


Invisible Pain Series: Mast Cell Activation Syndrome
Invisible Illnesses are physical, mental or neurological conditions that are not commonly visible from the outside to others. These conditions and the symptoms involved can limit or challenge a person’s movements, activities and daily functioning in various ways. Many forms of chronic/persistent complex pain are linked with a range of what we would call ‘Invisible Illnesses’ – conditions like Fibromyalgia, Mast Cell Activation Syndrome, Myalgic Encephalitis, Long COVID, Endometriosis, Auto-immune Disorders, Ehlers Danlos Syndromes and other Hypermobility-related syndromes, plus many more.
These conditions can bring about severe and debilitating pain for the person experiencing it, often without clear and objective ‘measurable’ signs that medical and health professionals can make sense of clearly. Leading to them falling into the ‘too hard basket’ for many health professionals. Which of course leaves the person living with one of these conditions feeling confused, overwhelmed and unable to live the life they want.
In this series of blogs I will be covering the various conditions/diagnoses that can lead to experiencing complex ‘invisible pain’. We will briefly review the best available scientific evidence for each condition, the current options available for treatment and how Physiotherapy can help get you back to the life you want to live.
Mast Cell Activation Syndrome
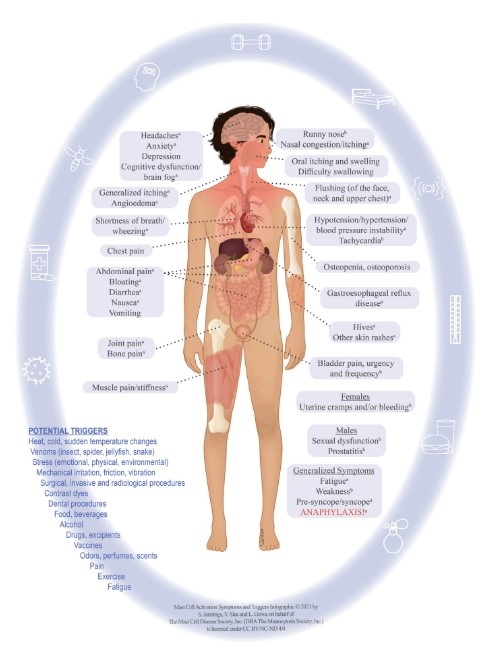
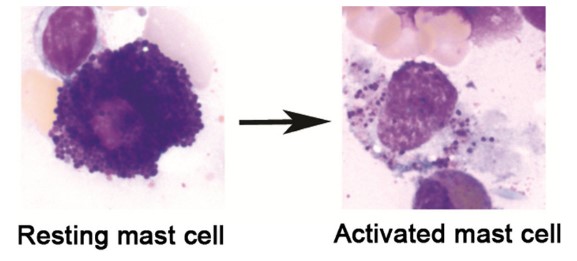
Mast cell activation syndrome (MCAS) is a condition that occurs when mast cells, a type of immune cell, release an excessive amount of histamine and other inflammatory substances into the body. This can lead to a range of symptoms, including those listed below:
- Widespread Fibromyalgia-type pain
- Joint hypermobility
- Headache
- Sensory neuropathy
- Dysautonomias (e.g. orthostatic hypotension, blood pressure and heart rate lability, thermal dysregulation)
- Allergic-type issues
- Fatigue
- Cognitive dysfunction
- Irritated eyes/nose/ mouth/throat
- Shortness of breath
- Heart palpitations
- Nausea
- Reflux
- Abdominal pain
- Diarrhoea (often alternating with constipation)
- Interstitial cystitis (chronic bladder pain)
- Menorrhagia & Dysmenorrhea (abnormal menstruation)
- Anxiety, mood disorders & much more
What is a Mast Cell?
Mast cells are ‘born’ in bone and sometimes fat tissue in the body. Upon leaving their birthplace they briefly circulate around the body and find their home (very sparsely) in all tissues. Especially tissues at environmental interfaces (e.g. nose, gastrointestinal tract, etc) and lymphovascular tissue, optimally positioned to serve as defenders against adverse environmental change.
Mast cells regulate host defence by acting as innate immune cells, interacting with the specific immune system, inducing/regulating inflammation, and recruiting other immune cells. They orchestrate microbial, toxic, and physical environmental defence through different biological mechanics (classic non-selective degranulation, selective mediator release). They also aid wound healing, tissue remodelling, and degrading certain endogenous toxins (e.g. endothelin-1 or neurotensin) in bacterial infection.
Prevalence & Diagnosis
Prior to the introduction of the term “Mast cell activation disease” (MCAD), “Mast cell disease” was the name given to refer to the full spectrum of diseases of mast cells, which included assorted forms of the rare disease of mastocytosis and various allergic diseases ranging from rare (e.g. certain urticarias) to common (e.g. environmental and food allergies). Until recently, the only Mast cell disease recognised by most health professionals was the range of overtly allergic-type phenomena and rarer mastocytosis.
Diagnosing MCAS is extremely challenging. This is due to the large number of places mast cells call home across the body, along with their enormous range in normal biological activities. Not to mention the wide range of ways they work/mediators they express. Think of them like a normal cell that when excessively activated, goes rogue like a criminal that can change faces and leave different kinds of problems depending on the face they wear, and where they find themselves in the city. Put simply MCAD (especially MCAS) is reasonable to suspect in any poorly explained chronic multisystem array of concurrent health conditions (especially if inflammatory in nature).
Symptoms can be persistent or episodic, coming and going in varied ways from person to person. Opposite effects can often appear in different patients at different times (e.g. alternating diarrhoea and constipation as in irritable bowel syndrome (IBS), which is increasingly linked to MCAS (2).
Underdiagnosis of Mast cell diseases, and MCAS has been prevalent, largely due to inappropriately diagnostic restrictive criteria. Despite increasing evidence of substantial prevalence of MCAS, with various publications providing estimates ranging from “rare” to as high as 17% of the general population (1). It is thought the latter estimate of 17% may be more likely due to the increasingly recognized high prevalence of a wide range of allergic and inflammatory disorders which may be rooted at least partly in MCAS.
With the widespread activity and placement of mast cells throughout the body, and limited research into MCAS diagnostic testing, diagnosis of MCAS remains a bit of a grey area. Not only that, MCAS is thought to be related, and potentially a large causative factor behind many other complex chronic pain conditions such as myalgic encephalitis/chronic fatigue syndrome (ME/CFS), fibromyalgia, irritable bowel syndrome (IBS), postural orthostatic tachycardia syndrome (POTS), small fiber neuropathy (SFN), hypermobile Ehlers Danlos Syndrome (hEDS), and Long COVID.
The “consensus-2” proposal states that levels of a slightly wider range of mediators relatively specific to the mast cells which rise above their normal ranges can be taken as diagnostic laboratory evidence of MCAS in the proper clinical context of other- wise unexplained chronic multisystem issues of generally inflammatory ± allergic ± dystrophic themes.:
- Tryptase
- Chromogranin A (CgA)
- Heparin
- PGD2
- Histamine
- N-MH
- 11-β-PGF2α
- Leukotriene E4 (LTE4)],
Some published research now suggests an elevated plasma heparin level likely is the single most sensitive marker of MCA, with approximately 80% of patients clinically demonstrating symptoms consistent with MCA showing increased levels of plasma heparin when measured using a sufficiently sensitive assay (1).
Treatment
While there is currently no cure for MCAS, there are several treatment options available, including physiotherapy as an adjunct. As the primary feature of MCAS is inappropriate or excessive mast cell activation, treatment always involves the identification and avoidance of mast cell activating triggers, along with control of mast cell mediator production/action. It has been commented by experts in this area that “treatment of MCAD should be focused on the individual patient, and tailored to the patient’s symptoms, disease manifestations, and the clinical course” (4). The same experts comment that moderate improvement is attainable, although both patients and providers must exercise patience, as an individual trial and error approach is required.
The predominant set of treatments available for MCAS are nutritional and pharmaceutical in nature, and thus beyond the scope of knowledge of the Physiotherapist writing this article. To comment briefly, there have been no therapeutic trials in MCAS yet. Most information about therapeutic effectiveness in MCAD has been found in small case series and single case reports, likely due to the mutational heterogeneity of the disease and thus the heterogeneity of its patterns of clinical presentation and therapeutic responsiveness. Common rules/approaches to treatment are listed below:
- Highly personalised regimens of pharmaceutical drugs are reported to be best
- Temporary abstinence from gluten, yeast, and dairy milk protein-containing foods during the initial month of drug therapy can improve response rate, possibly more from reducing trigger exposure than truly improving medication efficacy.
- NSAIDs (e.g. Ibuprofen) helps some MCAD patients but trigger others
- Aspirin desensitisation may be useful.
- Acute and chronic immunosuppressants can be considered
- Low dose Tyrosine kinase inhibitors (TKIs)
To read more see – Pharmacological treatment options for mast cell activation disease.
While it may seem surprising, or odd that Physiotherapy can help with a condition like MCAS, it is important to consider that adjunctive approaches to central medical management of the condition help maintain participation in valued activities in daily life. Integrative Physiotherapy can achieve this by working with each individual under the guidance of a MCAS aware Medical Practitioner to understand key triggers, functional limitations and goals of the individual.
Aside from the management and adjunctive treatment of pain, Physiotherapy focuses on the comprehensive development of psycho-physical capacity (strength, aerobic fitness, flexibility and nervous system adaptability). This capacity can then (in theory) lead to the more easeful management of symptoms in MCAS, and improvement in participation in valued activities (daily tasks, work, exercise, sport etc). An example of what Integrative Physiotherapy for MCAS can involve is outlined below:
- Comprehensive initial assessment, considering individuals medical and symptom history, goals and current presenting concerns/symptoms
- Massage and manual therapy to manage musculoskeletal pain/symptoms arising from MCAS
- The development of an individualised movement/exercise plan to suit the individual’s wants, needs and goals
- Exploration of nervous system regulation tools like breathing and mindfulness exercises to build tolerance and down-regulation skills for stress management. As psychological stress has been shown to increase mast cell activity
It’s important to note that while physiotherapy can be helpful for managing the symptoms of MCAS, it is not a cure. It should be used as part of a comprehensive treatment plan directed by a MCAS aware Medical Professional that also includes medication and lifestyle modifications.
If you’re struggling with MCAS or another invisible illness and need help, reach out and book an initial consultation with our Pain specialised Physiotherapist Oliver Crossley.

Oliver Crossley (APAM) POGO Physiotherapist
Book an appointment with Oliver here Featured in the Top 50 Physical Therapy Blog
References
- Afrin, L. B., Ackerley, M. B., Bluestein, L. S., Brewer, J. H., Brook, J. B., Buchanan, A. D., … & Molderings, G. J. (2021). Diagnosis of mast cell activation syndrome: a global “consensus-2”. Diagnosis, 8(2), 137-152.
- Afrin, L. B., Butterfield, J. H., Raithel, M., & Molderings, G. J. (2016). Often seen, rarely recognized: mast cell activation disease–a guide to diagnosis and therapeutic options. Annals of medicine, 48(3), 190-201
- Molderings, G. J., Haenisch, B., Brettner, S., Homann, J., Menzen, M., Dumoulin, F. L., … & Afrin, L. B. (2016). Pharmacological treatment options for mast cell activation disease. Naunyn-Schmiedeberg’s Archives of Pharmacology, 389(7), 671-694
- Wirz, S., & Molderings, G. J. (2017). A practical guide for treatment of pain in patients with systemic mast cell activation disease. Pain Physician, 20(6), E849
- Alysandratos, K. D., Asadi, S., Angelidou, A., Zhang, B., Sismanopoulos, N., Yang, H., … & Theoharides, T. C. (2012). Neurotensin and CRH interactions augment human mast cell activation. PLoS One, 7(11), e48934.
- Kurin, M., Elangovan, A., Alikhan, M. M., Al Dulaijan, B., Silver, E., Kaelber, D. C., & Cooper, G. (2022). Irritable bowel syndrome is strongly associated with the primary and idiopathic mast cell disorders. Neurogastroenterology & Motility, 34(5), e14265
- Bonamichi-Santos, R., Yoshimi-Kanamori, K., Giavina-Bianchi, P., & Aun, M. V. (2018). Association of postural tachycardia syndrome and Ehlers-Danlos syndrome with mast cell activation disorders. Immunology and Allergy Clinics, 38(3), 497-504
- Afrin, L. B. (2021, December). Some cases of hypermobile Ehlers–Danlos syndrome may be rooted in mast cell activation syndrome. In American Journal of Medical Genetics Part C: Seminars in Medical Genetics (Vol. 187, No. 4, pp. 466-472). Hoboken, USA: John Wiley & Sons, Inc
- Theoharides, T. C., Tsilioni, I., & Bawazeer, M. (2019). Mast cells, neuroinflammation and pain in fibromyalgia syndrome. Frontiers in Cellular Neuroscience, 13, 353
- Afrin, L. B., Weinstock, L. B., & Molderings, G. J. (2020). Covid-19 hyperinflammation and post-Covid-19 illness may be rooted in mast cell activation syndrome. International journal of infectious diseases, 100, 327-332
- Jennings, S. V., Slee, V. M., Finnerty, C. C., Hempstead, J. B., & Bowman, A. S. (2021). Symptoms of mast cell activation: the patient perspective. Annals of Allergy, Asthma & Immunology, 127(4), 407-409





