


ACL Surgery: Cyclops Lesions

When I mention the word “cyclops” it might conjure visions of a giant one-eyed beast from your nightmares but this type of cyclops is more of a physiotherapist’s nightmare. Sometimes when patients undergo reconstruction surgery of their Anterior Cruciate Ligament (ACL) they have issues with achieving full extension (straightening) of the knee. This may be due to a what is termed a “Cyclops Lesion”.
So what is a Cyclops Lesion?
The pathology was first described in 1990 by Jackson & Schaefer in patients post-ACL reconstruction surgery and it is now a well-recognised phenomena. The lesion is a focal anterior arthrofibrosis which consists of fibrous tissues and may or may not include cartilage and bony components (5). It occurs at the anterior portion of the graft and protrudes from between the femur and tibia at the intercondylar notch (2). In simple terms, it is a lump of scar tissue at the front of the knee and it blocks it from completely straightening.
A arthroscopic video of the cyclops lesion showing how it impinges in between the tibia and femur.
How does it present?
The hallmark sign of a cyclops lesion is loss of knee extension range often about 2-3 months following an ACL surgery. However it can be an issue for years post-op. It is not a huge loss of extension, often less than 10°, but it’s enough to be a problem (8). Pain at the front of the knee usually coincides with this reduced movement and there may even be an audible clunk. Usually the patient will also have some quadriceps dysfunction.
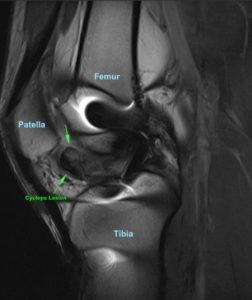
A MRI looking from the side shows the cyclops lesion (dark patch) protruding anteriorly.
Why does it happen?
There a couple of competing theories on why the scar tissue develops. Jackson & Schaefer suggested that problem was caused by either the debris left in the knee joint from drilling the tibial tunnel or from loose ACL graft fibres. They proposed that this debris caused formation of the granulation tissue. This has since been debated however the two surgeons were actually able to reduce their incidence of cyclops lesions by leaving less debris in the joint post-surgery (7). It’s also been suggested that the cyclops lesion was caused from graft impingement when the knee was in full extension which leads to scar tissue formation (4). Whatever the cause, the evidence currently suggests it’s not the fault of the patient or the physio. The development of cyclops lesions is a multi-factorial process and hard to predict (3).
Cyclops Lesion without surgery?
Although much less recognised, it is possible for patients who have suffered ACL trauma to develop a cyclops lesion even without having had surgery. The mechanisms are thought to be similar to the post-surgery presentation (7). This means that it should be suspected in any patient who has a loss of extension following any form of ACL injury.
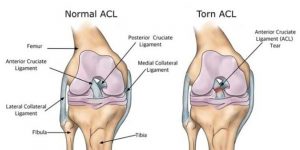
Anatomical location of the ACL and what a torn ACL looks like (right).
What can you do about it?
Unfortunately, physiotherapy isn’t able to help your cyclops lesion. No matter how hard you and your physio try to get the knee straight, it won’t go. A second arthroscopy is then needed to remove the nodule of scar tissue in order to regain extension (2).
If a cyclops lesion is suspected, you will need to return to your orthopaedic surgeon and likely have an MRI to confirm the presence of the scar tissue. MRI has been shown to be 84% accurate in detecting cyclops lesions (2) and surgical intervention is generally successful in restoring knee function (8).
Extension Matters!
In any ACL surgery it is really important to work hard on regaining extension early. Loss of extension is one of the most common complications following ACL surgery and can be of detriment to functional ability, especially in the athletic population (6). A small amount of hyperextension of the knee is important, the knee should actually go about 5-6° past completely straight. This is part of the “screw-home” mechanism or that “locked out” feeling you get when you straighten your knee. It’s an important aspect of creating a stable knee and a lack of extension puts added stress on the quadriceps muscles and patellofemoral joint (under the knee cap) (1).
3 Key Knee Extension Exercises
1. Supine Prolonged Low-Load Stretch
In laying or sitting, have your foot elevated. Apply a low load on top of the knee and hold this for a prolonged period e.g 15 minutes. It may be more comfortable to have the weight applied either side of the knee joint if the knee itself is sore. This stretch can be performed in a variety of ways depending on what equipment is available (see below).



2. Calf & Hamstring Stretch with Pressure
In a long-sit position place a towel or band around your foot. Keep your leg straight and pull on the towel stretching the calf. Simultaneously apply pressure down on the knee.

3. Standing Banded Knee Extension
In standing, anchor a resistance band to something and place it around your knee. Walk forward to increase the force pulling your knee into extension. Lock & unlock your knee, not letting it “flick” or “flop” back to straight.
The great part about this exercise is that it can be performed in a more functional, weight-bearing position. Also, moving your knee in & out of terminal extension helps develops hamstring and quadriceps control which can be lacking post-injury.
Summary
- The cyclops lesion is a nodule of scar tissue that has grown in the front of the knee joint
- The cause of cyclops lesions is likely multi-factorial but may be linked to debris in the joint
- The hallmark sign of a cyclops lesion is loss of extension post-surgery
- Patients usually also have anterior knee pain and quadriceps dysfunction
- Physiotherapy is ineffective once the lesion exists and arthroscopic surgery is needed which is often very successful
- It’s extremely important to work on regaining knee extension following any ACL surgery

James Gardiner
POGO Physiotherapist
Book an Appointment with James here.
Featured in the Top 50 Physical Therapy Blog
References
- Millett, P. J., Wickiewicz, T. L., & Warren, R. F. (2001). Motion Loss after Ligament Injuries to the Knee. The American Journal of Sports Medicine, 29(5), 664–675. doi:10.1177/03635465010290052401
- Bradley, D. M., Bergman, A. G., & Dillingham, M. F. (2000). MR Imaging of Cyclops Lesions. American Journal of Roentgenology, 174(3), 719-726. doi:10.2214/ajr.174.3.1740719
- Delince, P., Descamps, P. Y., Fabeck, L., & Hardy, D. (1998). Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 14(8), 869-876. doi:10.1016/s0749-8063(98)70025-8
- Marzo, J. M., Bowen, M. K., Warren, R. F., Wickiewicz, T. L., & Altchek, D. W. (1992). Intraarticular fibrous nodule as a cause of loss of extension following anterior cruciate ligament reconstruction. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 8(1), 10-18. doi:10.1016/0749-8063(92)90129-y
- Minne, C., Velleman, & Sulleman, F. E. (2012). MRI findings of cyclops lesions of the knee. SA Orthopaedic Journal, 11(2). Retrieved from http://www.scielo.org.za/scielo.php?script=sci_arttext&pid=S1681-150X2012000200011
- Petsche, T. S., & Hutchinson, M. R. (n.d.). Loss of Extension After Reconstruction of the Anterior Cruciate Ligament. Journal of the American Academy of Orthopaedic Surgeon, 7(2), 119-127.
- Runyan, B. R., Bancroft, L. W., Peterson, J. J., Kransdorf, M. J., Berquist, T. H., & Ortiguera, C. J. (2007). Cyclops Lesions That Occur in the Absence of Prior Anterior Ligament Reconstruction1. RadioGraphics, 27(6), e26-e26. doi:10.1148/rg.e26
- Sonnery-Cottet, B., Lavoie, F., Ogassawara, R., Kasmaoui, H., Scussiato, R. G., Kidder, J. F., & Chambat, P. (2010). Clinical and Operative Characteristics of Cyclops Syndrome After Double-Bundle Anterior Cruciate Ligament Reconstruction. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 26(11), 1483-1488. doi:10.1016/j.arthro.2010.02.034






