Background on Cycling Injuries

Cycling participation has surged in the wake of the global pandemic1. With more people working from home, and indoor training platforms such as Zwift becoming more accessible, there has never been a better time to saddle up. As such, we have seen dramatic increases in cyclists on the road, trails and over virtual platforms. Unfortunately, this has come with a rise in injuries associated with the sport2.
Cycling injuries present as either: acute (from a single traumatic event) or overuse (as a result of repetitive tissue loading). Whilst there is very clear epidemiological data on acute injuries, the research is somewhat lacking when it comes to overuse cycling injuries. There is likely under-reporting of overuse injuries3 as they rarely force cyclists to completely stop riding (and therefore be counted towards time-loss or medical treatment injuries). Dahlquist et al (2015) found that two-thirds of recreational cyclists continue to ride despite experiencing high levels of pain4. A review by Clarsen and Visentini found that overuse injuries represent 50-60% of cycling injury presentations3.
Patellofemoral pain has been identified as the most common overuse injury in cyclists of all abilities5, and is attributed to the greatest loss of time from training in professionals6. There is also a high prevalence of lower back (lumbar) pain in both professional6 and recreational cyclists7, which can limit both performance and enjoyment. This blog will later highlight other common overuse injuries experienced by cyclists and their potential causes.
Superficial soft tissue injuries such as skin abrasions, lacerations and muscle contusions make up the majority of acute cycling related injuries5. Traumatic fractures and head injuries account for approximately 5-15% of injuries according to a systematic review by Rooney et al5. They found that acute injuries most commonly affect the upper limb, with the clavicle being the most prevalent fracture. The nature of these acute traumatic injuries makes them hard to prevent, with protective equipment and sensible riding key to minimising risk.
What causes overuse injuries in cycling?
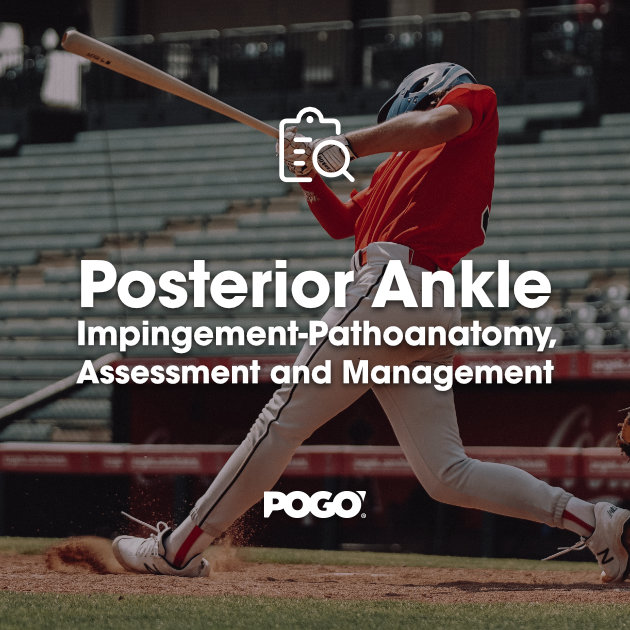
Training load, bike set up and tissue capacity are 3 key considerations when it comes to overuse injuries in cycling. Fortunately, most overuse injuries can be managed and prevented by addressing these aspects. Technique, equipment choice, and anatomical differences are also important factors to consider, but to a lesser degree.
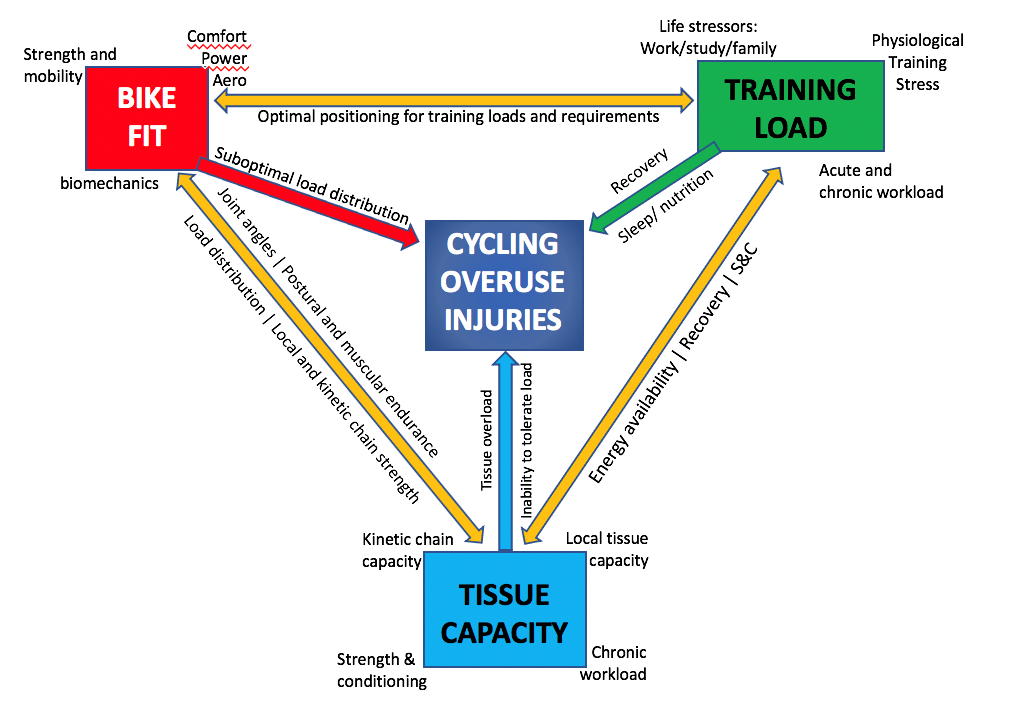
Image 1: In this blog series we will delve into the multifactorial and interrelated nature of cycling related overuse injuries.
Tissue capacity
By nature, cycling is a highly repetitive uniplanar sport involving sustained static postures over prolonged periods of time. This places large cumulative loads on certain structures, which can become sensitive without adequate strength or tissue capacity.
Put simply; our soft tissues (i.e., tendons, muscles, ligaments, cartilage and joint capsules) and hard tissue (bone) need to withstand the loads placed on them during exercise. Soft tissue and bone are dynamic structures, meaning they constantly adapt to the loads they’re subjected to.
Chronic underloading causes a gradual decline in tissue and physiological qualities such as fitness and strength. Overloading above the body’s capacity without sufficient recovery will have a catabolic effect, breaking down tissue and causing injury.
To improve capacity, our tissues need to be loaded enough to provide the necessary level of stimulus for adaptation, but not so much that it exceeds that tissue’s tolerance. It is important to note that it is during the recovery process that the body adapts and becomes stronger, not training in isolation. In other words, optimal loading requires a fine balance between sufficient tissue stress and adequate recovery.
When considering any overuse injury, it is critical to evaluate the tissue capacity of the entire kinetic chain- not just the injured site. This is important because ‘weak links’ further up or down the chain can cause excessive loading on other structures. For example, having weak glutes to assist with extension during the power stroke may increase loading on the quadriceps muscle and patellofemoral joint- resulting in anterior knee pain.
Strength and conditioning programs focused on heavy resistance training (i.e. weights) is the most effective way for cyclists to improve tissue capacity. Specific focus on quadriceps, gluteal, calf and hamstring muscles will not only reduce the risk of lower limb injuries but also improve performance8,9,10. It is easy for cyclists to neglect core and upper body work in the gym, however, adequate strength of these regions is necessary to sustain prolonged postures and keep the rider stable on the bike. This helps minimise unnecessary movements and improves efficiency, leading to better performance. A detailed gym strengthening program for cyclists is outlined at the end of this blog.
The other way to improve tissue capacity is by progressing training volumes appropriately, leading us to training load and error.
Training load
Training load is a critical factor in the prevention and management of all sporting overuse-related injuries, not just cycling or endurance events. So, what is training load and how is it calculated?
Training load is the dosage or stimulus produced by a workout/ride. For cyclists, it encompasses more than just mileage, duration or even power. These metrics are classified as external loads and do not capture the relative physiological stress imposed on the cyclist (internal loads). There are a growing number of ways to determine internal loads, especially with recent technological advancements and accessibility. Examples include heart rate (as a % of maximal HR or HR reserve), lactate concentrations, training impulse (TRIMP- based on HR x duration) and heart rate variability (measured at rest or after exercise). Perhaps the simplest and most valuable indicator of internal load is the rating of perceived exertion (RPE) multiplied by minutes to provide an ‘arbitrary unit’ (AU). This is analogous to ‘exertional minutes’ and has been shown to have strong correlation with seemingly more complicated and technologically advanced methods11,12.
Tracking workload with AU as a function of RPE x minutes is superior to using just speed, distance, or power. This is because it better reflects how hard a rider is working and their current state of fatigue and fitness. For example, a 60-minute hour hilly time trial on a hot humid and windy day after 3 days of racing prior and poor sleep leading up to the event may be calculated as 9.5/10 RPE x 60minutes = 570AU. In comparison, a 2hour social coffee ride on flat roads, cool calm conditions, fresh legs and a good night’s sleep may be calculated as 4/10RPE x 120minutes = 480AU.
Therefore, cyclists must take into account the following factors when planning training, and adjust workouts accordingly:
Internal factors: sleep quality and quantity, work/academic/family stress, sickness, hormonal status, nutrition before, during and after workouts/rides, energy availability, muscle fatigue from previous training, and the effect of certain medications.
External factors: temperature, humidity, course elevation, altitude, wind, riding in a group slipstream vs solo, and equipment choice (i.e., using a TT bike vs road bike).
As you can see, the above considerations can significantly influence the true physiological workload of any ride or workout, even if they are identical in distance or duration. Even psychological and emotional stressors can affect the body’s ability to train.
By limiting the number of changing training variables we change at a time, we can reduce the risk of injury. For example, simultaneous increases in hill climbing, mileage and racing in the same week is likely to cause tissue overloading and potential injury. Similarly, maintaining the same training volume and intensity, but with the flu, life stress and minimal sleep is going to impair recovery processes that facilitate adaptation.
Other training errors that are quite easy to discount include too much training in very high gear ratios (overgearing), spending more time on a stationary trainer (especially in this era), and off the bike “brick” sessions (for triathletes).
How can cyclists practically use training load data to minimise the risk of injury?
Online training platforms such as Strava and Training Peaks (TP) use specific algorithms to calculate a “Suffer Score” or “Training Stress Score” based on heart rate and power data respectively. Recommendations to increase, reduce or hold steady on training are made using this data in relation to previous training sessions and their relative effort.
A simple and objective way to do this without technology is using the Acute: Chronic workload ratio (ACWR). As the name suggests, it calculates the ratio between acute training load (over the last 7 days) and chronic workload (in the previous 28 days). Training load is described in arbitrary units (AU) as a product of RPE and session duration. Gabbett et al13 found that a ratio of 0.8-1.3 is the sweet spot for training, with ratios above 1.5 correlated with greater injury risk. Ensuring that ACWR is kept in the sweet spot will help cyclist avoid large spikes in load that may lead to a ‘boom-bust’ cycle of injury, leading to progressively worsening performance and reduced training loads.
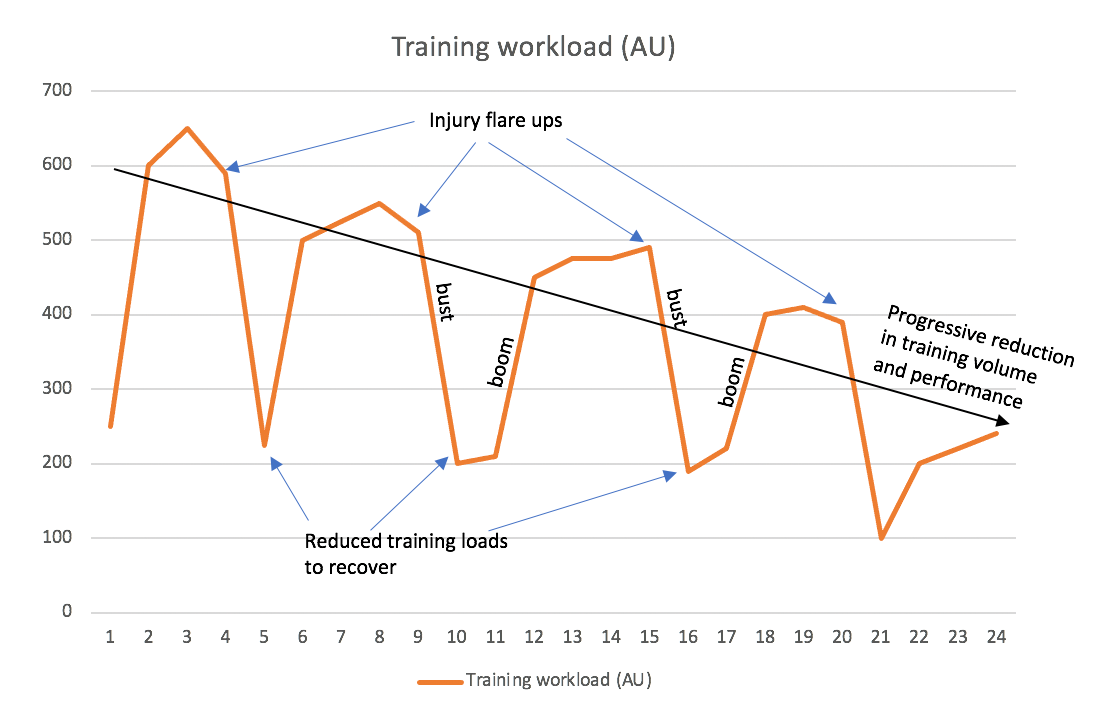
Image 2: Boom bust cycle: very rapid increases in training volume over short periods of time (booms in acute workload) are followed by injury (represented by decreases in training volumes). It is evident that the long term ‘chronic’ trend is a gradual decline in training volume and consequently performance.
The rule of too’s: outlines how too much (time and distance on the bike), too often (frequency of riding), too hard (intensity) and too soon (without adequate tissue capacity) does not give the body enough time to adapt to training stresses.
However, this does not mean that we should fear large training volumes. A 2016 review by Gabbett14 titled “The training-injury prevention paradox- should athletes be training harder and smarter?” outlines why reducing training volumes is not necessarily the best approach for preventing injuries.
The research is clear that greater training volumes are associated with improved performance in individual endurance sports such as cycling15. Though the evidence suggests that there is a dose-response relationship between greater workloads and higher injury risk16, it is also known that lower training loads are not only associated with increased injury risk13, but limits performance potential.
Gabbett found that higher chronic workloads are actually protective against injury, leading to the concept that training harder may in fact be training smarter. Cyclists accustomed to greater workloads are better prepared to handle relative ‘spikes’ in training loads compared to those training at much lower volumes. Using ACWR and the principles surrounding high chronic workloads, we can predict and pay special attention to when cyclists are most likely to get injured during their season:
i) Early in the preseason- where cyclists may over-enthusiastically ramp up their base build phase after a few weeks off.
ii) After a period of time off the bike- due to injury, illness or other commitments.
iii) The latter stages of the competition season where cyclists are racing frequently at higher intensities in a fatigued state.
In summary, training load is a critical factor in cycling injuries. If you don’t manage and progress workload appropriately, injury is inevitable, no matter how good your bike set up or physical capacity is. Therefore, the key takeaways of this section are:
- Training load is not simply a product of weekly mileage, power output or duration of training. It is influenced by external factors (such as environmental conditions) and internal factors (such as our state of health), which affects the true training stress of each session.
- Only change one training variable at a time.
- Monitor your training workloads, using more than just time and distance. Consider using ACWR or training apps.
- Progress training slowly and listen to your body. The 10% can be used as a guideline, but may prove too big of a ‘jump’ for those with already high training volumes. Schedule recovery days and deload weeks throughout the season.
- Strength and conditioning focusing on improving tissue capacity will help cyclists tolerate relative increases in workloads.
- Greater training volumes are protective against injury and beneficial for performance- the key is getting there safely!
Bike fit
Phil Burt, expert bike fitter and expert edition guest on episode #242, explains how there is no one ideal bike fit position, but rather a ‘bike fit window’. Bike fit involves finely balancing the 3 following variables: i) Power, ii) Aerodynamics, and iii) Comfort. Optimising one aspect, for example, improving aerodynamic profile will affect the other variables, e.g. reducing comfort/sustainability and power output. On the other hand, maximising comfort on the bike will come at the expense of aerodynamics. Therefore, a compromise must be met between these 3 variables.
Phil also explains how bike position is infinitely adjustable, however, the rider can only adapt within their anthropometric limits. He also outlined how some riders can absorb large changes in bike position (macro-absorbers), and that small changes can create a big difference for others (micro-adjusters). Bike fit is a dynamic process, and must be highly individualised to suit the rider’s needs and changing characteristics over time. For example, younger or more experienced riders may be able to tolerate more aggressive positions. On the other hand, older, injured, or less experienced riders may require a more relaxed fit. Bike fit for triathletes will focus on optimising aerodynamics and power, without impeding running performance.
Let’s take a closer look at the specifics behind a bike fit…
The rider’s bodyweight is distributed between 3 main contact points on the bike: the interface between feet/cleats on pedals, pelvis on the saddle and hands on the hoods. Adjustment of certain elements such as saddle, handlebar and cleat position can alter pressure distribution between the 3 contact points, and also load distribution through the kinetic chain. This may manifest as an overuse injury when coupled with inadequate tissue capacity, training errors and inadequate mobility.
Bike fit parameters:
Saddle position
Suboptimal saddle position is associated with a broad range of overuse related cycling injuries. Parameters such as height, setback and tilt have implications on the entire kinetic chain as well as weight distribution between the 3 interfaces. Fortunately, it is the easiest adjustment to make on the bike, and can yield significant performance and comfort benefits.
Saddle height
Saddle height determines hip and knee flexion/extension angles throughout the pedal stroke. A saddle that is too high will result in excessive pelvic lateral shifting or ‘rocking’ side to side in an attempt to reach the pedals in the 6-o’clock position. Relative ‘over-extension’ of the knee will result in loss of power at the very bottom of the pedal stroke and contribute to a variety of overuse injuries, which are outlined in the table at the end of this section.
On the contrary, a saddle that is too low will cause greater hip and knee flexion throughout the pedal stroke, also resulting in loss of power. Increased knee flexion during the power phase is thought to increase compressive loading at the patellofemoral joint17, with past research suggesting an inverse relationship between saddle height and patellofemoral compressive forces17. Although this is yet to be confirmed in more recent studies, common practice recommends increasing saddle height so that maximal knee extension is between 30-35 degrees in those with anterior knee pain18. By increasing provocative hip flexion angles, low saddle height can also be implicated in anterior hip pain, especially in those with hip joint pathology such as FAI. Low saddle height combined with poor pedal technique (excessive heel drop) can increase the risk of Achilles related problems such as tendinopathy and paratenonitis.
Saddle setback
Saddle setback (or fore-aft) refers to the horizontal distance between the tip of the saddle in relation to the bottom bracket. Adjusting setback will influence hip and knee joint angles, muscle engagement and weight distribution on the bike. This makes it an importance bike fit consideration to improve comfort, control, pedal efficiency, and injury risk.
A saddle that is pushed too far backwards may result in the rider ‘over-reaching’ for the handlebars, increasing demands on the core, lower back and upper body to keep the rider stable. This extra energy comes at a cost to performance and comfort.
Greater hip flexion angles at the top of the pedal stroke (12-o’clock position) will increase proximal hamstring and gluteal tendon compression, and may be implicated in hip impingement. Greater setback can also increase pressure on the perineum, leading to saddle sores and numbness. More often than not, riders will benefit from shifting their saddle further forward. Doing this will help open up the hips and engage the gluteal and quadriceps muscles, improving power.
Saddle tilt
Saddle tilt refers to the angulation of the saddle up or down. The current UCI (world governing body for sports cycling) rules state that saddles should have no greater than 9-degrees of tilt. As a general rule, saddles should be positioned horizontal, (i.e. level with the ground) however, evidence shows that a slight downward tilt can help alleviate perineal pressure19. For those with back pain, angling the saddle approximately 1-2 degrees downwards will position the pelvis in a slight anterior pelvic tilt, promoting even distribution
of flexion throughout the spine. An upwards tilt (i.e., the nose higher than the back) will posteriorly tilt the pelvis, forcing the lower back into greater flexion and increase perineal pressure.
Saddle shape and design
There are a large range of saddle shapes and designs available these days: from varying degrees of padding, cut out or gap designs, different widths and nose lengths. Whilst the research is not unanimous on the ‘best saddle design’, there are a few things we know for certain. The anatomy of every cyclist is unique, so trialling different saddles before committing to one is highly recommended. Naturally, females have wider hips, and therefore should consider wider saddles to accommodate anatomical differences. On the other hand, men that experience penile numbness should consider using a gap saddle to alleviate pressure. Saddle design can also be an important factor in different performance situations. Due to the aggressive anteriorly rotated pelvic position when riding a TT bike, pressure will be distributed further forward onto the pubic rami (compared to the ischial tuberosities ‘sit bones’ in road cycling). A triathlon specific saddle with a clipped nose will accommodate for this position, and often have an anti-slip cover to improve stability. Road racers may find that a saddle with a longer nose will provide greater stability.
It may be surprising to some that highly padded seats do not necessarily reduce perineal pressures. In fact, a 2002 study20has shown that increasing saddle width is more effective at reducing perineal pressures than increasing cushioning because they are able to distribute pressures more evenly.

Image 3: Saddles come in a variety of shapes, sizes and padding to accommodate for different anatomy and types of riding (i.e. triathlon, commuting, racing). It is recommended that you trial a variety of saddles until you find one that suits you.
Reach and drop
Reach and drop are important considerations that influence aerodynamics, comfort and handling ability.
Reach can be defined by the distance a cyclist must extend forward (horizontal displacement) to meet the handlebars. It is a product of saddle setback and stem length. Drop determines how low a cyclist must come down (vertical displacement) to meet the handlebars. This is determined by saddle height and headset spacing. Effective reach and drop will increase when riding on the drop bars on a road bike.
Greater reach and drop will force cyclists into more aerodynamic positions by minimising frontal surface area profile. However, riding in these aggressive positions requires adequate flexibility and strength. Due to greater hip and trunk flexion, proximal hamstring and gluteal tendons are subject to increased compression and loading, increasing the risk of tendinopathy. Getting lower on the bike is only faster to a point- breathing and power output are likely to become compromised with greater hip and trunk angles. Hip impingement may occur at the top of the pedal stroke, and supporting trunk and upper body muscles will have to work significantly harder to stabilise. Shifting weight further forward towards the handlebars can lead to excessive pressure on the hands and wrists, causing nerve compression of the median and ulnar nerves. Reducing drop and reach to improve comfort and control can be achieved using headset spacers or finding a shorter (or more angled) stem.
Handlebar positioning
Handlebar position can be adjusted in many ways to either maximise comfort and control or facilitate a more aerodynamic position. Slight backwards rotation of the handlebars can assist in achieving a more neutral wrist alignment for cyclists suffering wrist pain or hand numbness. Similarly, brake and shifter levers can be adjusted to minimise excessive radial or ulnar deviation (lateral wrist movements) which can further offload wrist and hand structures.
Hand placement should be at least shoulder width apart as a general guide, as any narrow will compromise control and stability (time-trial bars are an exception due to the main objective being speed).
Crank length
Crank length is a contentious topic with the old school of thought being that longer cranks provide greater leverage and therefore more torque. However, research challenges this notion, indicating that crank length has a negligible effect on power in submaximal cycling21. Swaying towards slightly shorter cranks may be a more appropriate choice from an injury and performance perspective. Effectively, it reduces hip and knee flexion angles at the top of the pedal stroke and naturally increases cadence. This makes it an ideal option for those experiencing anterior knee pain. Opening the hips up at the top of the stroke will confer greater power, reduce hip impingement and improve runs off the bike.
Cleat/shoe
An often-overlooked element in both cycling injury research and bike-fit is the foot-pedal interface. This is the direct site of energy transfer from the cyclist to the drivetrain. Forces generated by the hip, knee and ankle are directly transmitted to the bike via a very small contact area (the size of your cleat if riding clipless). As a result, the forefoot is subject to very large and sustained pressures being the only site of energy transfer. A 2012 Australian study involving 397 cyclists identified foot pain in 53.9% of respondents, with the forefoot region most likely to be affected22.
The interface has evolved from the simple flat pedal, to cages and toe straps, and now clipless systems. Research has indicated that riding with these attached foot-pedal interfaces more than doubles the incidence of experiencing foot pain22.
The introduction of carbon fibre shoes to improve stiffness and power transfer has also been shown to increase peak plantar pressures23. Simple adjustments such as pushing the cleat backwards or use of orthoses can help redistribute pressure away from the forefoot to alleviate pain.
Cleat position is an important consideration in clipless systems that ‘fix’ the shoe into position on the pedal. Cleats can be moved forwards, backwards, sideways and rotated to accommodate anatomical variation, riding style and personal preference.
Most people have some degree of tibial or femoral torsion (twisting of the leg bones) which influences how much we naturally toe-in or toe-out. It is important that cleats are orientated at an angle that accounts for this variation, so that the knee joint can function in its natural plane of motion. Riding with feet toed-in or -out further than one’s anatomical limitations can cause additional strain on structures on lateral and medial knee structures respectively. Nowadays, many brands have cleats that allow a few degrees of rotational play known as ‘float’. This can help minimise torsion forces transmitted at the foot-pedal interface, reducing strain up the kinetic chain.
Cleats can also be pushed forwards or backwards on the shoe. Having the cleat positioned further forward will increase work required by calf musculature due to greater leverage. It will also reduce foot stability on the pedal and increase pressure on the forefoot. A shift towards more midfoot-cleat positioning has been advocated due to a reduction in calf work and greater contribution of quadriceps, hamstring and gluteal muscles. Practically, mid-foot pedalling may be an appropriate option for cyclists with forefoot related pain (examples include sesamoiditis and intermetatarsal bursitis), or triathletes looking for a faster run off the bike.
Narrow cycling shoes are a common cause of forefoot pain due to compression of interdigital structures (such as nerves, blood vessels and bursa), which can lead to pins, needles and numbness.
Image 3: Bike fit parameters
Summary:
As alluded to earlier, there is no ‘perfect’ bike fit position, but rather a ‘window of fit’ in which riders can tolerate. This window varies from cyclist to cyclist, with some being able to absorb large changes in the above parameters without any issues, and others unable tolerate slight adjustments. Therefore, cyclists should experiment with different positions and feel what works best for them. There are no set recipes as every cyclist is unique and will have various requirements and goals to achieve from a bike fit (e.g. a fit focused on comfort and sustainability vs a competitive racer wanting to maximise power and gain an aerodynamic advantage). Today, bike fitters use a variety of approaches, or a combination of different bike fit methods.
Formula based approaches use anthropometric data such as limb length to determine fit parameters. This quick and easy approach allows people to fit themselves at home, however, does not take into account individual factors such as joint mobility, strength and pedalling technique. Other approaches involve using the rider’s joint angles to guide bike fit parameters. The static angle approach involves using goniometers (large protractors) to measure joint angles (e.g. knee angle) at certain points of the pedal stroke. Bike position is adjusted so that joint angles at these points fall within ‘acceptable’ ranges. Although this method may be a provide an adequate start point for most, expecting that the same angle ranges will suit every cyclist is unreasonable. This is especially the case for ‘micro-adjusters’ who may benefit from further tweaking using more technical approaches.
The dynamic approach utilises motion capture technology to measure joint angles and movement throughout the entire pedal stroke. This is a big advantage over the static approach as it accounts for pedal technique and can pick up intricacies such as frontal plane knee motion (lateral knee movements) associated with greater risk of injury.
Bike fit has come a long way and now modern methods incorporate scores of data ranging from saddle pressure and power distribution to guide bike fit parameters. However, with little research available on how to apply this data, bike fit remains to be dually an art and science.
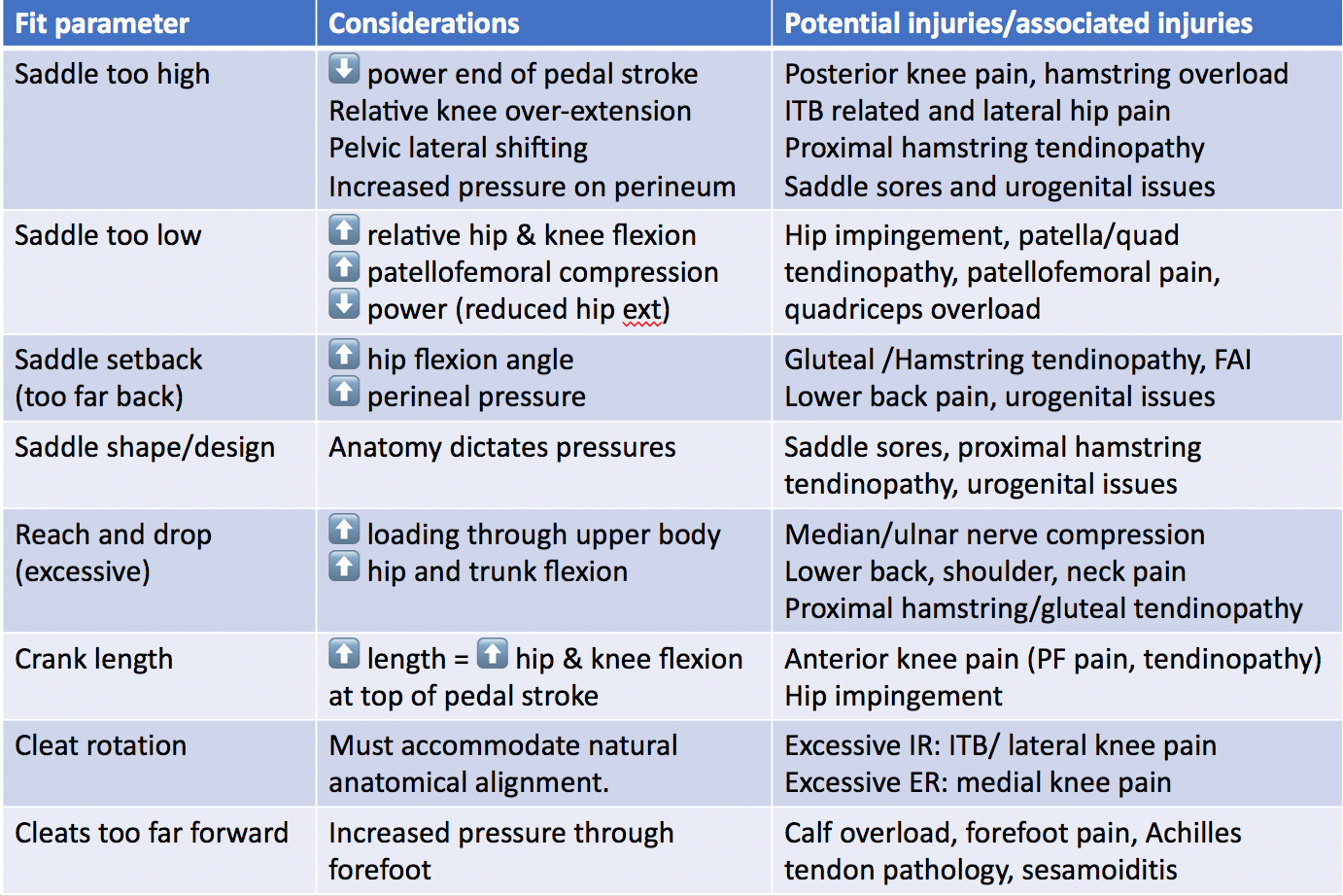
Image 4: Common bike fit injury considerations

Julian Tubman (APAM)
Physiotherapist
Featured in the Top 50 Physical Therapy Blog
References:
- Fuller, G., McGuinness, K., Waitt, G., Buchana, I., and Lea, T. (2021) The reactivated bike: Self-reported cycling activity during the 2020 COVID-19 pandemic in Australia. Transportation Research Interdisciplinary Perspectives. Vol 10, 100377.
- Monash University Accident Research Centre (2020) Injuries during the COVID-19 pandemic. Monthly Bulletin – Edition 8. Victoria. Monash University
- Clarsen, B., Visentini, P. (2016) Overuse injuries in cycling. Aspetar Sports Medicine Journal. Pages 486-492
- Dahlquist, M., Leisz, M.C., Finkelstein, M. (2015) The club level road cyclist: injury, pain and performance. Clinical Journal of Sports Medicine Vol 25 pages 88-94
- Rooney, D., Sarriegui, I., Heron, N. (2020) ‘As easy as riding a bike’: a systematic review of injuries and illness in road cycling. BMJ Open Sport and Exercise Medicine. E000840. Doi:10.1136/bmjsem-2020-000840
- Clarsen, B., Krosshaug, T., Bahr, R. (2010) Overuse injuries in professional road cyclists. American Journal of Sports Medicine. Vol 38 pages 2494-2501
- Wilber, C.A., Holland, G.J., Madison, R.E., Loy, S.F. (1995) An epidemiological analysis of overuse injuries among recreational cyclists. International journal of Sports Medicine. Vol 16, Pages 201-206.
- Sunde, A., Storen, O., Bjerkaas, M., Larsen, M.H., Hoff, J, Helgerud, J. (2010) Maximal strength training improves cycling economy in competitive cyclists. Journal of Strength and Conditioning Research. Vol 24 (8), pages 2157-2165
- Ronnestad, B.R., Hansen, J., Hollan, I., Ellefsen, S. (2014) Strength training improves performance and pedalling characteristics in elite cyclists. Scandinavian Journal of Medicine & Science in Sports. 25: e89-e98
- Vikmoen, , Rønnestad, B.R. (2021) A Comparison of the Effect of Strength Training on Cycling Performance between Men and Women. Journal of Functional Morphology and Kinesiology. 6(1):29.
- Zinoubi, B., Zbidi, S., Vandewalle, H., Chamari, K., & Driss, T. (2018). Relationships between rating of perceived exertion, heart rate and blood lactate during continuous and alternated-intensity cycling exercises.Biology of sport, 35(1), 29–37. https://doi.org/10.5114/biolsport.2018.70749
- Haddad, M., Stylianides, G., Djaoui, L., Dellal, A., & Chamari, K. (2017). Session-RPE Method for Training Load Monitoring: Validity, Ecological Usefulness, and Influencing Factors. Frontiers in neuroscience, Vol 11, page 612.
- Blanch, P., Gabbett, T,J. (2016) Has the athlete trained enough to return to play safely? The acute:chronic workload ratio permits clinicians to quantify a player’s risk of subsequent injury. British Journal of Sports Medicine. Vol 50(8) pages 471-5.
- Gabbett, T.J. (2016) The training-injury prevention paradox: should athletes be training smarter and harder? British Journal of Sports Medicine. Vol. 50(5) pages 273-80.
- Foster, C., Daines, E., Hector, L., Snyder, A.C., Welsh, R. (1996) Athletic performance in relation to training load. Wisconsin Medical Journal. Vol 95(6) pages 370-4
- Foster, C. Monitoring training in athletes with reference to overtraining syndrome. (1998) Med Sci Sports Ex Vol 30 pages 1164-8
- Bini, R., Hume, P.A., Croft, J.L.(2011) Effects of bicycle saddle height on knee injury risk and cycling performance. Sports Med. Vol 41(6) pages 463-76.
- Brukner, P., Khan, K., with Burt, P and Clarsen, B. (2012). Brukner and Khan’s Clinical Sports Medicine, from Biomechanical aspects of injury in specific sports. Sydney. McGraw Hill.
- Spears, I.R., Cummins, N.K., Brenchley, Z., Donohue, C., Turnbull, C., Burton, S., Macho, G.A. (2003) The effect of saddle design on stresses in the perineum during cycling. Med Sci Sports Exerc Vol 35(9) pages 1620-5.
- Schwarzer, U., Sommer, F., Klotz, T., Cremer, C., Engelmann, U. (2002) Cycling and penile oxygen pressure: the type of saddle matters. Eur Urol. Vol 41(2) pages 139-43
- Barratt, P.R., Martin, J.C., Elmer, S.J., Korff, T. (2016) Effects of Pedal Speed and Crank Length on Pedaling Mechanics during Submaximal Cycling. Med Sci Sports Exerc. Vol 48(4) pages705-13
- Uden, H., Jones, S., & Grimmer, K. (2012). Foot Pain and Cycling: a survey of frequency, type, location, associations and amelioration of foot pain. Journal of Science and Cycling, Vol 1(2), pages 28-34.
- Jarboe, N. E., & Quesada, P. M. (2003). The Effects of Cycling Shoe Stiffness on Forefoot Pressure. Foot & Ankle International, 24(10), 784–788.