


5 MASTERS (40+yrs) RUNNER CONSIDERATIONS

The masters runner has unique needs that need to be appreciated and understood by treating practitioners and masters runners alike. Week to week a large proportion of my clinical caseload is the 40+ runner. By understanding some of the key physiological changes that occur with maturation of the runner the best rehabilitation and performance outcomes can hopefully be achieved.
The benefits of running into 40+ years are widely recognised; particularly the slowing of cardiovascular decline rate. However as a runner enters the masters years (40+) Willy & Paquette (2) state that ‘masters runners will experience an inevitable and unavoidable progressive decline physiologically, bio-mechanically and also performance wise’.
I have observed large increases in masters runners taking to endurance running in their years beyond 40 years of age, and also continuing to run into later stages of life-well beyond 40 years of age. It appears that masters athleticism and staying active beyond 40 years of age is becoming more and more expected and normalised. Perhaps athletes like Kelly Slater (surfing), Craig Alexander (triathlon), and Bernard Lagat (running) are redefining what’s possible through their impressive 40years+ performances. Improvements and progressions in healthcare practices and the science that underpins it is also seemingly providing runners with the ability and expectation that running across a lifespan is not only helpful but also possible.
An example of the increase in masters runners is the number of finishers at the New York City Marathon greater than 40 years of age has increased by a multiple of 1.7x over approximately a two decade period circa 1980-circa 2000 (1).
With more and more runners running into their masters years readily available information that can aide masters runners in their quest to enjoy their best possible running is important. Such trends in greater masters runners participation can only be a good thing for the promotion of healthy ageing of the population.
This blog will explore 5 considerations for the masters runner, outlined below.
1.Differences in injury profile for masters runners compared with younger runners
Willy and Paquette (2) in their review of masters runner literature reported that masters runners tend to experience greater amounts of muscle and tendon injuries to below the knee structures such as the ‘calf complex’ (gastrocnemius and soleus), achilles tendon, and hamstrings (2). This is in contrast to runners <40years of age who tend to experience more knee and lower leg injuries such as ITB syndrome, and shin pain (‘shin-splints’). I have observed this to be the case in clinical practice, with the vast majority of master’s runner related injuries affecting tendons or calf musculature.
The increase in below the knee injuries in masters runners may be in part due to the known reduction in leg and achilles tendon stiffness that occurs with ageing. A less stiff achilles tendon will be subjected to elevated achilles tendon strain when generating push off force at toe off, which in turn elevates the risk of achilles tendon disruption and injury. It is known the a 20% decrease in achilles tendon stiffness is observed in individuals with achilles tendinopathy (3). Likewise the risk of calf soft tissue injury is heightened in the masters runner as the achilles tendon in long stiffness becomes more compliant (more ‘sloppy’ in energy storage and release) the calf is required to elongate under load eccentrically.
2. Reduction in ‘calf’ strength with ageing
As we age we lose approximately 30% of plantar flexor strength (1% per year) from 30 years of age onwards. The below image from Dr Rich Willy presented at the 2018 La Trobe University Running Symposium depicts this reduction if force generation and subsequent achilles tendon stiffness that masters runners experience.
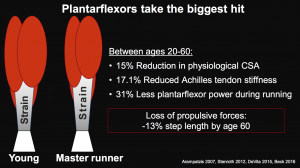
Image source: 2018 Running Symposium, Dr Rich Willy: The Masters Runner: maintaining durability.
The good news for masters runners is despite this known reduction in leg and achilles tendon stiffness the stiffness can be enhanced through specific strength and conditioning exercise. Masters runners with greater plantar flexor (calf) strength, exhibit greater achilles tendon stiffness, which in turn makes calf strengthening work for the masters runner imperative. High calf strength ability appears to be protective against achilles tendinopathy. Runners with greater eccentric plantar-flexor strength have been found to have a reduced risk of developing achilles tendinopathy (3).
3. Running surfaces for masters runners
Many runners mistakenly believe that running on soft surfaces such as grass, or trails as opposed to road or concrete running, is beneficial for reducing associated lower limb loads. However interventions that aim to minimise running on soft surfaces may be important for the masters runner in reducing the risk of achilles tendon and calf injuries (2).
Reducing the time spent running on soft surfaces can seem counter intuitive for not just masters runners, but runners in general. There exists a common belief that soft surfaces must be better for lessening the impact forces a runner experiences.
However, researchers have found that running on sand increased the risk of achilles tendinopathy by a magnitude of 10x in masters runners. This was compared with running on hard/firm surfaces, such as asphalt, which lowered the risk of achilles tendinopathy in masters runners by 53% (4).
4. Running may have a protective effect against the onset of hip and knee osteoarthritis
In contrast to calf and achilles tendon injuries in the masters runner, surprisingly osteoarthritis (OA) is quite rare in the masters runner. This is despite the popular sentiment that running may be ‘bad for the knees’ and the cause of OA onset and subsequent progression’.
Many people assume that walking would be ‘better’ on the joints than running, as the assumption is that the lower ground reaction and subsequent joint forces would be less injurious and ‘damaging’. However, researchers have shown that the cumulative knee joint loading is essentially the same for walking and running (5).
In fact running seems to condition the articular cartilage by promoting chondroprotective, or cartilage enhancing effects (5).
Researchers have found that despite popular opinion, recreational running may have a protective effect against developing hip and knee osteoarthritis compared with non runners (6). Hence it appears safe to advise masters runners that ‘fear not’ running does not seem to increase OA related symptoms or progression or indeed ‘wear out the knees’.
For those masters runners who have known non traumatic osteoarthritis of the knee running has been shown by researchers to not increase symptoms of progression of the OA process (7).
However, it should be noted that the one group in which running was not found to be protective against the onset of knee or hip osteoarthritis was runners who had a long history of high volume/high intensity running. Such runners (akin to elite runners) were found to have equivalent risk of hip and knee OA as sedentary individuals or non-runners (6). In contrast, runners who ran moderate volume or intensity actually had the lowest risk of developing hip or knee OA (6).
In a 2018 published paper researchers found that the rate of hip and knee OA in marathoners was 8.8%, which was much lower than the rate amongst a matched non running group who had a 17.9% rate of hip and knee OA (17.9%) (8).
However despite any potential increase in OA associated with running, running has shown to be effective in preventing at least 35 chronic conditions and treating at least 26 chronic conditions -so masters runners should aim to keep running! (9,10)
For those masters runners who do suffer from knee osteoarthritis quadriceps strengthening exercises have been shown to improve the cartilage quality of the knee in individuals with a past history of knee surgery (11). Other strategies to improve knee OA symptoms may be to alter running cadence (higher cadence may decrease knee joint cumulative loading), or to manage loading through simple strategies such as replacing some running sessions with cross training activities such as swimming or cycling.
A 2019 research study (13) looked to evaluate the short term impact of running long distances (a four month marathon training program followed by a first time marathon) on the health of the knee joints of 82 middle aged runners. Knee MRIs were taken both before (6 months prior to the marathon) and after (2 weeks following the marathon). MR imaging pre the marathon showed signs of ‘damage to several keys structures’ of the knees of the majority of runners in the study-most runners were void of knee pain or symptoms. Following the marathon MR imaging showed improvements to the health of subchondral bone of the tibial (shin bone) and femoral (thigh bone) condyles. The patella cartilage appeared to worsen however remain asymptomatic. The authors concluded that these findings provide ‘the most robust evidence to link marathon running with knee joint health and provides important information for those seeking to understand the link between long distance running and osteoarthritis of the main weight-bearing areas of the knee’.
5.The Physiology of the Masters Runner
In addition to the musculoskeletal changes that occur as a runner enters the masters years, there are also numerous cardiovascular function and therefore endurance performance changes that occur with ageing.
Physiologically as a runner enters the masters years the below changes have been found (13) through studying 55 runners aged between 30 and 80 years who ran on average 50km per week to occur:
- In trained runners V02max decreases by 7% between 30 and 70years of age
- Heart rate max decreased by 3.2% per decade
- Average 10km run time slowed by 6% per decade
- Cardiac output decreased by 5.8% per decade
The researchers concluded that the decline of VO2max with ageing in runners was mainly explained by the central cardiovascular factors represented by the decline of heart rate max and cardiac output.
Willy and Paquette (2) surmise that although running training cannot completely halt the natural and above mentioned age related declines in cardiovascular function, that there is ‘absolutely no doubt that continued endurance training volume and intensity are beneficial to slowing these declines in the masters runner. And with the many known positive health benefits of lifelong running, doing so is key for an ageing runner or individual.
Summary
Maters runners and practitioners can look forward to enjoying and benefiting from lifelong running. Keeping the above considerations in mind will assist in aiding the pursuit of enjoyable and beneficial running beyond the age of 40 years.
Related:
The below resources and links provide further information re masters runners.
1.Masters runners podcast with Dr Rich Willy HERE>>

2. Below are two infographics and their captions that I published to Instagram relating to masters runners:
Infographic 1: 5 Things Masters Runners Should Do

👉🏻While running across the lifespan can help to slow the rate of decline of cardiovascular capacity and strength, as a runner enters the masters years they will experience an inevitable and unavoidable progressive decline physiologically, biomechanically and also performance wise 👟
👉🏻These tips can potentially help to offset some of the changes experienced by the masters runner resulting in a slower rate of change with the passing of time ⏳:
1️⃣ running across the lifespan has been shown to add years to runner’s lifespan compared with non runners
2️⃣ between 20 & 60yrs runners will experience approximately 1/3 reduction in power generated at the calf when running
3️⃣ it’s important to not get stuck in the ‘mid & comfortable running pace’ rut. Running at speed can assist with building tissue tolerance and running body resilience-which may be injury protective (when done with wisdom)
4️⃣ from 20-80yrs 30% of muscle mass is lost- resistance training can help to offset and even reverse this change
5️⃣ Adopting a hard: easy approach can assist with optimising tissue health, thereby assisting with the development of a chronic training base while not being interrupted through injury
TAKE HOME: By adding even just one of the above tips you may assist your masters running (P.S. Still very helpful also for runners sub 40yrs) 👍🏻
Infographic 2: 5 MASTERS RUNNERS FACTS 👟

☝🏻There is a growing number of masters (> 40yrs) runners world-wide 🌎 taking to the sport + also continuing to run for longer. Here are 5 Masters Runners facts as published by Willy & Paquette*👀
1️⃣ The increase in below the knee injuries in masters runners may be in part due to the known reduction in leg and achilles tendon stiffness that occurs with ageing. A less stiff achilles tendon will be subjected to elevated achilles tendon strain when generating push off force at toe off, which in turn elevates the risk of achilles tendon disruption and injury 👣
2️⃣. Researchers have found that running on sand increased the risk of achilles tendinopathy by a magnitude of 10x in masters runners. This was compared with running on hard/firm surfaces, such as asphalt, which lowered the risk of achilles tendinopathy in masters runners by 53%🏖🛣
3️⃣. Researchers have found that despite popular opinion, recreational running may have a protective effect against developing hip and knee osteoarthritis compared with non runners 🦵👍🏻
4️⃣. There is an inevitable and unavoidable progressive decline physiologically associated with reduced cardiovascular function including a reduction in maximal aerobic capacity (V02max) of approx 7% per decade between 30 and 70yrs ⬇️
5️⃣. Statins may increase the risk of tendinopathy, while fluoroquinolone use may slow down achilles tendon rehabilitation due to a reduced rate of collagen synthesis ⏳
🖥*Ref: R. Willy, Paquette, M. (2019). The physiology and biomechanics of the masters runner. J Sports Med Arthrosc Rev 2019, 27: 15-21
👉🏻For some great further tips on masters running jump over to Expert Edition Ep 1️⃣3️⃣2️⃣ of @physicalperformanceshow to learn from @montannarunninglab 💡
TAKE HOME: there are a myriad of health benefits to be had for those who run beyond 40yrs of age. These tips may be of interest and also utility in helping the master runner enjoy injury free running. Remember when it comes to the Masters Runner: ‘below the knee is the key!’

Brad Beer (APAM)
APA Titled Sports & Exercise Physiotherapist (APAM)
B.Physio/ B. Ex. Sc
Author ‘You CAN Run Pain Free!’
Founder POGO Physio
Host The Physical Performance Show
Featured in the Top 50 Physical Therapy Blog
References:
(1) Lepers R, Cattagni T. Do older athletes reach limits in their performance during marathon running? Age (Dordr). 2012; 34: 773-781.
(2) R. Willy, Paquette, M. (2019). The physiology and biomechanics of the masters runner. J Sports Med Arthrosc Rev 2019, 27: 15-21
(3) Ayra S, Kulig K. Tendinopathy alters mechanical and material properties of the Achilles tendon. J Appl Physiol. 2009; 108:670-675.
(4) Knobloch K, Yoon U, Vogt PM. Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int. 2008; 29: 671-676.
(5) Miller RH. Joint loading in runners does not initiate knee osteoarthritis. Exerc Sport Sci Rev. 2017; 45: 87-95.
(6) Alentorn-Geli, E., et al., The Association of Recreational and Competitive Running With Hip and Knee Osteoarthritis: A Systematic Review and Meta-analysis. J Orthop Sports Phys Ther, 2017. 47(6): p. 373-390
(7) Lo GH, Musa SM, Driban JB, et al. Running does not increase symptoms or structural progression in people with knee osteoarthritis: data from the osteoarthritis initiative. Clin Rheumatol. 2018. [Epub ahead of print]
(8) Ponzio DY, Syed UAM. Purcell K, et al. Low prevalence of hip and knee arthritis in active marathon runners. J Bone Joint Surg AM. 2018; 100: 131-137.
(9) Skou, S.T., et al., Physical Activity and Exercise Therapy Benefit More Than Just Symptoms and Impairments in People With Hip and Knee Osteoarthritis. J Orthop Sports Phys Ther, 2018. 48(6): p. 439-447.
(10) Lee, D.C., et al., Running as a Key Lifestyle Medicine for Longevity. Prog Cardiovasc Dis, 2017. 60(1): p. 45-55.
(11) Roos EM, Dahlberg L. Positive effects of moderate exercise on gylcosaminoglycan content in knee cartilage: a four month, randomised, controlled trial in patients at risk of osteoarthritis. Arthritis Rheum. 2005; 52: 3507-3514.
(12), et al. Can marathon running improve knee damage of middle-aged adults? A prospective cohort study.
(13) Fuchi T, Iwaoka K, Higuch M et al. Cardiovascular changes associated with decreased aerobic capacity and aging in long distance runners. Eur J Appl Physiol Occup Physiol. 1989; 58: 884






Great article Brad. Easy to understand & very relevant.