Groin and Pubic Pain – What is the source of symptoms? What is the source of the problem?

The hip and groin is a complex area, with a wide variety of possible injuries in numerous anatomical structures. Athletic pubic pain has been called by many names sometimes interchangeably. A correct diagnosis helps guide you through best management and can give an accurate prognosis for time to return to sport or whether normal training can continue. To make a complex area more complex, imaging such as MRI reveals a high prevalence of ‘abnormal findings’ in athletes without symptoms, increasing the complexity of determining diagnosis in this area (2, 3).
If we examine the anatomy of the pubic and groin region there are numerous musculoskeletal structures that can become a source of symptoms for an active individual. These include but are not limited to the pubic symphysis, pubic bone, rectus abdominus tendon and adductor longus tendon. Also potentially referring symptoms in this area include the lumbar spine and pelvic floor. Here we help you identify different types of pain in this region and what it means for your recovery.
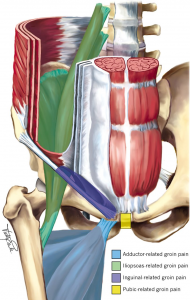
Common Sites Of Groin and Pubic Pain (1)
Sources Of Symptoms
Pubic Bone Stress Reaction/Stress Fracture
Bone related symptoms present with maximal tenderness localised to the bone on one or both sides. There can also be associated lower abdominal or upper adductor symptoms. Symptoms typically have a gradual and are worse with increasing levels of stress, such as running, kicking or kicking.
Pubic Bone Apophysitis
Apophysitis refers to inflammation of the growth plate. In active adolescents inflammation can occur at the pubic bone and can present very similar to a bone stress injury in a younger athlete. Distinguishing features from bone stress include increased pain on adductor stretch or pain or adductor contraction whilst in stretched position.
Rectus Abdominis Tendinopathy/Enthesopathy
Rectus abdominis tendinopathy or enthesopathy refers to symptoms arising from the tendon of the abdominals where it inserts onto the superior pubic bone. Pain is typically slightly above the pubic bone and can occur either after a sudden increase in abdominal loads or more gradually over time.
Adductor Tendinopathy/Enthesopathy
Adductor related pain refers to pain localised high on the adductor tendon or its location onto the pubic bone. Pain is reproduced on palpation and contraction of the adductors. Typically pain will warm up but is aggravated by higher level cutting, kicking, turning loads.
Pubic Symphysis Irritation
Pubic symphysis is the fibrocartilaginous disc localised between the two pubic bones. Symptoms can arise from this location and its margins more than the local bone, abdominals and or adductors.
Patterns Of Pain
As much as there can be different identified areas that are the source of symptoms as listed above, many can overlap and occur simultaneously. Adding to diagnostic difficulty is that many of these presentations can have widespread pain at the pubic bone, abdominals and adductors. Additionally aggravating factors are similar (running, cutting, twisting, sit ups, adductor contractions, kicking and coughing/sneezing) and many have a similar onset of symptoms.
Source of The Problem
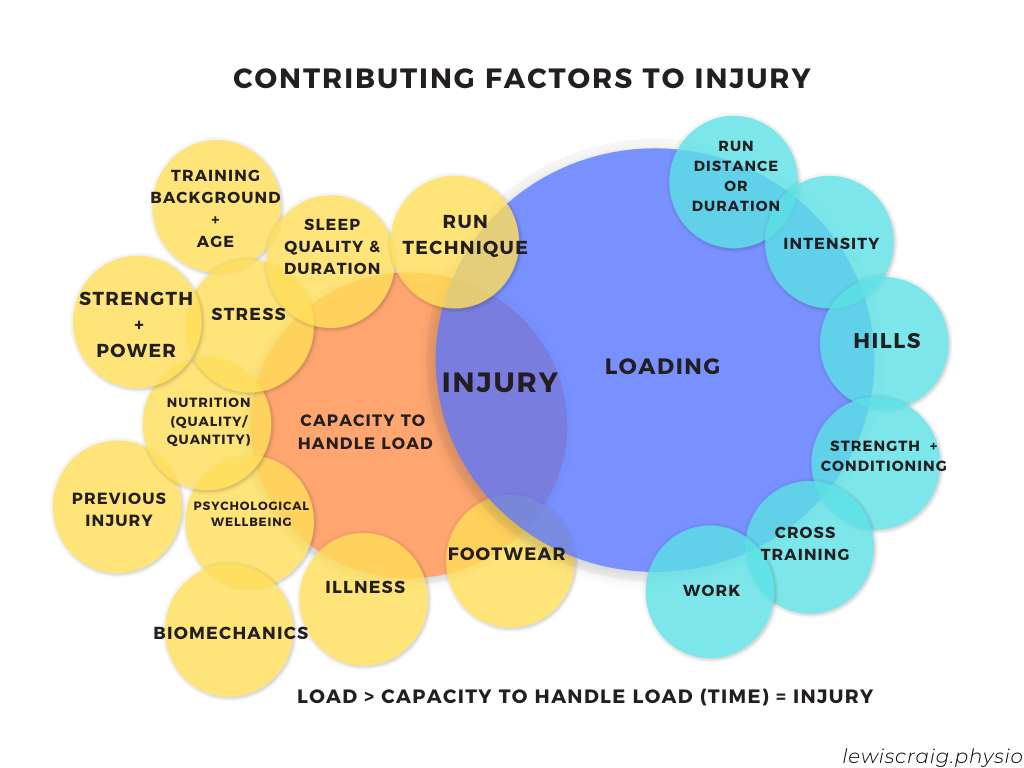
Although the source of symptoms may be specific to an entitiy described above, each can be caused by the same characteristics. Contributing factors are typically multifactorial and can include a sudden increase in load (running, change of directions, kicking, hills, gym work). Addressing the source of the problem requires looking at the range of variables that may have accounted for the injury (see figure 2). In particular identifying biomechanical patterns that may increase stress on the source of symptoms is important. These patterns such as increases in side or forward flexion of the trunk, greater hip abduction or internal rotation can be targeted in rehabilitation (Franklyn-Miller et al 2017). Addressing strength and range of motion deficits is also important in early rehabilitation before returning to higher level loading.

Lewis Craig (APAM)
POGO Physiotherapist
Masters of Physiotherapy
Featured in the Top 50 Physical Therapy Blog
References
- Weir, A., Brukner, P., Delahunt, E., Ekstrand, J., Griffin, D., Khan, K. M., … & Paajanen, H. (2015). Doha agreement meeting on terminology and definitions in groin pain in athletes. British journal of sports medicine, 49(12), 768-774.
- Branci, S., Thorborg, K., Nielsen, M. B., & Hölmich, P. (2013). Radiological findings in symphyseal and adductor-related groin pain in athletes: a critical review of the literature. British journal of sports medicine, 47(10), 611-619.
- Branci, S., Thorborg, K., Bech, B. H., Boesen, M., Nielsen, M. B., & Hölmich, P. (2014). MRI findings in soccer players with long-standing adductor-related groin pain and asymptomatic controls. British journal of sports medicine, bjsports-2014.
- Franklyn-Miller, A., Richter, C., King, E., Gore, S., Moran, K., Strike, S., & Falvey, E. C. (2017). Athletic groin pain (part 2): a prospective cohort study on the biomechanical evaluation of change of direction identifies three clusters of movement patterns. British journal of sports medicine, 51(5), 460–468. https://doi.org/10.1136/bjsports-2016-096050