
Sacral fractures can seem like one of those problems that are rare and you’ll never get – however they are deceptively more common than you would expect. Sacral stress fractures are often unsuspected and can deceive patients and clinicians alike as they present similarly to more common conditions like disc degeneration, disc bulges, hamstring and lower back muscle strains – as well as other conditions like facet arthropathies, spondylolisthesis and trochanteric bursitis (1).
Anatomy
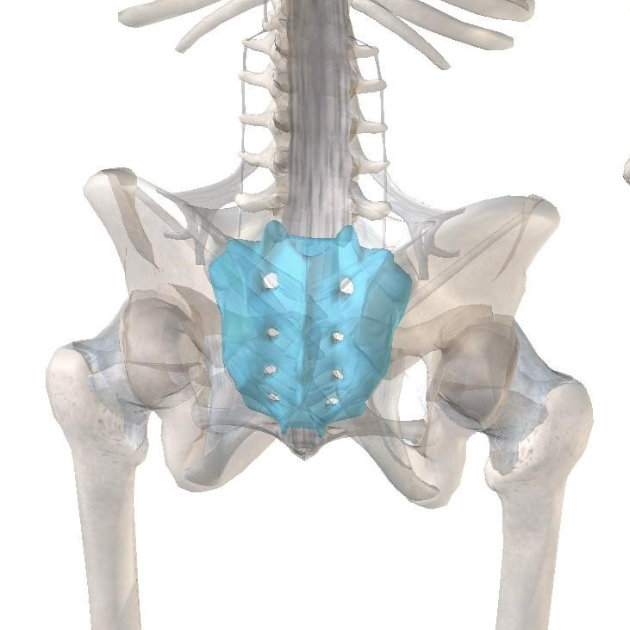
The sacrum or “Os Sacrum” (sacred bone) was so named by the Romans as a direct translation from the older Greek hieron osteon (3). Hieron primarily meaning “holy,” but also “large,” “great,” and “magnificent” – potentially for its role and regional significance (3). Thus the Sacrum, AKA “holy/large bone” is a triangular or shield-shaped bone at the base of the spine comprising 5 vertebral segments. It sits between the two Iliac bones of the pelvis – helping to distribute weight from the spine into the legs and feet. Because of this crucial role in weight/force transference, it can be vulnerable to damage.
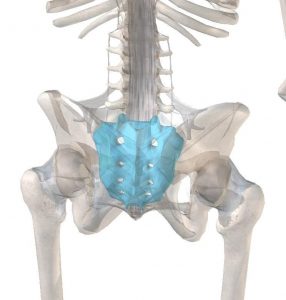
Source: www.visiblebody.com
Sacral stress fractures commonly present with an insidious onset of vague low back, buttock and/or pelvic pain #physiowithafinishline @pogophysio Share on XSacral stress fractures commonly present with an insidious onset of vague low back, buttock and/or pelvic pain (1,2). They can be divided into two main categories; insufficiency and fatigue, which are separated based on differing bone physiology and mechanism of injury (1):
Types:
- Insufficiency: Insufficiency fractures occur when normal stresses are applied to bone with decreased density, most often due to osteoporosis (1).
![]()
- Fatigue: Fatigue fractures are caused when abnormal stresses are applied to normal bone, such as from the intense training of athletes for prolonged periods (1). Fatigue fractures are common in runners – ~%20 (1)
![]()
Risk Factors
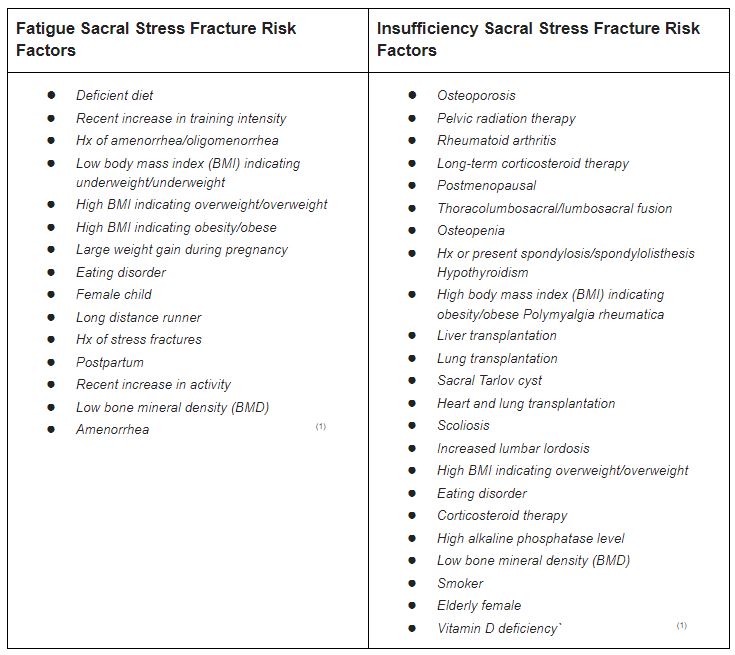
Being aware of the relevant risk factors for both fatigue and insufficiency sacral stress fractures IS KEY to preventing, identifying and treating them (1). The most common risk factors for insufficiency fractures are osteoporosis/Osteopaenia, radiation therapy, rheumatoid arthritis and long-term corticosteroid use (1). Whereas the most common risk factors for fatigue fractures are a deficient diet, a recent increase in training intensity and a high BMI (1). For a complete list of risk factors see the table below:
How are they Diagnosed?
The diagnosis of sacral stress fractures requires a combination of clinical presentation findings, imaging results, and laboratory studies (1). Whilst plain radiographs (X-rays) can pick up some sacral stress fractures, they often fail to adequately display most fractures (1,2). Thus bone scintigraphy (bone scans) and magnetic resonance imaging (MRI) are the gold standard for detecting and diagnosing sacral stress fractures (2).
Treatment
Treatment for Sacral stress fractures of course differs greatly depending on the age of the person and type of sacral stress fracture they have. Most people improve symptomatically following conservative therapy, the time course can be prolonged and quite variable. The following broad treatment strategies are recommended for sacral stress fractures:
- Medication:
- Pain control: e.g. Paracetamol (NSAIDS are not recommended as they can interfere with normal bone healing processes) (4)
- Vitamin D and Calcium: Vitamin D deficiency is common in those with osteoporosis (4)
- Biophosphonates: inhibits bone resorption – assists in maintaining bone mineral density (4)
- Bed Rest/ Immobilisation Vs Early Mobilisation:
People with sacral stress fractures were commonly recommended bed rest and immobilisation for 3-6 months – however reduced weight bearing can:- Accelerate loss of bone mineral density
- Increase incidence of deep vein thrombosis, pulmonary embolus, loss of muscle strength, negative calcium balance, decubitis ulcer and pneumonia
- Reduce performance of the cardiovascular system, urinary tract complications and even
- Worsen osteoporosis – without considering the psychological side effects (4)
 Early mobilisation is key to optimal recovery in cases that do not require surgical intervention (1,4)
Early mobilisation is key to optimal recovery in cases that do not require surgical intervention (1,4)
Weight-bearing and muscle tension induce a hormetic response in osteoblastic activity, which results in bone formation. Whereas a prolonged bed rest may cause unrestrained osteoclastic-mediated bone resorption – reducing bone mineral density. (1,4)
In simpler terms – we need to place just enough stress through the fractured area by weight bearing in our legs to maintain that the amount of weight bearing does not worsen or impair fracture healing (1,4)
- Surgery
People commonly only need surgical treatment if there is instability or detectable motion at the fracture site, or if neurological defects or severe disruptions of sacrum alignment are present (4)
Procedures:
- Sacroplasty – a procedure where cement is injected by a interventional radiologist under CT guidance into fracture lines has shown positive results but requires further research to understand its long term results/ any adverse effects (4)
You should consult your GP and Physiotherapist for the best treatment options relative to your age and circumstance before considering the strategies mentioned above.

Oliver Crossley (APAM)
POGO Physiotherapist
Featured in the Top 50 Physical Therapy Blog
References
- Yoder, Kristi, Jenna Bartsokas, Kristina Averell, Erin McBride, Christine Long, and Chad Cook. “Risk factors associated with sacral stress fractures: a systematic review.” Journal of Manual & Manipulative Therapy 23, no. 2 (2015): 84-92.
- Lyders, E. M., C. T. Whitlow, M. D. Baker, and P. P. Morris. “Imaging and treatment of sacral insufficiency fractures.” American Journal of Neuroradiology 31, no. 2 (2010): 201-210.
- Sugar, Oscar. “How the sacrum got its name.” JAMA 257, no. 15 (1987): 2061-2063.
- Longhino, Valentina, Cristina Bonora, and Valerio Sansone. “The management of sacral stress fractures: current concepts.” Clinical cases in mineral and bone metabolism 8, no. 3 (2011): 19.





2 responses to “Sacral Stress Fractures”
Hi, I have a question about restless leg syndrome during marathon training. Do you know what causes this and how to treat it?
Thanks!
Lisa
Hi Lisa,
Thanks for your question.
I interpret your query to mean that you are getting evening leg symptoms that are disturbing your sleep.
Tune into this Expert Edition of The Physical Performance Show (34:34 in) where sleep physician Dr Cunnington speaks about restless leg syndrome and the causes and solution HERE>>
Regards Brad Beer
Sports & Exercise Physiotherapist