


If you’re suffering from a pain at the front of your knee then this is a blog for you to read! What is a fat pad? What does it do? Why does it hurt? And why do you want to know about it? These are all questions I will answer for you in this blog.
Anatomy & Purpose
So there’s actually three fat pads at the front of the knee but what I’m focussing on is the Infrapatella Fat Pad or sometimes called Hoffa’s Fat Pad, named after the bloke who made the first links to the fat pad being a cause of pain back in 1904.
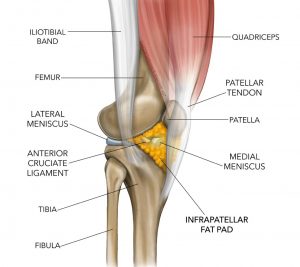
The fat pad is intraarticular meaning it actually sits within the joint but outside the synovium (joint capsule). It’s location is as follows:
- deep to the patella tendon which it attaches to
- superior attachment is to the lower patella (knee cap)
- inferior attachment on the anterior tibia.
- It blends in and attaches to the menisci, infrapatellar bursa and the intermeniscal ligament.
So the fat pad is a part of the knee joint, not just some lump of fat sitting exterior to the knee (8). It easily conforms to the movement of the knee joint and helps act as a protective cushion between articular surfaces (1). When it becomes damaged and adhesion occur, knee joint biomechanics are altered (5). A 2015 study found consistent evidence that having a larger fat pad benefited the knee and was associated with increased cartilage volume, reduced cartilage defects, and fewer bone marrow lesions and osteophytes (3).
An abundance of blood vessels supply the infrapatellar fat pad meaning it has a rich blood source. Along with the many vessels, the fat pad has a high neural innervation which arise from the femoral, obturator and sciatic nerves but the predominant supply comes from the posterior tibial nerve (8).
The intriguing part about this fat pad is that despite having the same composition as subcutaneous fat (fat under the skin), it almost never changes in size. It doesn’t get any bigger if we increase our BMI and it only ever reduces with severe malnutrition (8). Wouldn’t it be nice if the same principle applied to the rest of our body!.
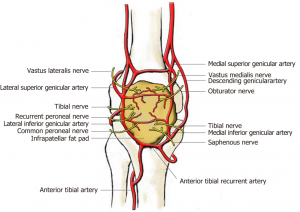
Vessel and nerve innervation of the infrapatellar fat pad
Fat Pad Pathology Presentation
- Anterior knee pain exacerbated by extension or prolonged flexion – prolonged standing will be provocative, sometimes even a straight leg raise will hurt. Passive hyperextension of the knee is likely to replicate pain. Prolonged sitting may also irritate the pain, this is known as the “cinema sign”, as in sitting in the cinema for a long period (4).
- The fat pad is tender to touch – this will be below the patella and deep to the patella tendon
- A puffy anterior knee – the fat pad is a bit like a sponge and when inflamed will become engorged in fluid (9).
- Pain may be worse when barefoot or wearing flat shoes compared with a heeled shoe
- High irritability – trivial events may lead to large flares in symptoms
- Surgical History – depending on the surgical technique, the fat pad may become inflamed if impacted during surgery.

Knee oedema due to an inflamed infrapatellar fat pad. Source: clairepatella.com
Cause of Pain
Fad pads are one of the most innervated structures in the knee and are highly sensitive with chronic inflammation possibly leading to fatty fibrosis.(1). It’s been shown that when painful there is an increase in Substance-P fibres in the fat pad which produces sensitivity to nociceptive (incoming pain/danger) signals, promotes inflammation and may directly influence pain (5). Pain can due to either mechanical or metabolic causes.
Firstly, mechanical trauma leads to an inflammatory response in the fat pad. This might be a blow to the front of the knee, occur following a recent knee surgery or even a rapid straightening of the knee. Generally the person will feel a sharp pain at the anterior knee (11). Accumulative microtrauma can also occur when the fat pad is continually caught and pinched between the patella and tibia. A predisposing factor for this impingement is an inferiorly tilted patella (2).
Secondly, the pain can be due to metabolic causes but this relationship is complex and yet to be fully explored and understood. Being obese causes general systemic inflammation which can lead to inflammation of the fat pad (11). Also in people who have knee osteoarthritis, the infrapatellar fat pad secretes increased levels of inflammatory mediators such as interleukin-6 (6,7). However, having a larger fat pad may be protective against knee OA by helping dissipate loads at the knee (3). You can see how this relationship can be confusing!
Treatment: Acute vs Chronic
The main difference between treating acute or chronic infrapatellar fat pad pain is screening for and correcting causative factors. When acute trauma is identified as the reason for inflammation, then focus is concerned primarily on offloading the fat pad and allowing it to settle. When the pain is a persistent issue that has developed over time, it’s likely there is an underlying reason that needs to be resolved.
This process can be described in two stages:
Stage 1: Reduction of Inflammation
- Activity Modification – reduce aggravating activities which may mean reducing walking time/distance, reducing prolonged standing and anything else provocative
- Wearing heeled shoes – avoiding barefoot especially if its painful
- Ice Massage
- Offload Taping – lifting the inferior patella away from the fat pad with a ‘V-Tape’ technique. This may be applied 24/7 until symptom free (4).
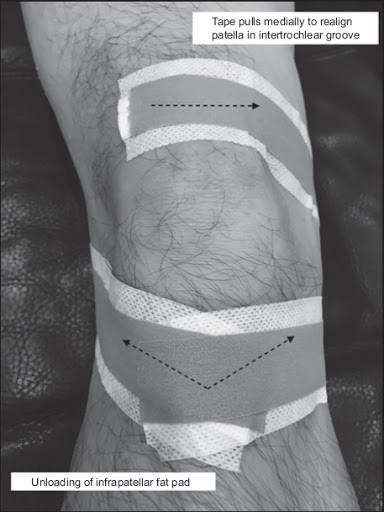
An example of ‘V-tape’ technique to offload the fat pad
Stage 2: Recondition the limb / Fix the cause
- Progressive loading exercise: with a strong focus on the quadriceps and also considering glutes and hip external rotation exercises for control of knee medialisation (knee valgus). Closed chain exercises (foot on the ground) are thought to be most effective and functional (4).
- Isometric Knee Exercise: may be useful in the early stages, working within a safe zone of 20-40° of knee flexion can be manageable if the pain is irritable (9).
- Stretching: of the quadriceps and hip flexors may be indicated in patients with the “cinema sign” or pain with prolonged knee flexion in sitting. If the quadriceps are tight, this may increase the compression of the patella on the fat pad and lead to pain (4,9). This is likely irrelevant if knee flexion is not provocative.
- Corticosteroid Injections: have been shown to improve fat pad pain (4).
- Weight loss: remember how the fat pad can become pro-inflammatory in knee OA patients, well through diet & exercise it has been shown that the fat pad volume can be reduced and thus theorised to reduce the secretion of pro-inflammatory mediators and reducing pain (10).
Things to consider assessing:
- Knee Hyperextension – if the patient has poor control over inner range quadriceps or stands often in a hyperextended position then this may irritate the fat pad. Quads control exercises may be prescribed to correct this.
- Patella Hypermobility – the patella may have a large amount of movement which can impinge the fat pad. Dynamic quad exercises can be prescribed to treat this.
- Patella position – tight structures on the lateral aspect of the knee may cause a lateral pull or maltracking. Things to assess would be the ITB, lateral retinaculum and femoral medialisation which could due to control or bony morphology issue. Multiple studies have found patella alignment changes can contribute to fat pad oedema (12,13).
These two stages may not be mutually exclusive. Treatments from each section may overlap.

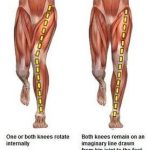
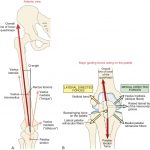
From left to right: a) knee hyperextension, b) knee valgus (left), c) forces acting on the patella
Summary
- Fat pad pathologies are not a common cause anterior knee pain but still need to be considered
- The infrapatellar fat pad is the main offender
- Symptoms include: pain in knee extension or prolonged flexion & a puffy, tender fat pad
- The fat pad is highly vascualrised, has lots of neural innervation and helps joint biomechanics
- Mechanical or metabolic stresses may lead to fat pad pain
- Treatment is broken into 2 stages: decrease inflammation & reconditioning the limb/fixing the underlying cause

James Gardiner
POGO Physiotherapist
Book an Appointment with James here.
Featured in the Top 50 Physical Therapy Blog
References
- Borja, M. J., Jose, J., Vecchione, D., Clifford, P. D., & Lesniak, B. P. (2013). Prefemoral Fat Pad Impingement Syndrome: Identification and Diagnosis. The American Journal of Orthopedics.
- Brukner, P., & Khan, K. (2016). Brukner & Khan’s Clinical Sports Medicine: Injuries (5th ed.). McGraw-Hill Education Australia.
- Cai, J., Xu, J., Wang, K., Zheng, S., He, F., Huan, S., Xu, S., Zhang, H., Laslett, L., & Ding, C. (2015). Association Between Infrapatellar Fat Pad Volume and Knee Structural Changes in Patients with Knee Osteoarthritis. The Journal of Rheumatology, 42(10), 1878-1884.
- Dragoo, J. L., Johnson, C., & McConnell, J. (2012). Evaluation and Treatment of Disorders of the Infrapatellar Fat Pad. Sports Medicine, 42(1), 51-67.
- Hannon, J., Bardenett, S., Singleton, S., & Garrison, J. C. (2016). Evaluation, Treatment, and Rehabilitation Implications of the Infrapatellar Fat Pad. Sports Health: A Multidisciplinary Approach, 8(2), 167-171.
- Ioan-Facsinay, A., & Kloppenburg, M. (2013). An emerging player in knee osteoarthritis: the infrapatellar fat pad. Arthritis Research & Therapy, 15(6), 225.
- Klein-Wieringa, I., Kloppenburg, M., Bastiaansen-Jenniskens, Y., Yusuf, E., Kwekkeboom, J., El-Bannoudi, H., Nelissen, R., Zuurmond, A., Stojanovic-Susulic, V., Van Osch, G., Toes, R., & Ioan-Facsinay, A. (2011). The infrapatellar fat pad of osteoarthritic patients has an inflammatory phenotype. British Medical Journal, 70(5).
- Mace, J., Bhatti, W., & Annand, S. (2016). Infrapatellar fat pad syndrome: a review of anatomy, function, treatment and dynamics. Acta Orthopædica Belgica, 82(1).
- (2019, November 2). Episode 003 Hoffa’s Fat Pad. http://physiotutors.libsyn.com/physiotutors-episode-003-hoffas-fat-pad
- Pogacnik Murillo, A. L., Eckstein, F., Wirth, W., Beavers, D., Loeser, R. F., Nicklas, B. J., Mihalko, S. L., Miller, G. D., Hunter, D. J., & Messier, S. P. (2017). Impact of Diet and/or Exercise Intervention on Infrapatellar Fat Pad Morphology: Secondary Analysis from the Intensive Diet and Exercise for Arthritis (IDEA) Trial. Cells Tissues Organs, 203(4), 258-266.
- Robertson, C. (2016). The infrapatellar (Hoffa’s) fat pad explained. Claire Patella. https://clairepatella.com/the-infrapatellar-hoffas-fat-pad-explained/
- Subhawong, T. K., Eng, J., Carrino, J. A., & Chhabra, A. (2010). Superolateral Hoffa’s Fat Pad Edema: Association With Patellofemoral Maltracking and Impingement. American Journal of Roentgenology, 195(6), 1367-1373.
- Campagna, R., Pessis, E., Biau, D. J., Guerini, H., Feydy, A., Thevenin, F. S., Pluot, E., Rousseau, J., & Drapé, J. (2012). Is Superolateral Hoffa Fat Pad Edema a Consequence of Impingement between Lateral Femoral Condyle and Patellar Ligament? Radiology, 263(2), 469-474.




