


Overuse Knee Injuries in Cyclists

Knee Pain in Cyclists – The Common Culprits
Knee injuries:
The most common site of overuse injury in cyclists of all levels is the knee (5,6) . This is of no surprise considering the repetitive nature of the sport, with cyclists completing in excess of 10,000 pedal revolutions over a 2 hour ride (at an average cadence of 83rpm). There are various potential causes of cycling related knee pain, making accurate diagnosis and specific early management key to successful outcomes. Key differential diagnoses include:
Anterior knee pain:
- Patellofemoral related pain
- Patella tendinopathy
- Quadriceps tendinopathy
- Infrapatellar fat pad impingement
Medial knee pain:
- Pes anserine bursitis
- Medial patellofemoral ligament (MPFL) strain
- Medial plica syndrome
- MCL bursitis
Posterior knee pain:
- Distal hamstring tendinopathy (medially: semimembranosus, laterally: biceps femoris)
- Strain to posterior knee joint capsule
Lateral knee pain:
- ITB syndrome
Here we will take a deeper look into Patellofemoral related pain and ITB syndrome…
Patellofemoral related pain
Background:
PFP is responsible for the majority of knee complaints(3,4,7) and is attributed to the greatest loss of training time in professional cyclists(6,24) . PFP, synonymous with anterior knee pain, is an umbrella term that encapsulates pain originating around or behind the knee-cap. Possible sources of pain include the patella retinaculum, synovial lining, and its bursa, however, the highly innervated subchondral bone is most likely implicated with PFP.
Presentation:
Cyclists typically present with an insidious onset of vague anterior knee pain, around or deep to the knee-cap. Activities that cause compressive loading of the patellofemoral joint such as decline squats and descending stairs will aggravate symptoms. It may progress to becoming quite sharp and felt during the down or power phase of the pedal stroke. There is rarely swelling, episodes of giving way or loss of ROM, however, cyclists may experience crepitus under the patella during loaded knee movements.
There will often be a substantial increase in training volumes preceding PFP symptoms. Factors such as hill climbing
Contributory factors:
Biomechanical
It is thought that i) patellofemoral joint (PFJ) compression forces, ii) frontal plane knee motion (lateral displacement), and iii) rotational forces (torque) at the knee joint are key factors in the development of PFP.
1. Patellofemoral joint compression forces
To better understand the nature of PFP, a simple understanding of joint biomechanics at the knee joint is useful. The patella acts a pulley between the quadriceps and patellar tendons, transmitting extension forces generated by the quads. Using vectors (see diagram below), the resultant force is compressive in nature, pulling the patella against the femur in the intercondylar groove. The magnitude of this compressive force increases as the angle between the quadriceps and patellar tendons decreases (ie moving into knee flexion).
It is important to note that surface contact area between the femur and patella also increases between 30-90degrees of knee flexion (25). Improved joint congruency has the effect of distributing PF compressive forces over a greater surface area. Applying the laws of physics: greater compressive joint forces during knee flexion may be mitigated by increased surface contact area- influencing actual PF joint pressures applied to articular surfaces.
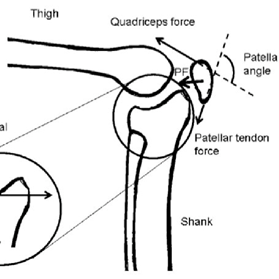
Image 1: Vector analysis of compressive PF joint forces
Source: https://www.researchgate.net/figure/Illustration-of-the-patellofemoral-joint-and-related-forces-quadriceps-patellar-tendon_fig2_321526807
Putting this into practice: a higher saddle results in reduced knee flexion angles and quadricep muscle forces- all of which decrease PF compressive forces. A study by Ericson et al (26) found that saddle height is inversely related to PF joint contact pressures, supporting this theory. However, conflicting findings from other studies (27,28) have suggested that saddle height has limited effect on PF pressures. This may be due to the greater joint surface contact area available to distribute these forces. Despite the debatable evidence, it is recommended that cyclists experiencing PFP increase saddle height so that maximal knee extension is approximately 30degrees (18) .
2. Frontal plane medial knee projection
Medial motion at the knee whilst cycling (dynamic valgus) is thought to cause lateralisation of the patella in the trochlear groove, increasing loading of the lateral PF joint. Studies(29, 30) have found that cyclists with a history of knee pain tend to adopt more medial positions compared to uninjured cyclists. Hannaford et al (30) found that correcting medial knee projection through adjustments at the foot-pedal interface improved symptoms. The mechanism behind cleat/insole wedging will be explained under bike-fit related factors.
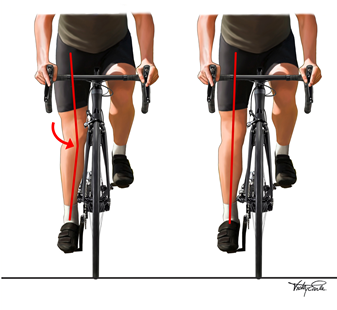
Image 2: Frontal plane medial projection of the knee
Source: https://vearlemedicalart.com/gallery-2/cycling-frontal-knee-motion/
3. Rotational forces at the knee
It has been speculated that fixing the foot onto the pedal interface causes greater rotational forces (torque) at the knee joint. Prior to the introduction of modern clipless pedal systems, the foot could move freely on the pedals, allowing the cyclist to find their neutral foot position and reduce torque at the knee joint. However, by fixing the foot in an unnatural position, any rotation has to be transferred up the kinetic chain towards the knee.
This has led to the invention of ‘floating pedals’ that allow some degree of axial rotation. Wheeler et al (31) have shown that these systems reduce applied moments at the foot pedal interface (without compromising power transmission), which should theoretically reduce torque at the knee joint. It is important to note that sub-optimal cleat positioning rather than fixing the foot onto the pedal is the root cause of the problem. However, attaining the perfect cleat position can be quite cumbersome, especially without paying for a professional bike fit, making floating pedals the preferred choice in cyclists today.
Anatomical and strength risk factors
Non-modifiable anatomical risk factors that increase contact PF pressures include patella alta (32) (knee-cap that sits higher) and trochlear dysplasia (33) (shallow groove for the knee-cap). These reduce the amount of patellofemoral joint contact area, thereby increasing pressure on the sensitive sub-chondral bone (F=PxA). Greater Q angles (natural angle at which femur meets tibia) are associated with patella lateralisation (34), which increases loading of the patella’s lateral facet. This may partly explain why females are at higher risk of developing PFP due to their wider hips. Whilst the contribution of these anatomical factors are important considerations, addressing modifiable risk factors such as training load and muscle strength are key to PFP management.
The importance of gluteal muscle strength cannot be ignored when it comes to PFP. Gluteus maximus is the prime hip extensor and assists concentric work of the quads during the downstroke. Increasing glute max strength and recruitment can reduce relative work of the quads, mitigating compressive forces at the patellofemoral joint.
Glute max is also responsible for hip external rotation, along with deeper muscles such as quadratus femoris, piriformis, and the obturator and gemellus groups. Combined with gluteus medius and minimus which abduct the hip, the 3 glute muscles help control excessive hip adduction and internal rotation. These hip movements are associated with frontal plane medial knee projection and are well established PFP risk factors (35). Strengthening the hip abductors and external rotators have been shown to effectively improve pain and function in those with PFP (36,37).
Quad weakness is not only a major risk factor in the development of PFP (38), but a huge performance limiter. Research (38,39) shows that people with PFP have weaker and smaller quadriceps than those without pain. What is less clear is the significance of VMO activation relative to the lateral quad muscle (VL). A systematic review by Bini et al (40) concluded that “cyclists with over-use related knee pain presented with an altered activation of the vastus medialis and lateralis muscles”. It has been previously believed that relative weakness of the VMO and overactivity of the VL leads to lateral ‘maltracking’ of the patella. On the practical level, it is known that we cannot train the VMO in isolation and that no single exercise preferentially recruits this muscle (41).
Regardless of this debate, it is clear that quad strengthening programs provide both short and long term improvements in pain and function for those with PFP/
Overall, cyclists with or without knee pain should incorporate a combination of hip and knee strengthening into their training on a regular basis. Here are examples of such exercises and progressions:
Early stage:
- Knee extension 45-90deg of knee flexion
- Leg press minimal range
- Quarter squat
- Single leg dip abduction bias
- Single leg deadlift with contralateral weight
- Side plank top leg abduction
- Single leg hip thrust
Mid stage:
- SL sit to stand
- Full range knee extension à progress to SL
- Full range leg press à progress to SL
- Reverse lunge with abduction bias
- Banded goblet squat
End stage:
- Heel elevated squat à progress to SL
- Heel elevated cyclist squat
- High step up
Load related factors:
There will often be a substantial increase in training volumes preceding PFP symptoms. Factors such as hill climbing, riding ‘out of the saddle’, and overgearing work significantly increase demands placed on the quad muscles. These variables must be considered even if weekly mileage remains stable. Triathletes must also take into account running on top of cycling training, keeping in mind that downhill running increases PF joint stress. Athletes must also structure training to allow sufficient time for tissue adaptation. For example, avoid scheduling a quad dominant (i.e. front squats and knee extensions) weights session close to a hilly bike ride with lots of efforts.
Bike fit related factors:
As detailed earlier, saddle height, cleat orientation/float and medial wedging are important consideration when managing PFP.
It is generally recommended to increase saddle height to reduce knee flexion angles which increase quad work and PF compressive forces. Similarly, a reach that is too long may pull the rider forward, forcing them to take more weight through their quads rather than the saddle supporting their bodyweight.
In an ideal world, precise cleat alignment that accommodates natural tibial rotation and foot projection angle would address excessive rotational forces at the knee. Unfortunately, not everyone has access to getting such a precise fit, nor does every cyclist ride with legs as straight as pistons. Floating cleats can attenuate rotational forces at the knee joint without compromising on power.
The use of either cleat or insole wedging can address excessive medial knee motion by aligning the hips, knees and ankles into a better position. Most cyclists present with a forefoot varus, that is, having the foot tilt up on the inside (big toe tilted up). However, most cycling shoes and cleats are completely flat and do not account for this. As a result, the foot must pronate to meet the shoe, resulting in tibial internal rotation, knee valgus and hip adduction further up the kinetic chain. The simple addition of a medial wedge can block this pronation, optimising alignment of the lower limb (see image below). The same principle can be applied for cyclists with weak hip abductors /external rotators that collapse at the knee.
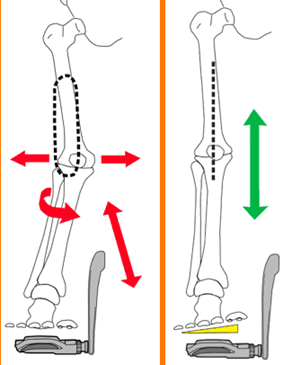
Image 3:The effect of medial wedging on lower limb alignment when cycling
Source: https://www.roadbikerider.com/do-you-really-need-shoe-wedges-or-is-your-q-factor-too-narrow/
Summary of management strategies:
Understanding the aforementioned factors will provide cyclists a good idea on how to manage PFP. In summary:
- First line management involves scaling back on provocative training loads. In less irritable cases, cyclists should try to maintain volume and cut back on intensity (i.e. hills, overgearing or harder efforts). Scheduling in extra rest days or substituting rides for gym work focused on non-provocative quad and glute strengthening is a sensible approach.
- There are strong evidence based recommendations for quadricep, hip abductor and external rotator strengthening for pain and functional improvements
- Cueing to avoid medial knee collapse may provide symptomatic relief.
- Saddle position, cleat orientation, vertical offset and the use of wedging can alter kinematics at the knee joint that contribute to PFP.
ITB Syndrome
Background
ITB syndrome is a common cause of lateral knee pain in cyclists and runners alike, and account for up to 15% of overuse knee injuries in cyclists (42). Previously coined ITB friction syndrome, it is now understood to caused by compression of the highly innervated fatty tissue between the ITB and femur. It has been shown that maximal compression occurs at approximately 30degrees of knee flexion (43) – correlating with classical ITBS pain symptoms. Cadaveric studies (B&K) have confirmed that the ITB does not ‘flick’ over the lateral femoral condyle (44) as previously believed, putting the friction theory to rest. This thick band of fascia crosses both the hip and knee joints, providing lateral support into hip adduction. Although the band cannot be stretched, adjacent muscles such as the vastus lateralis, biceps femoris and TFL can tension the band via fascial attachments. Excessive hip adduction and internal rotation may also increase ITB tensioning therefore compression of the fat pad distally.
Presentation:
Cyclists will present with sharp lateral knee pain that manifests at a predictable time or distance into a ride. It is often described as an ‘intense stabbing pain’, worse with the knee in slight flexion (approximately 20-30degrees), and will often force cyclists to stop training. There will be tenderness on palpation or compression over the lateral femoral condyle (about a finger’s width above the lateral knee joint line). In irritable cases, cyclists will experience symptoms bending and straightening the knee, walking downhill or descending stairs.
Contributing factors:
- Strength deficits of the hip abductors and external rotators are known risk factors for the development of ITB syndrome (45). Weakness of these muscles may result in excessive hip adduction and internal rotation, tensioning the ITB.
- A saddle that is too high is also linked with ITB syndrome. Repetitive knee flexion and extension through the provocative compressive zone (20-30deg knee flexion) is likely to further irritate the underlying fatty tissue.
- Cleat orientation that forces a toe-in, heel-out foot position (18) will result in greater internal rotation of the tibia- which is known to increase compression on the lateral aspect of the knee.
- Sudden increases in cycling duration or mileage is an important risk factor that has been discussed at length in the first blog of this series. Triathletes should also consider concurrent running volumes. Downhill or cambered running in particular can irritate symptoms. Carrying existing muscle fatigue from running into riding can also bring about symptoms earlier into rides.
- Non-modifiable anatomical risk factors that can increase ITB tension include; significant leg length discrepancies, narrow pelvic width, prominent femoral epicondyles, varus knee alignment (45) and sub-talar pronation (18).
Management:
1. Load management:
It is important for cyclists to reduce training volumes to allow the irritated fat pad to settle.
In mild cases, cyclists may be able to continue riding at lower intensities but should stop well before the predictable onset of pain. Triathletes should consider reducing running volumes and avoid running on cambers or downhill until symptoms settle. During the acute stage, cyclists should engage in cross training activities such as swimming and address causative strength deficits. Icing the area may provide a temporary reduction in pain after flare ups, however, does not address the root cause of the problem.
2. Bike set up:
It is recommended that cyclists with lateral knee pain reduce saddle height to ensure the knee does not extend past the provocative ‘compressive range’ of 30degrees knee flexion. Therefore it is recommended that maximal knee extension is set at approximately 40degrees knee flexion (18).
Cleats should be positioned so that the feet are aligned in their natural position. Foot projection angles in these cyclists should typically range from straight or slightly turned outwards.
The addition of a medial wedge under the cleat or inside the cycle shoe can minimise hip adduction by blocking sub-talar pronation at the ankle joint (as outlined in the PFP section of the blog series).
Lastly, Q factor (horizontal distance between the pedals) should be adjusted so that hips, knees and ankles are in neutral alignment. Cyclists with wider hips on a bike with a small Q factor may find narrow foot spacing increases stress on the lateral knee.
3. Strengthening:
People with ITBS commonly present with hip abductor and external rotator weakness. Although there is debate to whether greater tensioning of the ITB causes compensatory weakness of these muscles, evidence supports progressive resistance training programs that target these muscles (46). Cyclists should also continue strengthening the entire kinetic chain throughout rehab, increasing quadricep, calf and hamstring capacity. Examples of exercise that can be utilised during each stage of rehab are listed below:
Early stage:
- Side plank top leg abduction
- Crab walk
- Standing fire-hydrants
- Cable hip abduction
Mid stage:
- Lateral step up (small step)
- Box step up
- Star excursion balance
- Single leg hip thrust
Late stage:
- Curtsy step up
- Curtsy lunge
- Rearfoot elevated squat
A quick note on foam rolling, massage and stretching:
Foam rolling and stretching the ITB has been popularised as treatment for ITBS. Remember, the ITB is not a contractile structure and cannot be stretched or deformed. Therefore, massage and rolling will not directly change ITB length or ‘break down’ knots. Trying to stretch or roll out the ITB will only cause greater tensioning of the fascia and compression of the fatty tissue beneath.
Training through cycling injuries- a general guide
Cyclists should avoid total rest when injured and aim to maintain some level of training. This will facilitate a quicker return to pre-injury training levels and reduce the impact of detraining on performance.
The key is finding a workload that:
1. Does not flare up pain greater than a ‘mild’ level (approx 3/10 on a pain scale of 1-10) during or after training
2. Allows discomfort to settle quickly after training and returns to baseline levels within 24hours.
3. Does not cause a long-term trend of increasing pain (i.e. over weeks)
This can be achieved by reducing the duration of workouts, rides per week, intensity of sessions, amount of hill climbing or overgearing efforts and substituting cycling sessions for other forms of cross training.
In rare cases where cyclists are completely forced off the bike (examples being traumatic fracture or a highly irritable proximal hamstring tendon), they should aim to maintain cardiovascular fitness through non-provocative activities. Modalities such as swimming, pool running or elliptical machines can be structured similar to the cyclist’s typical training sessions to maintain fitness. For example, bike interval sessions can be easily replicated in the pool or on the elliptical machine using the same intensities and work: rest ratios.
It is also a great time for cyclists to focus on strength and mobility deficits, which will lead to better performance (8-10) and enjoyment on the bike. Even if cyclists are unable to load through their lower limbs due to serious injury, working on core and upper body strengthening will enhance stability and assist in sustaining good positions during longer rides. As mentioned in part 1, this will also minimise unnecessary movements, optimising efficiency and comfort.
If you haven’t read part 1, here is a brief overview of the topics covered:
The first instalment of the blog took a deep delve into bike fit, tissue capacity and training error- the 3 critical factors that must be considered when dealing with overuse injuries. Here are some key takeaways from the preceding sections of the blog for context:
- Most overuse injuries can be managed or prevented by either; i) increasing tissue capacity, ii) training at appropriate loads, iii) suitable bike fit, or iv) a combination of these factors
- The most effective way to improve tissue capacity (ability to handle training load) is through a progressive heavy resistance training program combined with adequate recovery.
- Training load is the dosage or stimulus produced by a workout or ride. It is influenced by internal factors (such as life stressors, nutrition and general health) and external factors (such as environmental conditions).
- Consistent training at high loads has been shown to be protective against injury. Acute: Chronic Workload Ratio (ACWR) can help guide training loads to avoid a boom-bust cycle of injury.
- There is a window of optimal bike fit that finely balances the following 3 variables: i) aerodynamics, ii) power, iii) comfort
- Bike fit can change over time and must take into account the cyclist’s mobility, strength, previous injuries, anthropometry and specific cycling goals/requirements.
- Subtle adjustments to bike fit parameters can redistribute joint forces, muscular work and interface contact pressures- all of which can offload sensitive tissue and play a key role in injury prevention and management.

Julian Tubman (APAM)
Physiotherapist
Featured in the Top 50 Physical Therapy Blog
References:
- Rooney, D., Sarriegui, I., Heron, N. (2020) ‘As easy as riding a bike’: a systematic review of injuries and illness in road cycling. BMJ Open Sport and Exercise Medicine. E000840. Doi:10.1136/bmjsem-2020-000840
- Clarsen, B., Krosshaug, T., Bahr, R. (2010) Overuse injuries in professional road cyclists. American Journal of Sports Medicine. Vol 38 pages 2494-2501
- Clarsen, B., Visentini, P. (2016) Overuse injuries in cycling. Aspetar Sports Medicine Journal. Pages 486-492
- Dahlquist, M., Leisz, M.C., Finkelstein, M. (2015) The club level road cyclist: injury, pain and performance. Clinical Journal of Sports Medicine Vol 25 pages 88-94
- Wilber, C.A., Holland, G.J., Madison, R.E., Loy, S.F. (1995) An epidemiological analysis of overuse injuries among recreational cyclists. International journal of Sports Medicine. Vol 16, Pages 201-206.
- De Bernado, M., Barrios, C., Vera, P., Laiz, C., Hadala, M. (2012) Incidence and risk for traumatic and overuse injuries in top level road cyclists. Journal of Sports Science. Vol 30: pages 1047-1053
- Palastanga, N., Field, D., Soames, R. (1989) Anatomy and human movement: structure and function. Oxford. Heinemann Medical Books
- Ericson, M.O., Nisell, R. (1987) Patellofemoral forces during ergometric cycling. Physical Therapy. 67(9) pages 1365-9
- Tamborindeguy, A.C, Bini, R. (2011) Does saddle height affect patellofemoral and tibiofemoral forces during bicycling for rehabilitation. J Bodyw Mov Ther. 15(2): pages 186-91
- Bini, R.R, Hume, P.A. (2014) Effects of saddle height on knee forces of recreational cyclists with and without knee pain. Int SportMed J. 15(2) pages 188-99
- Brukner, P., Khan, K., with Burt, P and Clarsen, B. (2012). Brukner and Khan’s Clinical Sports Medicine, from Biomechanical aspects of injury in specific sports. Sydney. McGraw Hill.
- Bailey, M.P., Maillardet, F.J., Messenger, N. (2003) Kinematics of cycling in relation to anterior knee pain and patellar tendinitis. Journal of Sports Science. 21(8) 649-57
- Hannaford, D.R., Moran, G.T., Hlavac, H.F. (1986) Video analysis and treatment of overuse knee injury in cycling: a limited clinical study Clin Podiatr Med Surg. 3(4): 671-8
- Wheeler, J.B., Gregor, R.J, Broker, J. (1995). The effect of clipless float design on shoe/pedal interface kinetics and overuse injuries during cycling. Journal of applied biomechanics. 11: pages 119-41
- Luyckx, T., Didden, K., Vandenneucker, H., Labey, L., Innocenti, B., Bellemans, J. (2009) Is there a biomechanical explanation for anterior knee pain in patients with patella alta?: influence of patellar height on patellofemoral contact force, contact area and contact pressure. J Bone Joint Surg Br. 91(3):344-50.
- Batailler, C., & Neyret, P. (2018). Trochlear dysplasia: imaging and treatment options. EFORT open reviews, 3(5), pages 240–247
- Herrington L. (2013) Does the change in Q angle magnitude in unilateral stance differ when comparing asymptomatic individuals to those with patellofemoral pain? Phys Ther Sport. 14(2):94-7.
- Witvrouw, E., Callaghan, M.J., Stefanik, J.J, et al (2014) Patellofemoral pain: consensus statement from the 3rd International Patellofemoral Pain Research Retreat held in Vancouver September 2013. British Journal of Sports Medicine. 48: 411-14
- Lack, S., Morrisey, D., Malliaris, P. (2012) Gluteal muscle activity and patellofemoral pain syndrome: A systematic review. British Journal of Sports Medicine DOI: 10.1136/bjsports-2012-090953
- Earl, J., Hoch, A.Z. (2011) A Proximal Strengthening Program Improves Pain, Function and Biomechanics in Women with Patellofemoral Pain Syndrome. American Journal of Sports Medicine. 39: 154
- Lankhorst, N.E, Bierma-Zeinstra, SMA, van Middelkoop, M. (2012) Risk Factors for patellofemoral pain syndrome: a systematic review. Journal of Orthopaedic Sports Physical Therapy 42(2): 81-A12
- Giles L.S., Webster, K.E., McClelland, J.A. et al. (2013) Does quadriceps atrophy exist in individuals with patellofemoral pain? A systematic literature review with meta-analysis. Journal Orthopaedic Sports Physical Therapy 43(11): 766-76
- Bini, R.R., Bini, A.F. (2018) Potential factors associated with knee pain in cyclists: a systematic review. Journal of Sports Medicine. 9: 99-106
- Smith, T., Bowyer, D., Dixon, J., Stephenson, R. (2009) Can vastus medialis oblique be preferentially activated? A systematic review of electromyographic studies. Physiotherapy Theory and Practice 25(2): 69-98
- Holmes JC, Pruitt AL, Whalen NJ. Iliotibial band syndrome in cyclists. Am Orthop Soc sports med. 1993;21:419 –424.
- Fairclough, J., Hayashi, K., Toumi, H., Lyons, K., Bydder, G., Phillips, N., Best, T. M. and Benjamin, M. (2006), The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome. Journal of Anatomy, 208: 309–316
- Fairclough, J., Hayashi, K., Toumi, H. et al. Is iliotibial band syndrome really a friction syndrome? J Sci Med Sport 2007;10(2):74–6.
- Friede, M., Innerhofer, G., Fink, C., Alegre, L., Csapo, R. (2022) Conservative treatment of iliotibial band syndrome in runners: Are we targetting the right goals? Phys Ther Sport. 27(54), 44-52
- Geisler, P,R. (2020) Iliotibial Band Pathology: Synthesizing the Available Evidence for Clinical Progress. J Athl Train. doi: 10.4085/JAT0548-19. Epub ahead of print. PMID: 33351908.
- Sunde, A., Storen, O., Bjerkaas, M., Larsen, M.H., Hoff, J, Helgerud, J. (2010) Maximal strength training improves cycling economy in competitive cyclists. Journal of Strength and Conditioning Research. Vol 24 (8), pages 2157-2165
- Ronnestad, B.R., Hansen, J., Hollan, I., Ellefsen, S. (2014) Strength training improves performance and pedalling characteristics in elite cyclists. Scandinavian Journal of Medicine & Science in Sports. 25: e89-e98
- Vikmoen, O., Rønnestad, B.R. (2021) A Comparison of the Effect of Strength Training on Cycling Performance between Men and Women. Journal of Functional Morphology and Kinesiology. 6(1):29.






