


How to Rehabilitate Anterior Hip Pain in Runners

Pelvic and hip injuries are some of the lesser seen injuries in runners, with less than 10% of runners reporting pain at the hip and pelvis. Of which an even smaller percentage present with anterior hip pain. As it is an uncommon area to have pain or injury, it can be confusing for runners to get diagnosed and then effectively manage and rehabilitate. Here is a comprehensive guide to anterior hip pain in the runner.
Hip Anatomy
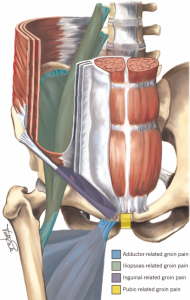
The anterior region of the hip has a number of structures that can refer symptoms into the front of the hip. In a running population symptoms can arise from the iliopsoas tendon. A conjoint tendon formed by the large Iliacus and Psoas Major muscles (known collectively as Iliopsoas), it’s commonly referred to as your hip flexor/s. Deep to the Iliopsoas tendon is the Iliopsoas bursa and femoroacetabular joint (hip joint). These can be both responsible for anterior hip symptoms. Another one of the muscles that cross the hip joint that can be a source of symptoms is rectus femoris. It is one of your quadricep muscles and acts not only to flex the hip along, but also extend the knee. Towards the midline are more commonly seen groin pain including which can be from adductor muscles, pubic bone and pubic symphysis. Just above this symptoms may arise from the inguinal canal and rectus abdominis. The picture below illustrate some of these structures.
Diagnosis
To correctly manage anterior hip pain it is important to correctly identify the source or sources of symptoms, and exclude other potential diagnosis. Groin symptoms and injuries have been covered here. For this blog our focus is on anterior hip pain occurring in runners which more commonly will fit into one (or more) of the following diagnosis.
1. Iliopsoas Strain or Rectus Femoris Strain
A strain of the hip flexors can occur at the tendon or muscle of Iliopsoas or rectus femoris. This is an uncommon injury for runners, yet most commonly occurs as an acute incident with speed work. Pain presents as an acute moment during high speed running (relative to the runner) or towards the end of a faster session. When assessing this area pain is often reproduced on stretch and contraction (4).
2. Iliopsoas tendinopathy
The Iliopsoas tendon can be a source of pain without an acute strain. This is often termed tendinopathy and involves changes to the tendon matrix which occur time and are often associated with ‘overuse.’ Tendinopathy differs from tendinitis (inflamed tendon) and paratendinitis (inflamed tendon sheath) in that the driver of symptoms is not inflammation.
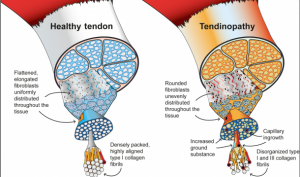
Figure source: Pathogenesis and management if tendinopathies in sports medicine (Transl Sports Med)
Iliopsoas tendinopathy often occurs with an increase in hip flexion loads. In runners this often is increased uphill running and/or speed work; particularly as a runner fatigues and loses form. This diagnosis can feel like an increased stiff and tight feeling at the front of the hip. This can also occur alongside hip dysplasia (see below).
3. Femoral Stress Fracture or Reaction
An important diagnosis not to be missed is a femoral stress reaction. Bone stress injuries are a result of an imbalance between the formation and removal of bone. Exercise creates microdamage, which acts as a stimulus for bone to remodel and deposit new bone, so it can tolerate more microdamage. When the microdamage (bone resorption) occurs quicker than the remodelling of bone, a stress reaction can occur. This can then progress further to a stress fracture depending upon the loads applied and the bone status of the runner. A femoral stress reaction often presents as anterior hip pain that can radiate down into the thigh. The femoral neck is one of the more common stress reaction sites in runners. It is often confused as tightness but is vague in location and doesn’t feel like it can be ‘stretched out’ (4). Pain is also often brought on by activity, can be painful to hop, eventually if it progresses it can be painful with everyday walking and activities (5). It is often clear on x-ray and therefore MRI is best to exclude or include as a diagnosis. Risk factors may include training errors (too much, too quick, too soon), previous injury, disordered eating, low BMD, RED-s (see here).

4. Hip Dysplasia
Developmental dysplasia of the hip (DDH) describes a spectrum of hypermobility and instability at the hip joint. Many people only associate it with newborns, where persistent subluxation of the hip or when significant instability is present plaster casting or a harness is introduced. At the lower end of this scale DDH is a high percentage of adolescents and adults, men and more commonly women with hip pain. The runner often presents with a high amount of mobility and flexibility both generally and noteably at the hip. It is thought that this extra mobility of the ball (femur) within the socket (pelvis) results in irritation of the hip joint and or surrounding structures (such as the iliopsoas tendon mentioned above). Pain can occur from an incident or slowly over time and can be unilateral or bilateral. Commonly positions of ‘hip impingement’ aggravate such as bringing the knee towards the chest, up hill walking or running and prolonged sitting. These runners also have trouble with extension based activities such as running, stairs, wearing heels, faster walking or running. You’ll often catch this person ‘hanging off their hip’ when they stand or sway which aggravates their symptoms. This is often the position someone holding a small child leans into to make it easier to hold; shifting all weight onto one leg with a straight knee.
5. FAI
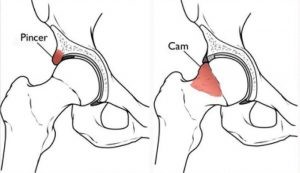
FAI or femoracetabular impingement is a diagnosis made when there are signs and symptoms of irritation of the anterior hip joint (capsule, labrum) alongside bony changes visible on xray. In people with FAI, extra bone forms on either the femoral head (cam lesion) or the acetabulum (pincer lesion). When the leg is moved into certain positions, these bony growths make contact with other aspects of the joint or soft tissue and can result in pinching symptoms or ‘impingement’ . This leg position is typically when the hip is flexed, crossing the midline and/or rotated inward. These positions can be without symptoms for a large portion of time before a spike in training loads or increased movements into this position results in symptoms. This bony morphology (CAM or PINCER) is therefore present in a large amount of sporting athletes without pain, and are often present from early adolescence. Typically it is quite rare to see in runners due to the limited ranges of hip flexion and rotation which would typically aggravate these symptoms. This can be confused with DHD in many female runners as some signs and symptoms are the same.
Hip Osteoarthritis presents as a stiff and achy hip. Osteoarthritis at the hip is a common occurrence and typically will worsen with activity and get better after relative rest. It is often seen in overlap with DDH and FAI but in someone over the age of 40 years. The symptoms that a therapist is looking for may include deep joint pain that is aggravated by certain activities such as squatting and sitting and stiffness after rest. In the physical examination, the therapist expects to find decreased range of motion, pain into particular movements and no single moment of injury. Simple imaging can help identify hip OA, however will not necessarily mean someone will have pain (that is you can have hip osteoarthritis on imaging and be painfree).
Management Principles
1. Identify Key Contributing Factors
One of the first steps before beginning treatment of the injury is to recognise key contributors to the initial injury. This provides a good opportunity to reflect on the circumstances leading to the onset of hip pain, to modify or change risk factors if able and aim to avoid making similar errors in the future. For example if you have sustained a femoral stress reaction, it might be worth checking bone mineral density for signs of osteoporosis or osteopenia. Then management can incorporate exercises which help increase bone density alongside targeted modification to nutrition. A key contributor might have been repeat nights of poor sleep. This may be something you can modify and create healthy sleep habits, or alternatively you may not need to change anything because typically you sleep well, it’s just a tool for reflection. Assessment from your health professional may identify decreased range of movement, weakness or changes in biomechanics which may impact symptoms. If identified it is then more likely to be addressed in the runner’s management, with the aim to reduce the likelihood of re-injury. Other contributing factors may include those below:
2. Modify Hip Loads
A key aspect of helping hip symptoms settle is to reduce or modify aggravating activities. Different diagnoses will require drastic differences in load modification and therefore accurate diagnosis is important. Someone with a femoral stress fracture should not be running however someone with a tendinopathy or hip OA may not need to change their running at all. It is often helpful to reduce hills and speed work in runners with anterior hip pain, particularly after a strain, those with ‘impingement,’ and tendinopathy. Tasks which involve prolonged or repeated hip flexion (knee to chest action) can be a source of aggravation particularly with DDH, Hip OA and impingement; so therefore it can be beneficial to reduce time spent sitting in low chairs, uphill or upstairs walking, stretches or yoga poses that involve hip flexion (eg prayer or child’s pose), squatting and getting in and out of the car. In addition to these positions if the cause of symptoms is DDH it may also help to reduce ‘hanging off the hip’ when standing, sitting with leg crossed, rotation exercises such as clams and positions of increased hip extension (including hip flexor stretches, long stride walking and prolonged standing especially in high heels). Some of these tasks may or may not need modifying depending on the source of symptoms and how irritable symptoms are.
3. Build Capacity
Strength and conditioning of the muscles around the hip is a key aspect of managing and treating hip pain. Depending upon the diagnosis certain hip exercises can be prone to irritating symptoms. For example a squat or leg press can be a common aggravating exercise for hip joint symptoms (OA, impingement, DDH), however a smaller squat range, sumo squat or banded goblet squat may reduce hip symptoms. If the priority of the squat is just to build up quadriceps capacity, this can often be achieved with less discomfort using a leg extension machine. Exercises that involve repeat hip internal and/or external rotation (such as clams) can also aggravate an irritable hip joint. Strength through all global hip and thigh muscles is important alongside deeper stability muscles such as gluteus medius, minimus, piriformis and small external rotators of the hip. These smaller muscles become even more important in the hypermobile client such as DDH. Building capacity can often start no matter the symptoms, it is a matter of careful exercise selection, range of motion and resistance used. Some exercises that can be incorporated are shown below.
4. Symptom Modifiers
Alongside the management principles above, other modalities may be helpful in management of symptoms. These can provide short term reductions in symptoms and will be dependent on individual diagnoses and circumstances. This may include; massage, hip mobilisations, ice, heat, dry needling, taping, medication, shockwave therapy and corticosteroid injection.
5. Education
Paramount to any management of hip pain is to understand the diagnosis. Understanding the source of symptoms, wider contributors to pain such as social and psychological factors along with specific factors affecting prognosis are important. The more informed and knowledgeable one is about their hip symptoms the more control they have over aggravating factors and hopefully the smoother the rehab.
Exercise Prescription
Exercise prescription is a key part of the rehabilitation progress and aims to increase the capacity of the tissues around the hips and lower limb to handle load. Typically this is through a combination of resistance exercises and occasional stretching. The exercises are then progressed in difficulty as pain allows, symptoms settle and strength improves. Some example Early Stage; Middle Stage and Late Stage rehab exercises are described below. This is by no means an exhaustive list of exercises and some will be more relevant to certain diagnoses than others. Modifications of numerous variables are important to maximise individual benefits such as sets, reps, tempo, time to fatigue, range of movement, technique and rest to name a few.
1. Early Stage or Irritable Hip Exercises
- Weighted Glute Bridge (Glute Max – Small Range)
- Banded Hip Abduction Side Lying (Holds or Small Range)
- Adductor Squeeze (Holds straight knee or bent knee)
- Knee Extensions
- Prone Hamstring Curls
- Isometric Sidelying Hip Flexion
2. Middle Stage Exercises
- Hip Thrust
- Bulgarian Split Squat
- Prone Hip External Rotations
- Resisted Hip Flexion Supine
- Side Plank (Knees)
3. End Stage Exercises
- Squat
- Deadlift
- Lateral Lunges
- Adductor Side Plank
- Side Plank Scissors

Lewis Craig (APAM)
POGO Physiotherapist
Masters of Physiotherapy
Featured in the Top 50 Physical Therapy Blog
References:
- Thorborg, K., Bandholm, T., Zebis, M., Andersen, L. L., Jensen, J., & Hölmich, P. (2016). Large strengthening effect of a hip-flexor training programme: a randomized controlled trial. Knee Surgery, Sports Traumatology, Arthroscopy, 24(7), 2346-2352.
- Andersson E, Oddsson L, Grundström H, Thorstensson A (1995) The role of the psoas and iliacus muscles for stability and movement of the lumbar spine, pelvis and hip. Scand J Med Sci Sports 5(1):10–16
- Deane RS, Chow JW, Tillman MD, et al. Effects of hip flexor training on sprint, shuttle run, and vertical jump performance. J Strength Cond Res. 2005;19(3):615‐621 [PubMed] [Google Scholar]
- Brukner and Kahn
- Kahanov, L., Eberman, L. E., Games, K. E., & Wasik, M. (2015). Diagnosis, treatment, and rehabilitation of stress fractures in the lower extremity in runners. Open access journal of sports medicine, 6, 87.
- Kraeutler, M. J., Garabekyan, T., Pascual-Garrido, C., & Mei-Dan, O. (2016). Hip instability: a review of hip dysplasia and other contributing factors. Muscles, ligaments and tendons journal, 6(3), 343.
- Rauseo, C. (2017). The rehabilitation of a runner with iliopsoas tendinopathy using an eccentric-biased exercise-a case report. International journal of sports physical therapy, 12(7), 1150.

![]()





