation. The Clinical Journal of Pain, 35(6), 544.
- Hilton, L., Hempel, S., Ewing, B. A., Apaydin, E., Xenakis, L., Newberry, S., … & Maglione, M. A. (2017). Mindfulness meditation for chronic pain: systematic review and meta-analysis. Annals of Behavioral Medicine, 51(2), 199-213.
- Reiner, K., Tibi, L., & Lipsitz, J. D. (2013). Do mindfulness-based interventions reduce pain intensity? A critical review of the literature. Pain Medicine, 14(2), 230-242.
- Sterling, M., Smeets, R., Keijzers, G., Warren, J., & Kenardy, J. (2019). Physiotherapist-delivered stress inoculation training integrated with exercise versus physiotherapy exercise alone for acute whiplash-associated disorder (StressModex): a randomised controlled trial of a combined psychological/physical intervention. British Journal of Sports Medicine, 53(19), 1240-1247.
- Jafari, H., Courtois, I., Van den Bergh, O., Vlaeyen, J. W., & Van Diest, I. (2017). Pain and respiration: a systematic review. Pain, 158(6), 995-1006
- Wells, R. E., Collier, J., Posey, G., Morgan, F., Auman, T., Strittameter, B., … & Zeidan, F. (2020). Attention to breath sensations does not engage endogenous opioids to reduce pain. Pain, 161(8), 1884.
- Jinich-Diamant, A., Garland, E., Baumgartner, J., Gonzalez, N., Riegner, G., Birenbaum, J., … & Zeidan, F. (2020). Neurophysiological Mechanisms Supporting Mindfulness Meditation–Based Pain Relief: an Updated Review. Current Pain and Headache Reports, 24(10), 1-10.
- Macedo, L. G., Smeets, R. J., Maher, C. G., Latimer, J., & McAuley, J. H. (2010). Graded activity and graded exposure for persistent nonspecific low back pain: a systematic review. Physical therapy, 90(6), 860-879.
- López-de-Uralde-Villanueva, I., Munoz-Garcia, D., Gil-Martinez, A., Pardo-Montero, J., Munoz-Plata, R., Angulo-Diaz-Parreno, S., … & La Touche, R. (2016). A systematic review and meta-analysis on the effectiveness of graded activity and graded exposure for chronic nonspecific low back pain. Pain Medicine, 17(1), 172-188.
- Shafiee, E., MacDermid, J., Packham, T., Walton, D., Grewal, R., & Farzad, M. (2022). The Effectiveness of Rehabilitation Interventions on Pain and Disability for Complex Regional Pain Syndrome; A Systematic Review and Meta-analysis. The Clinical Journal of Pain, 10-1097.
- Low, M. (2017). A novel clinical framework: the use of dispositions in clinical practice. A person centred approach. Journal of evaluation in clinical practice, 23(5), 1062-1070
- Anjum, R. L., Copeland, S., & Rocca, E. (2020). Rethinking causality, complexity and evidence for the unique patient: a causehealth resource for healthcare professionals and the clinical encounter (p. 241). Springer Nature



