


I have been meaning to write this blog for sometime. There seems to be few resources on how to best rehabilitate running related sacral bone stress injuries.
Up to 20% of all sports medicine injuries are bone stress related (Fredericson et al, 2016) with between one and two thirds of long distance runners experiencing a bone stress injury (Warden et al, 2014). Weeks & Beck (2008) published data showing the incidence of bone stress injuries across common sports, with cross-country running being the most injurious for both male and female athletes (see below).
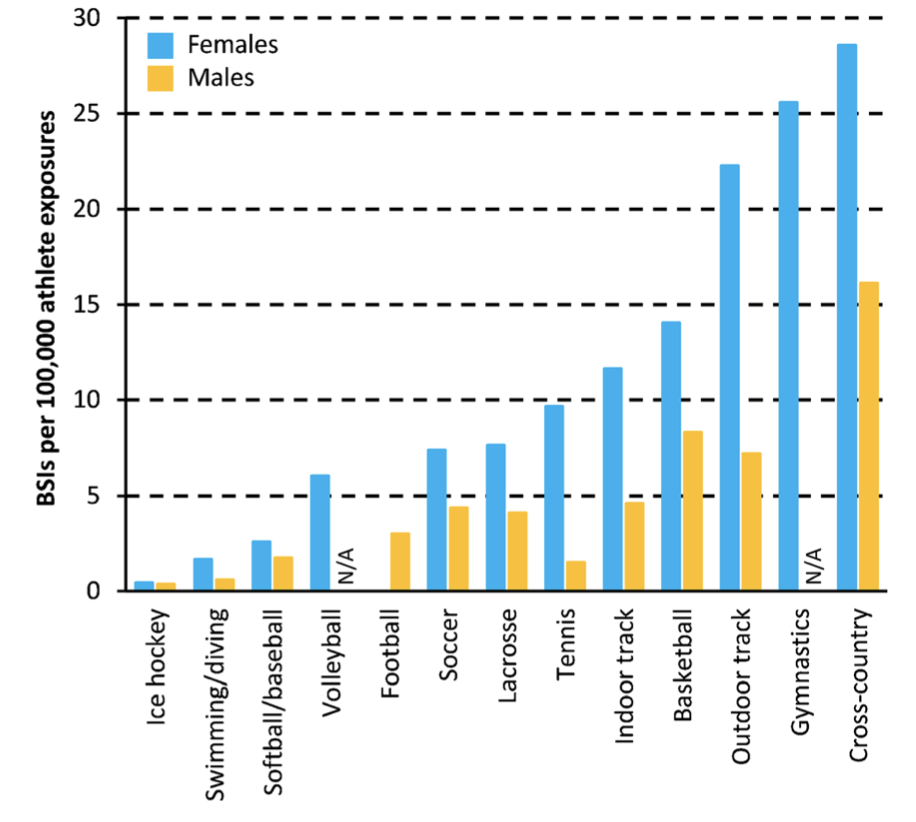
Source: Weeks & Beck (2008) The BPAQ.
Bone stress injuries occur when a region of a runner’s skeleton accumulates bone microdamage at a rate that exceeds normal bone remodelling processes. Uncoupling of bone ‘breakdown’ and ‘repair’ can be due to numerous factors in addition to the often cited ‘training errors’. Other factors can include the health of the runner’s skeleton, low energy availability, nutrient deficiencies, medical conditions, and running footwear and surface interactions.
While many runners are aware of bone stress injuries of the tibia, and foot, bone stress injuries of the sacrum are often not considered as a potential cause of a runner’s lower back/ buttock/ gluteal region pain.
While relatively ‘rare’ in recent years there have been numerous high profile running based athletes who have succumbed to sacral bone stress injuries. These include:
In 2016 Runners World published an article noting that at the time ‘run of’ sacral bone stress injuries in the elite running world (Are sacral stress fractures on the rise)
It is important that clinicians diagnose sacral bone stress injuries early to ensure the minimum impact on the athlete’s training cycle as possible. To do so, clinicians require an awareness of presenting complaints and a high index of suspicion for the running athlete.
Over the years I have observed numerous cases of running based athletes presenting with lower back/buttock region pain who have been misdiagnosed-suffering instead from symptoms related to sacral bone stress injuries.
Most recently a recreationally competitive age group triathlete presented exasperated by unilateral lower back /buttock pain. He had been treated for 6 months plus for ‘lower back pain’ with worsening of symptoms. On sending the athlete for an MRI – a sacral bone stress injury (stress fracture) was noted. Appropriate treatment ensued.
Aetiology
As with all bone stress injuries, injury onset is multifactorial.
Consideration needs to be given to factors that modify the bone workload itself as well as the ability of the runner’s skeleton to absorb that respective workload. Factors that modify bone workload can include training programs, running surfaces, running footwear, running technique, and muscle capacity of the running kinetic chain. Professor Stuart Warden et al refers to these factors as ‘biomechanical factors’.
Concurrently consideration also needs to be given to risk factors that influence the ability of the runner’s skeleton to resist accumulated microdamage that occurs with distance running. Warden et al refer to these risk factors as ‘biological risk factors’.
These risk factors are depicted below in an image I use when presenting on the rehabilitation of bone stress injuries.
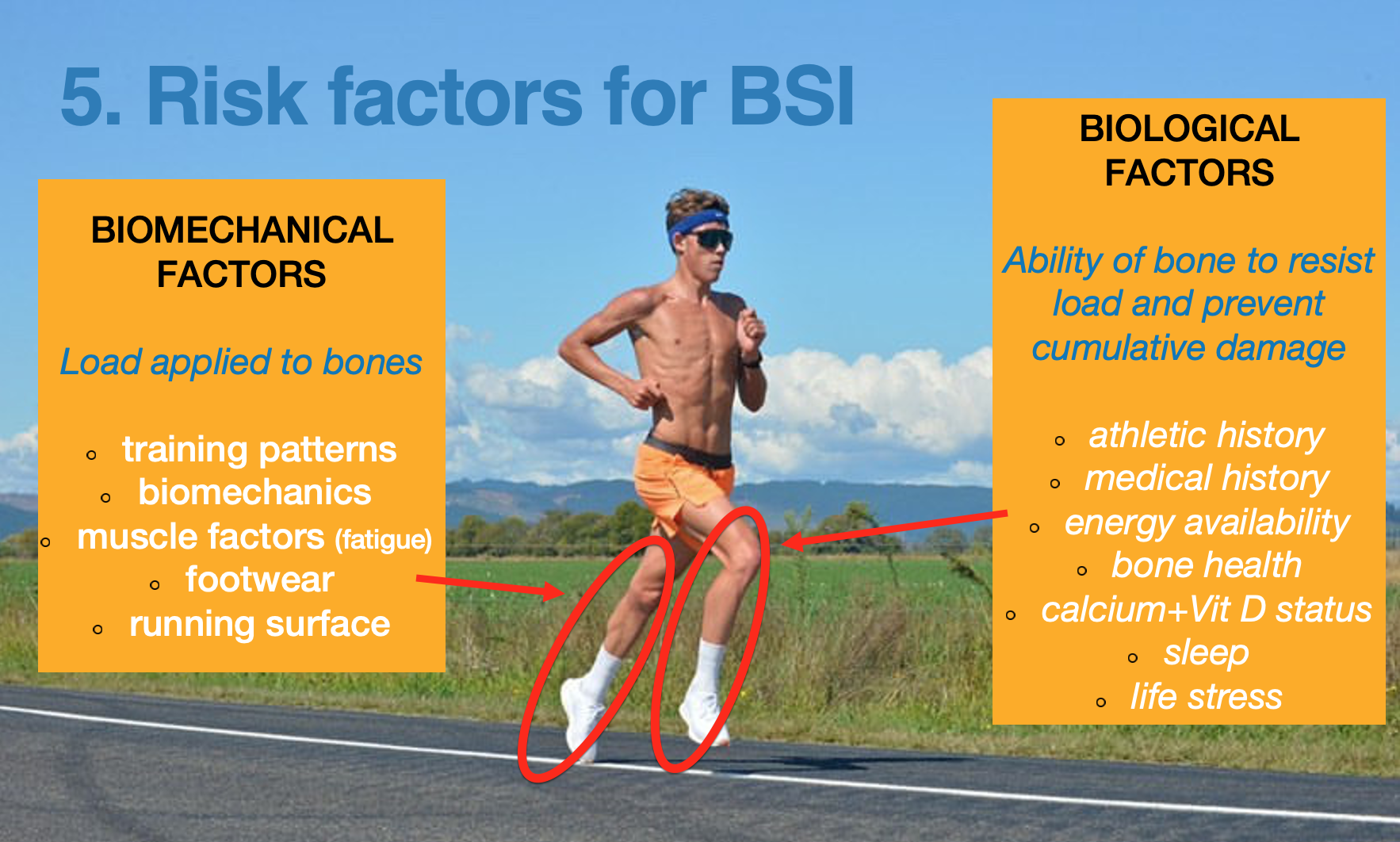
In my clinical experience there can be an over attribution of focus given to biomechanical factors, however a neglect (partial or full) of consideration when it comes to the biological factors such as energy availability and the runner’s bone health. This can be due to ignorance that the role of biological factors can play, or perhaps the difficulty of modifying biological factors as opposed to the greater ease of addressing biomechanical factors may be explanatory of this observation.
Classically when diagnosing sacral stress fractures practitioners will aim to delineate between fatigue fractures and insufficiency fractures. However delineating between fatigue fractures and insufficiency fractures is difficult in running related athletes. Fatigue fractures occur when healthy skeletons (ie sound bone health) are exposed to injurious workloads and the accrual of associated bone microdamage. While insufficiency fractures occur when ‘unhealthy skeletons’ (ie low bone mineral density, high bone turnover) are exposed to ‘normal’ physiological loads. In many runners excessive skeletal loading is accompanied by varying degrees of skeletal fragility and heightened bone stress injury risk, hence the distinction between insufficiency and fatigue fractures are not helpful or applicable to the running athlete, who may by definition be classified as having both an insufficiency and fatigue fracture/injury.
We will discuss both biological and biomechanical factors in more detail in the rehabilitation of sacral bone stress injuries below.
Where do sacral bones stress injuries occur?
Bone stress injuries of the sacrum occur in three regions of the sacrum. Injuries can occur lateral to the sacral foramina -affecting the sacral ‘wing (Type 1), injuries involving the sacral foramina (Type 2), and injuries of the sacral body that may involve the spinal canal and result in neurological signs (Type 3). This classification system is adapted from the ‘Denis Classification’. Type 3 fractures can be longitudinal running ‘across’ the sacral body.
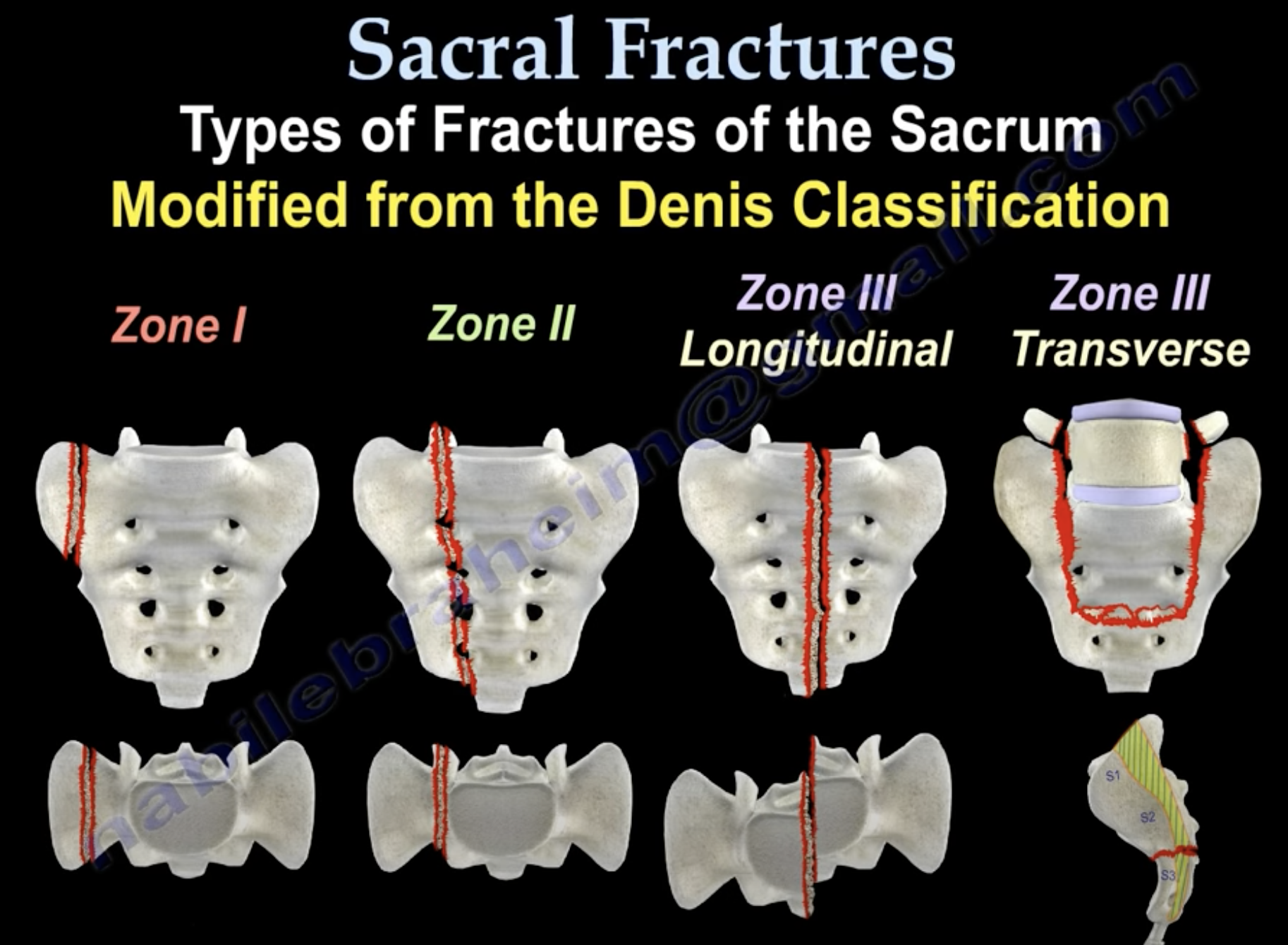
Sacral stress fracture locations. Source: Sacral Fractures – Everything You Need To Know – Dr. Nabil Ebraheim
The below images are MRI images of a 22yr old runner with a sacral stress fracture. (B) T2 axial fat suppressed images showing sacral ala stress fracture with surrounding bone marrow oedema. (C) Coronal T1 images showing showing fracture line and bone marrow oedema. (D) Coronal T2 weighted images clearly showing fracture line in saral ala.
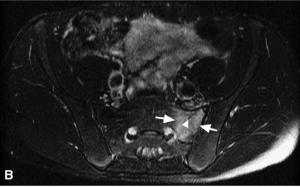
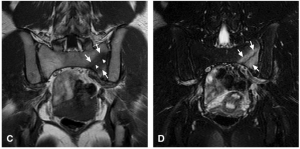
Source: Reproduced with permission from Fredericson M, Jennings F, Beaulieu C, et al. Stress fractures in athletes. Top Magn Reson Imaging. 2006;17(5):309–325
Presentation
The runner presenting with a sacral bone stress injury often complains of a deep and ‘diffuse’ (ie not localised) pain around the lower back/ buttock region. Pain will typically be unilateral (one sided). The pain is made worse with impact loading activities (e.g. running), and if further along the bone stress injury continuum pain may be reported with walking and even standing.
Physical examination findings may include:
- Tenderness on palpation of the sacrum/ SIJ region
- Pain on impact load assessments such as pogo hop> single leg hop (exercise caution with indexing these tests)
- SIJ ‘provocative tests’ such as the sacral thrust, compression, and distraction test may be positive. Learn more HERE>>
Differential diagnosis
Other conditions to consider can include: lower back pain with referral (e.g. L5/ S1 nerve root irritation/compression), SIJ pain, and deep gluteal syndrome.
A comprehensive subjective assessment and physical examination will be key. However accompanying imaging is typically required for a definitive diagnosis to be made. MRI represents the best imaging modality in terms of sensitivity and specificity.
Clinically I find the MRI findings will assist the runner in ‘owning’ their diagnosis and complying with the oftentimes protracted period of time required to return to running.
Treatment of sacral bone stress injuries in runners
Attention needs to be given to all potential factors that may have resulted in the sacral bone stress injury. These can include training workload errors, energy availability deficits, and potentially poor bone health for the runner. That is a full work up of all potential aforementioned biomechanical and biological risk factors should be undertaken.
The ‘steps’ of rehab are as follows:
1.Deload the affected bone
The first key is to decrease pain and restore pain free walking. The runner will be required to cease from running. If the athlete is experiencing symptoms with weight bearing they should partial weight bear with the use of crutches. Crutches may be used for an initial period of skeletal deloading up until the athlete can mobilise without pain. This may take 1-2 weeks. Once the athlete is pan free crutches/ mobility aid use can be discontinued, and full weight bearing can be recommenced.
The time between injury and commencement of a staged return to run program used to be typically time based e.g. 4, 6, 8, 12 weeks before recommencing, however contemporary best practice is to be symptom led and look to expose the affected bone to staged and progressive loading once pain free ambulation has been achieved.
Pathophysiologically when it comes to bone remodelling osteoclast activation and resorption in cortical bone has been reported to take approximately 4 weeks, with new bone being replaced at around the 3 month mark (Warden et al, 2021). This process takes longer in trabecular bone, hence why bones such as the trabecular rich sacrum may take longer to heal (Warden et al, 2021).
Repeat imaging (MRI) can be useful in avoiding premature return to a training program
2.Complete review of all possible factors that contributed to the injury
While in the deloading phase the runner will not be able to be biomechanically assessed; biological factors can be thoroughly explored and treated where indicated.
Consideration needs to be given to:
Training errors
It has been estimated that 60% of all running injuries are due to training errors (Hreljac et al ,2005). In the literature adolescent runners who ran greater than 32km a week had an increased risk of BSI (Tenforde, et al, 2013). While athletes who trained more than 700 hours during a year (>13hrs week) had 2.1-fold risk for an overuse injury compared to the others (Ristolainen et al, 2014).
Meanwhile Warden et al (2021) report that BSI symptoms typically begin appearing approximately 3-4 weeks following a major workload ‘error’. Such errors may include insufficient recovery time between bone loading bouts (i.e. training sessions), sudden increases in weekly workload in terms of number of loading cycles (i.e. miles or kilometres run), and/or an increase in training intensity.
When reviewing training workloads looking for potential injury causative ‘errors’ the treating practitioner, coach, and athlete should give strong consideration to the role that intensity of running may have played in the injury onset.
Bone microdamage accumulation occurs as a result of the number of loading cycles, rate of loading, and the magnitude of the applied loads. Load magnitude which is a function of running intensity is by far the most important in terms of BSI risk (Warden et al, 2021).
An inverse relationship exists between the number of loading cycles and the load magnitude, whereby just a small increase in the load magnitude can dramatically reduce the fatigue threshold point of a bone. A bone modelling study 10% increase in load magnitude (i.e. 10% increase in running pace) resulted in halving the number of loading cycles before bone failure (Warden et al, 2021).
Bone health
I have clinically observed that when a runner is diagnosed with a pelvic/proximal bone stress injury attention needs to be given to the runner’s bone health. Bone health encapsulates the ability of the skeleton to absorb the running workload, including architectural features of bone’s such as critical thickness, bone mineral density, and bone geometry. Bone mineral density is easy to quantify and can be readily assessed via dual-energy X-ray absorptiometry (DXA). There is often an assumption that runner’s have ‘robust skeletons’ as they regularly participate in loaded and repetitive activity.
However the repetitive loading profile of distance running results in bone cells quickly becoming desensitised to running loads, with the result being a poor ‘osteogenic’ (bone building) potential. Warden et al (2021) cite that distance running ‘does not build good bones’. Rather the greatest osteogenic stimulus is found with loading that is intermittent, involves explosive jumping/sprinting, with a changes of direction (Warden et al, 2021).
Barrack et al (2008) reported that up to 40% of female adolescent cross country runners had a DXA z-score of below -1 (osteopenia) for spinal (L1-L4) bone mineral density.
Specifically relating to sacral bone stress fractures Fredericson et al (2003) found that of the 12 women with sacral stress fractures in their study, 7 women had reduced bone density (osteopenia) via DXA assessment, while 2 women had osteoporosis. While 2 of the 9 men in their study met the criteria for osteopenia.
One of the chief reasons for low bone mineral density amongst runners is due to the high prevalence of relative energy deficiency in sport (RED-S) amongst both male and female distance runners. RED-S is the contemporary term for the Female Athlete Triad that the IOC championed in 2014 in order to recognise that male athletes can suffer ill effects also from low energy availability and high energy expenditure.
RED-S is common in both male and female middle and long distance runners. Koehler et al. (2013) reported RED-S to be more common in female (58%) than male (51%) endurance athletes. In elite athletics the prevalence of clinical low energy availability was 31% and 25% in female and male middle- and long-distance athletes (Heikura et al, 2017).
RED-S is a diagnosis of exclusion being diagnosed primarily via secondary indicators such as menstrual irregularity or amenorrhoea, reduction in libido, decreased morning erectile function for male athletes. The below infographic outlines these secondary indicators of RED-S.
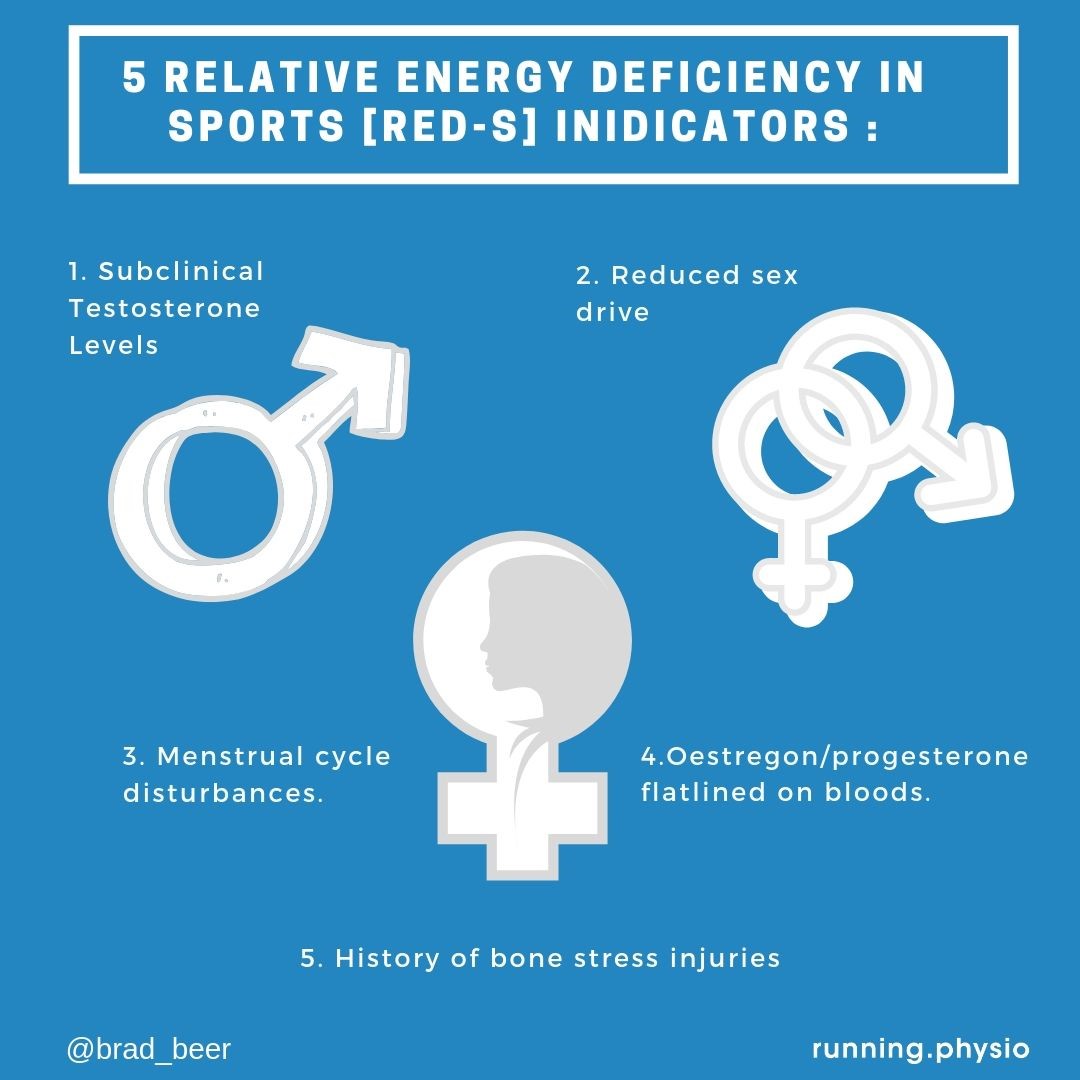
Energy availability/RED-S:
9 of the 12 women in the Fredericson et al (2003) sacral stress fracture study were amenorrhoeic. Amenorrhoea and irregular menstrual function is a hallmark sign for the female athlete of low energy availability. Specific for female athletes studies have reported that proper reproductive (hypothalamic-pituitary-ovarian axis) physiological functioning is achieved with an energy availability of 30kcal/kg of fat free mass per day, while 45kcal/kg of fat free mass is required daily in order to maintain bone metabolism.
It is well established that low energy availability contributes to impaired bone health in athletes via the down regulatory effects on gonadal steroid production.
For male athletes low testosterone levels (associated with prolonged endurance training) has been associated with low BMD scores (Hind et al, 2006).
It is important to screen runners with a bone stress injury for RED-S, for optimal recovery, and health and performance of the athlete. Including a dietitian, preferably sports focussed dietitian is key in screening for possible low energy availability and the concomitant problems that result from it.
It is believed that proximal bone stress injuries are more commonly associated with low energy availability. This may be due to the higher composition of trabecular rich bone more proximally. Historically pelvic bone stress injuries were classified as ‘low risk’, however in recent times studies have noted that trabecular rich bone injury sites such as the sacrum are associated with longer return to sport timeframes and longer healing times.
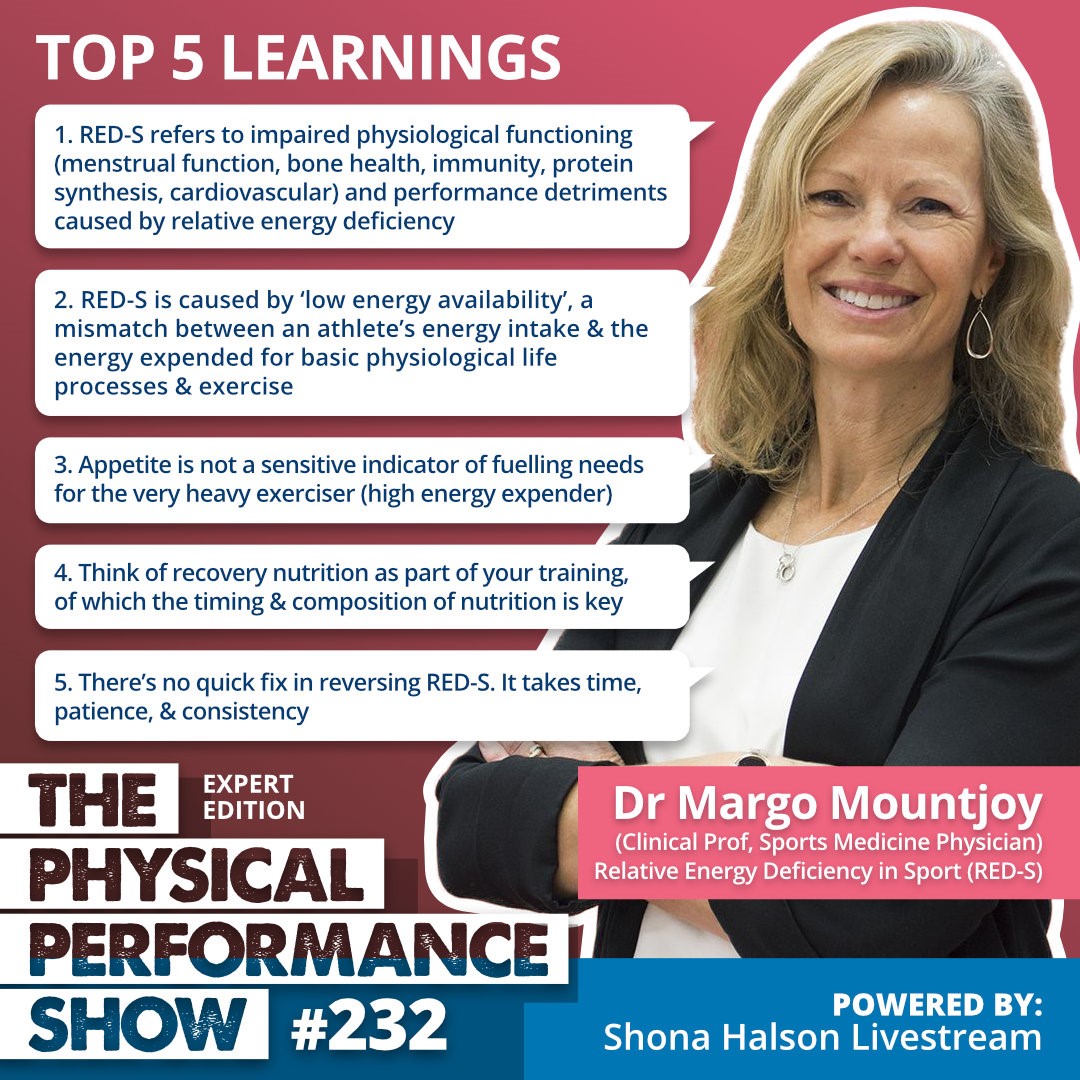
To learn more about RED-S listen to Episode 232 The Physical Performance Show
Nutrient availability
With any bone stress injury in a runner clinically I see it as a good opportunity to assess Vit D status and calcium intake. These can be undertaken by a General Practitioner ordering bloods to ascertain Vit D status, and a dietitian reviewing calcium intake.
There exists a high prevalence of Vitamin D deficiency in runners, with low Vitamin D levels having been associated with increased incidence of BSI (Ruohola, et al, 2006).
Meanwhile female runners who consumed less than 800mg calcium per day, were found to have a 600% greater stress fracture rate than female runners who consumed greater than 1500mg of calcium per day (Nattiv et al, 2013).
Dietary calcium intake recommendations are:
Adults need to have an intake of 1,000mg calcium (recommended daily intake, RDI). This should increase to 1,300mg for women over 50yrs of age, and men over 70yrs. Athletes daily intake would ideally be greater given the large amount of calcium that is lost in sweat. It has been suggested that amenorrheic female runners and males with BSI risk factors may require an additional 500mg of daily calcium intake to assist with required calcium homeostasis (Harrast, M, 2019).
Meanwhile bone health experts recommend between 1000 and 2000 IU/day for maintenance of optimal Vitamin D levels.
Related: Calcium levels for runners: a dairy -free example of meeting the calcium RDI
3. Commence appropriate S&C and cross training
Once the runner is symptom free with walking they can typically commence cross training. This may include swimming, cycling, or water running. Consideration would need to be given to cycling loads due to possible exacerbation of symptoms from sitting pressure on the sacrum.
Strength training is currently somewhat ‘controversial’ in the bone rehabilitation world. Given that we now know that the greater component of internal bone loads comes from muscle contractions as opposed to ground reaction forces (Matijevich et al, 2019, there is speculation as to whether muscle strength work may be beneficial or potentially detrimental for bone repair timelines.
Clinically I believe it is protective and as such I commence runners on targeted home and gym strength & conditioning programs as early as possible. Clinical judgement must be used for the start of the programs and also for effective progressions.
The scientific literature cites that when muscles surrounding bones become weakened or fatigued their ability to attenuate impact bone loads is lessened, resulting in increases in skeletal bone loading, and heightened BSI risk ( Milgrom et al, 2007).
Muscle size (Beck et al, 2000) and strength (Hoffman, et al, 1999) have also been correlated with a protective role of muscle in stress fracture development.
Exercise prescription should be targeted at the local area (ie lumbo-pelvic region), as well as distally, ensuring that any deficits in the running kinetic chain are addressed.
For more information on strength and conditioning for runners:
4. Commence return to run program
Consideration may need to be given to potential repeat MRI may be indicated to avoid false starts with training program resumption.
Fredericson et al (2003) reported that runners recovering from high grade sacral bone stress injuries can commence a return to run program around 10-12weeks.
Fredericson also reported that all 21 of the runners who had sustained sacral stress fractures in their study were cleared for the commencement of a return to run program between 8 and 12 weeks post diagnosis, resuming pre-injury training workloads between 3 and 6 months.
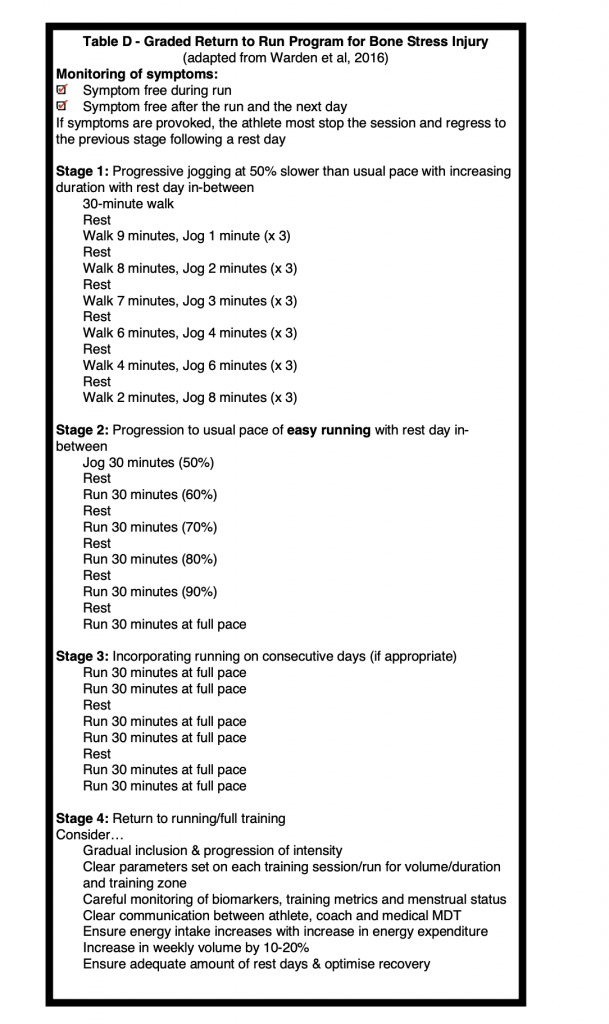
It should be noted that return to run programs remain mostly ‘art’ but they can incorporate guidelines from scientific findings.
Some key considerations when progressing return to run programs are pictured in the below infographic and supporting notes:
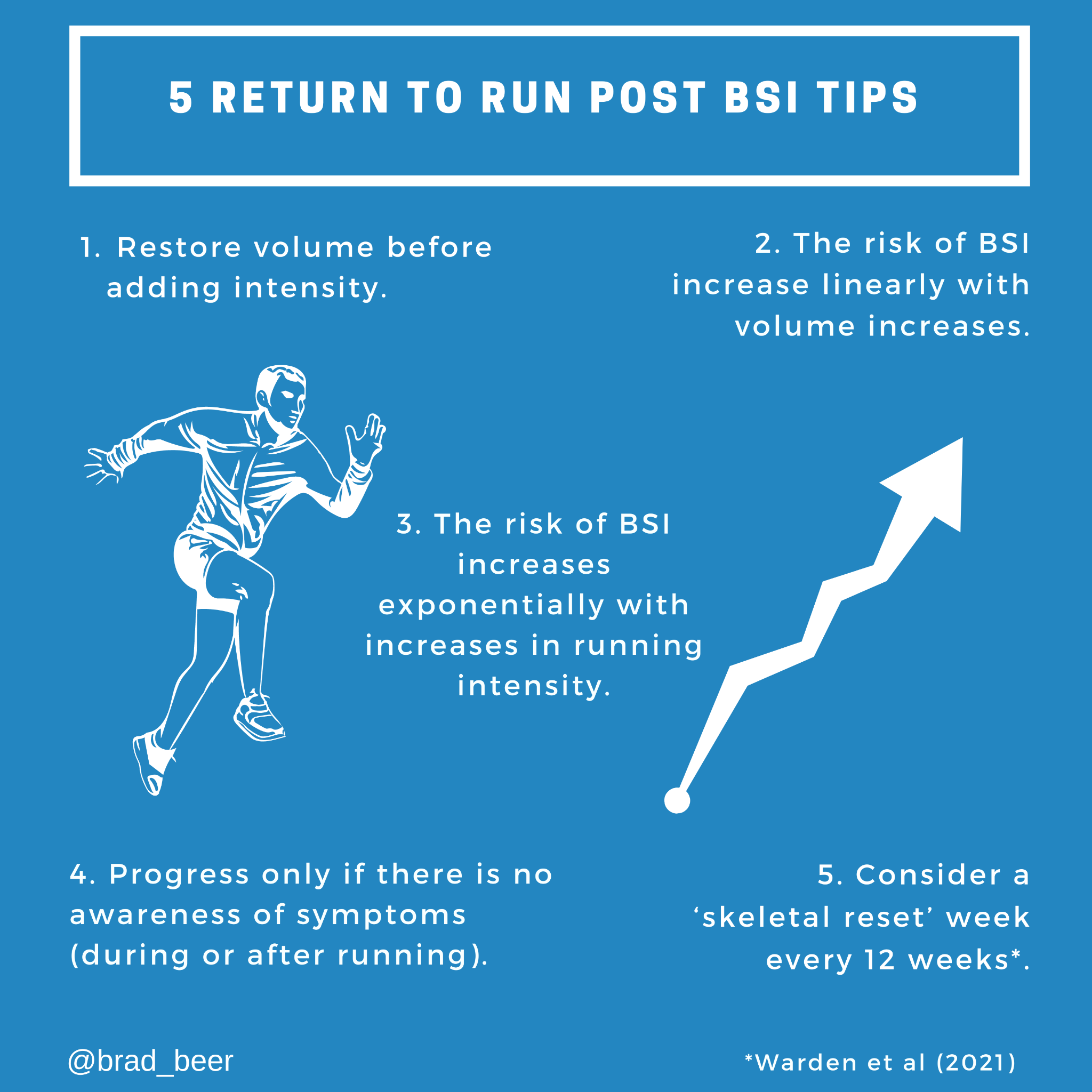
- Tip 1. Restore running volume before adding intensity. This principle applies for all running related injuries. As challenging as it can beware of increasing volume whilst also increasing intensity
- Tip 2. Acknowledge that there is a linear risk of BSI onset with training volume increases. That is, an increase in loading cycles (minutes/ volume) confers a 1:1 elevated risk of a BSI.
- Tip 3. Be discerning with prescribing intensity running as part of the return to run program. There’s an exponential increase in BSI risk with increases in bone load magnitudes (factor of running intensity). As aforementioned a 10% increase in tissue stress/strain results in halving the number of loading cycles before bone fatigue failure (Warden et al, 2021)
- Tip 4. Progress workload only in the absence of any symptoms either during or after running.
- Tip 5. Consider a skeletal reset/ de loading week. Warden et al (2021) propose distance runners may benefit from including a ‘skeletal reset’ week e.g. every 12th week. This is to avoid the accumulation of bone micro-damage & to assist in restoring bone mechano-sensitivity.
While there are no set ‘recipes’ for programs tailored to every individual athlete’s needs it is a popular practice for runners and coaches to use known return to run programs such as:
- Steve Cole program
- Bolthouse et al
- Warden et al (as depicted below)
If lower body positive pressure treadmills e.g. anti gravity treadmills are accessible the runner may engage the use of such technology which can have the potential benefits of an earlier return to some controlled loading, and increased loading cycle exposure due to the reduced body weight environment. If using an anti gravity treadmill monitoring for symptoms with workload progressions is the same as if the runner is progressing with overground running.
5. Assess running biomechanics
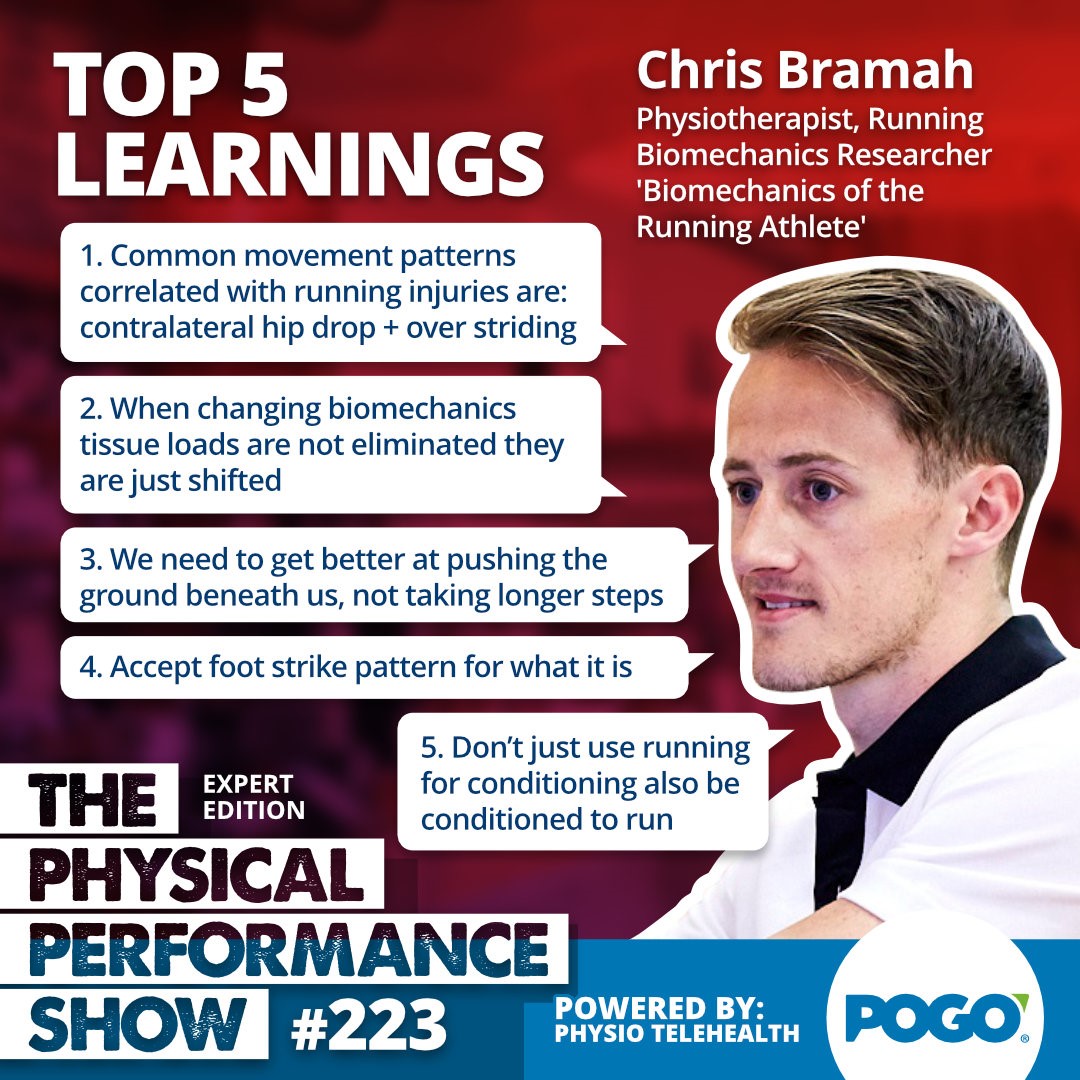
When it comes to running biomechanics and the correlation with running related injuries Bramah et al (2018) reported that ‘hip dip’ and overstriding were two biomechanical traits linked with running injury onset in both recreational and elite runners.
Dr Rich Willy in Bone Stress Injuries: Diagnosis, Treatment, & Prevention (2021) outlines that running with a narrow step width increases varus loads that act on the lower limb, tibial stress, and hip adduction. While running with a wider step width reduces these variables.
Hence a biomechanical assessment of the runner rehabilitating from a sacral stress injury is warranted assessing for overstriding, cross over gait/narrow step width, and pelvic control. This can be undertaken on a treadmill with a smart phone.
To learn more about running biomechanics listen HERE>> Podcast Chris Bramah: Biomechanics of the Running Athlete
In Summary
As with any rehabilitation effort from any running related bone stress injury, rehabilitation for sacral bone stress injuries needs to be multifactorial in approach. Strong consideration needs to be given to the athlete’s fuelling, training workload, and potentially biomechanics.
Return to run programs need to honour key principles such as re-establishing volume before adding intensity, alongside wise workload progressions, all while monitoring for symptoms.
Returning to full training workload following a sacral bone stress injury will take an athlete months, not merely weeks.
Related
- What causes bone stress injuries (blog)
- Sacral stress fractures (blog)
- Preventing bone stress injuries in runners (podcast Professor Stuart Warden)
- Fuelling the Endurance Athlete (podcast Renee Mcgregor)
- Effective Rehab for Runners with Bone Stress- Professor Stuart Warden JOSPT Insights podcast

If you need help
If you need help with a running related injury please make contact b.beer@pogophysio.com.au
We offer in person appointments and also telehealth consultations-used by runners internationally to get back to their best.

Brad Beer
APA Titled Sports & Exercise Physiotherapist (APAM), POGO Founder
Book an Appointment with Brad here.
Featured in the Top 50 Physical Therapy Blog
References
- Fredericson M, Jennings F, Beaulieu C, Matheson GO. Stress fractures in athletes. Top Magn Reson Imaging. 2006 Oct;17(5):309-25. doi: 10.1097/RMR.0b013e3180421c8c. PMID: 17414993.
- Fredericson M, Salamancha L, Beaulieu C. Sacral stress fractures: tracking down nonspecific pain in distance runners. Phys Sportsmed. 2003 Feb;31(2):31-42. doi: 10.3810/psm.2003.02.189. PMID: 20086455.
- Barrack MT, Rauh MJ, Nichols JF. Prevalence of and traits associated with low BMD among female adolescent runners. Med Sci Sports Exerc. 2008 Dec;40(12):2015-21. doi: 10.1249/MSS.0b013e3181822ea0. PMID: 18981950.
- Warden A, Davis I, Fredericson M. Management and prevention of bone stress injuries in long distance runners: A clinical commentary. J Orthop Sports Phys Therap. 2014; 44 (10): 749-765 doi: 10.2519/jospt.2014.5334.
- Weeks BK, Beck BR. The BPAQ: a bone-specific physical activity assessment instrument. Osteoporos Int. 2008 Nov;19(11):1567-77. doi: 10.1007/s00198-008-0606-2. Epub 2008 Apr 15. PMID: 18414964.
- Koehler K, Achtzehn S, Braun H, Mester J, Schaenzer W. Comparison of self-reported energy availability and metabolic hormones to assess adequacy of dietary energy intake in young elite athletes. Appl Physiol Nutr Metab. 2013;38(7):725-733. doi:10.1139/apnm-2012-0373.
- Heikura, Ida & Uusitalo, Arja & Stellingwerff, Trent & Bergland, Dan & Mero, Antti & Burke, Louise. (2017). Low Energy Availability is Difficult to Assess But Outcomes Have Large Impact on Bone Injury Rates in Elite Distance Athletes. International Journal of Sport Nutrition and Exercise Metabolism. 28. 1-30. 10.1123/ijsnem.2017-0313.
- Hind K, Truscott JG, Evans JA. Low lumbar spine bone mineral density in both male and female endurance runners. Bone. 2006 Oct;39(4):880-5. doi: 10.1016/j.bone.2006.03.012. Epub 2006 May 6. PMID: 16682267.
- Tenforde AS, Sayres LC, McCurdy ML, Sainani KL, Fredericson M. Identifying sex-specific risk factors for stress fractures in adolescent runners. Med Sci Sports Exerc. 2013;45(10):1843-1851. doi:10.1249/MSS.0b013e3182963d75.
- Ristolainen et al (2014) Training related risk factors in the aetiology of overuse injuries in endurance sports. J Sports Med Phys Fitness. 54 (1), 78-97.
- Matijevich ES, Branscombe LM, Scott LR, Zelik KE. Ground reaction force metrics are not strongly correlated with tibial bone load when running across speeds and slopes: Implications for science, sport and wearable tech. PLoS One. 2019 Jan 17;14(1):e0210000. doi: 10.1371/journal.pone.0210000. PMID: 30653510; PMCID: PMC6336327.
- Milgrom C, Finestone A, Segev S et al. Are overground or treadmill runners more likely to sustain tibial stress fracture? Br J Sports Med 2003;37(2):160–3.
- Beck TJ, Ruff CB, Shaffer RA et al. Stress fracture in military recruits: gender differences in muscle and bone susceptibility factors. Bone 2000;27(3):437–44
- Hoffman JR, Chapnik L, Shamis A et al. The effect of leg strength on the incidence of lower extremity overuse injuries during military training. Mil Med 1999;164(2):153–6.
- Ruohola JP, Laaksi I, Ylikomi T, et al. Association between serum 25(OH)D concentrations and bone stress fractures in Finnish young men. J Bone Miner Res. 2006;21(9):1483-1488. doi:10.1359/jbmr.060607
- Nattiv A, Kennedy G, Barrack MT, Abdelkerim A, Goolsby MA, Arends JC, Seeger LL. Correlation of MRI grading of bone stress injuries with clinical risk factors and return to play: a 5-year prospective study in collegiate track and field athletes. Am J Sports Med. 2013 Aug;41(8):1930-41. doi: 10.1177/0363546513490645. Epub 2013 Jul 3. PMID: 23825184; PMCID: PMC4367232.
- Bramah C, Preece SJ, Gill N, Herrington L. Is There a Pathological Gait Associated With Common Soft Tissue Running Injuries? Am J Sports Med. 2018 Oct;46(12):3023-3031. doi: 10.1177/0363546518793657. Epub 2018 Sep 7. PMID: 30193080.




