


The Myth of Core Stability and Low Back Pain

Low back pain is now the number one cause of disability globally and will be experienced by most people at some point in their lives (84% lifetime prevalence) (1,2). However, it is best understood as a symptom, and not a disease in and of itself (1,2). The prevalence and complexity of low back pain has led to much argument over the best way to manage it, this is particularly seen in the contrast between statements in the image below from the late Dr Alf Nachemson, a pioneering researcher and clinician in LBP, and Professor Stuart McGill, a famous spine biomechanics researcher.
Much of this contrast seen above can be put down to the distinctions between the old biomedical model and the modern, more holistic biopsychosocial model. The older biomedical model was purely focused on objective physical signs of pathology and presumed the source/origin of diseases and illness lie in these physical signs. Which then meant all modes of treating such diseases and illnesses focused solely on pathological structures themselves (e.g. protruding lumbar discs, joint osteoarthritis etc).
Whereas the newer Biopsychosocial approach, pioneered by George Engel over 30 years ago, frames illness and disease from a broader perspective, integrating biological factors (e.g. joints, muscles and tissues), with psychological (e.g. stress and anxiety) and social (low socio-economic status, close personal relationships) factors to understate and treat such issues from a more holistic view (6,8).
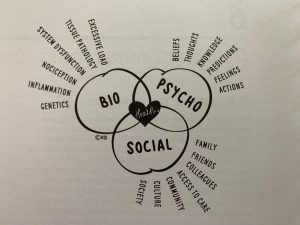
Image Source: Explain Pain Supercharged (6)
One biomedical panacea in particular still persists as a cure all for most back pain of all kinds and durations … ‘Core Stability’. However, we will find that it is not the cure all we think it is, and back pain is better understood from a more holistic perspective introduced above.
The notion of core stability for LBP notably arose out of the global rehab and fitness world’s reaction to brilliant research from Paul Hodges, a Physiotherapy professor at University of Queensland, who was then in 1998 completing his PhD. Paul looked at a group of people with recurrent low back pain matched with a control group and assessed their abdominal muscle activation (notably the transversus abdominus and obliquus internus abdominis muscles) during and immediately after a range of different velocity arm movements (3). What he found was that those with recurrent LBP failed to recruit their deeper abdominal muscles with fast and intermediate speed arm movements – for more read here (3).
This finding of altered preparatory spinal control in a few subjects initiated a wave of hypotheses and subsequent research into the relationship between abdominal muscle control (especially the poor old transversus abdominus (TA) – AKA our deepest and internal muscular waist belt) and low back pain. The central assumption of this hypothesis is that the TA produces a preparatory stability of the lumbar vertebrae by inducing an increase in intra-abdominal pressure (what happens when you cough or brace) that reduces local shear and compressive forces on the spine – which have been shown to increase risk of disc prolapse (4). Fast forward twenty years to the present day and see that the poor old TA muscle has become the focus and culprit for most types of LBP. However, we will see that this focus and blaming of a singular muscle is not well backed by research evidence.
The TA is commonly categorised into the ‘local’ subgroup of trunk or ‘core’ muscles which are supposed to control single vertebral segments and are responsible for their stabilisation (4). The larger subgroup of ‘global’ trunk muscles are not directly connected to the spine but support and affect spinal orientation without direct segmental influence (4). When a person then presents to the clinic complaining of back pain – the common approach has been to prescribe isolated trunk muscle strengthening and control exercises that address the so called ‘local’ subgroup of muscles, such as the transverse abdominus, multifidus and obliquus internus abdominus (4). When held up to objective investigation, we actually see trunk muscles work as a functional unit, with muscle activations shifting depending on the specific movement task (4). The notion that muscles in the trunk can be specifically split up into groups and trained separately is a reductionist and false notion (4).
In a critical review of the literature on ‘core stability’, Wirth et al. states that there is no supporting evidence for the basic assumption that those with low back pain have activation deficits or atrophy of core muscles like the TA or multifidus (4). They also comment that an activation deficit or muscle atrophy is more likely to be the result of pain rather than the cause (4).
Whilst the available science supports exercise as a beneficial treatment for LBP, the reality is (as always far more complex) more dynamic and interactive than our simple models can often explain (7). Hence, we return to the previously mentioned Biopsychosocial model to better explain what we currently understand about back pain and how to best rehabilitate it. As we have seen, back pain is not well understood by solely framing it within a biomedical framework (1). Many people have been shown to display pathological and degenerative signs on imaging (e.g. disc prolapse and joint degeneration on X-rays and MRI) without any reported pain (REF). Evidence clearly states that most low back pain is non-specific, meaning that it is not possible to identify a single origin (there are often many) of a patient’s symptoms (7).
Therefore, the notion that back pain is best treated by specific core muscle training that supports and reduces further risk of damage these ‘pathological areas’ becomes laughable and at best inadequate (1,4).
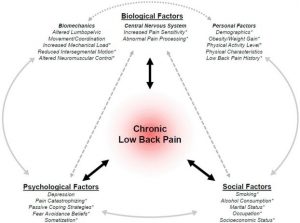
Image Source: (5)
The Biopsychosocial model more appropriately explains how multiple factors in a person’s life can influence their illness experience. This is best visualised in the image above.As mentioned in my previous blogs – Pain is best understood as a protective mechanism of the nervous system related to a balance of danger and safety messages we receive (6). Structural damage is only one of those, and as mentioned above, it is not always a reliable indicator of why someone is feeling pain. With of all of this in mind, the main question remains:
‘What then do we do when experiencing low back pain (acute and chronic)?’
Most of us know we need to keep moving, and the evidence suggests this. The two best treatment strategies we have for low back pain from the available science are:
Physical Activity:
Personal valued forms of exercise are best (e.g. if you like swimming > gym) to help build physical capacity and thus build a protective buffer against physical stressors that often contribute to the onset of pain
Education:
Gaining a broader understanding from a biopsychosocial perspective that de-threatens your experience of pain and promotes an active approach to rehabilitation
(1)

Oliver Crossley (APAM)
POGO Physiotherapist
Book an appointment with Oliver here
Featured in the Top 50 Physical Therapy Blog
References:
- Foster, Nadine E., Johannes R. Anema, Dan Cherkin, Roger Chou, Steven P. Cohen, Douglas P. Gross, Paulo H. Ferreira et al. “Prevention and treatment of low back pain: evidence, challenges, and promising directions.” The Lancet 391, no. 10137 (2018): 2368-2383
- Airaksinen, Olavi, Jens I. Brox, Christine Cedraschi, Jan Hildebrandt, Jennifer Klaber-Moffett, Francisco Kovacs, Anne F. Mannion et al. “European guidelines for the management of chronic nonspecific low back pain.” European spine journal15, no. Suppl 2 (2006): s192
- Hodges, Paul W., and Carolyn A. Richardson. “Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds.” Archives of physical medicine and rehabilitation80, no. 9 (1999): 1005-1012.
- Wirth, Klaus, Hagen Hartmann, Christoph Mickel, Elena Szilvas, Michael Keiner, and Andre Sander. “Core stability in athletes: a critical analysis of current guidelines.” Sports medicine47, no. 3 (2017): 401-414
- Farrokhi, Shawn, Brittney Mazzone, Michael Schneider, Sara Gombatto, John Mayer, M. Jason Highsmith, and Brad D. Hendershot. “Biopsychosocial risk factors associated with chronic low back pain after lower limb amputation.” Medical hypotheses108 (2017): 1-9
- Moseley, G. Lorimer, and David S. Butler. Explain pain supercharged. NOI, 2017
- Maher, Chris, Martin Underwood, and Rachelle Buchbinder. “Non-specific low back pain.” The Lancet389, no. 10070 (2017): 736-747
- Engel, George L. “The need for a new medical model: a challenge for biomedicine.” Science196, no. 4286 (1977): 129-136






