Tennis Elbow Series (Part 1): Diagnosis and management options

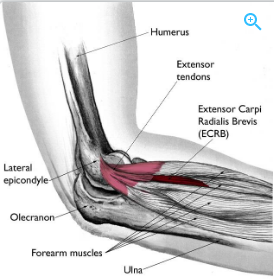
Lateral epicondylitis (LE), also known as tennis elbow or lateral elbow tendinopathy, affects 1-3% of the population. LE is an overuse injury and occurs usually do to an overload of the wrist extensor muscles. These muscles have a common origin (attachment) which is the lateral epicondyle (the bony prominence on the outside of the elbow). Due to the overload of muscles, the bony prominence becomes inflamed and sore. This can then cause further pain down into the wrist extensor muscles or can stay locally on the outside of the elbow. LE can also be caused by trauma. For instance, if you knock your elbow on a doorway with some force, this can trigger inflammation around the tendon origin and cause the onset of the condition.
It is important, however, to screen the neck as well via the ulnar, radial and median nerve tension tests. Issues with the neck and/or nerves can be perceived as LE due to the location of symptoms and determining which structure is at fault is vital for accurate treatment.
Symptoms of LE:
- Reduced grip strength
- Pain on resisted wrist and/or finger extension
- Painful turning or twisting of forearm/wrist particularly when gripping an object
- Tender to touch over outside of elbow
- Perception of “tight” forearm (wrist extensors)
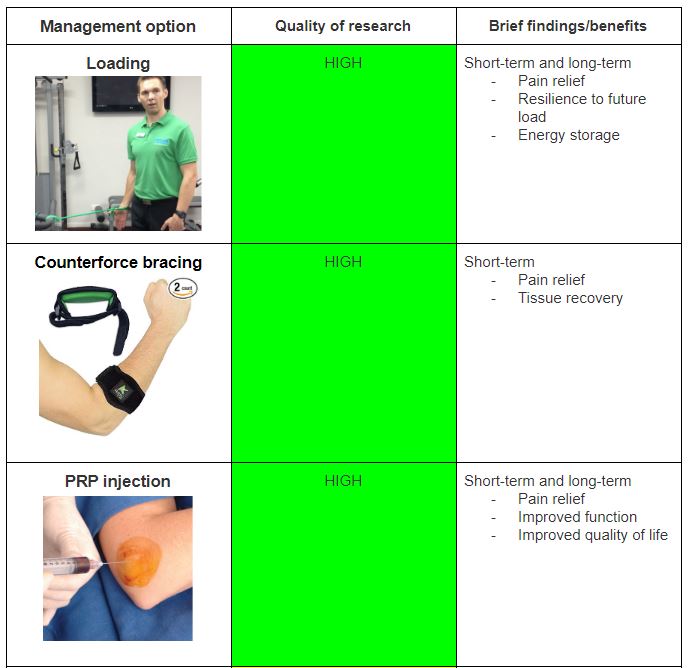
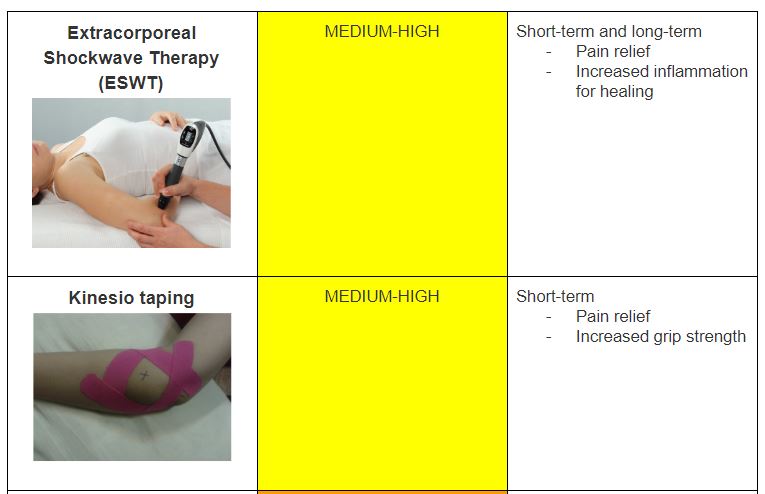
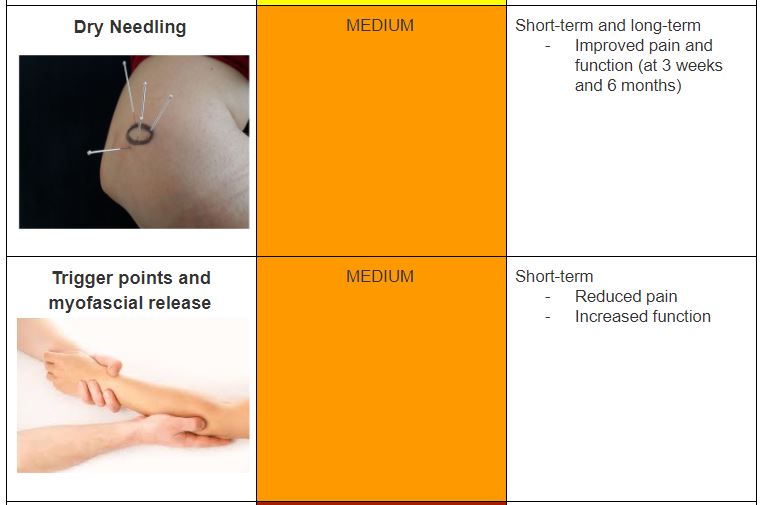
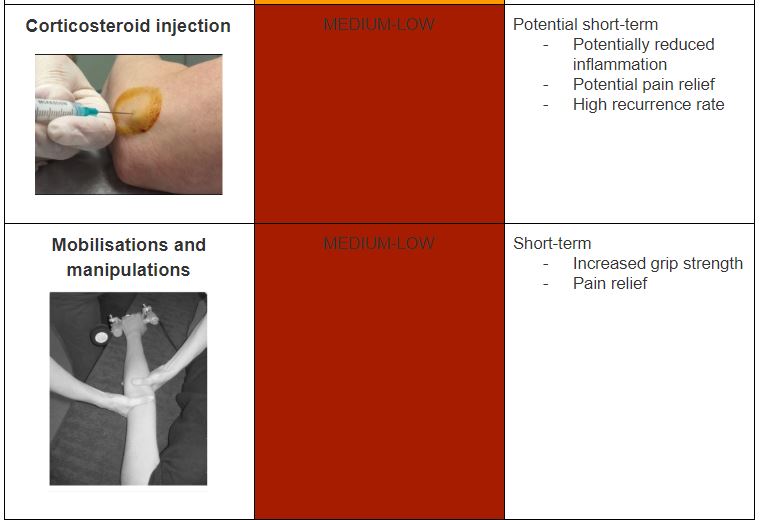
Management options (SUMMARY TABLE)
While the diagnosis of lateral epicondylitis is rather straightforward – management and prognosis is more challenging for clinicians and their clients. The table below is a summary of LE management options, the quality of research behind it and brief findings from the research. For more information on the type of treatments available for LE as well as the method and results the research has found – refer to part 2 of the LE series.
Main message: “Start loading your elbow”
The most important ingredient in the recipe of managing LE is a progressive loading program. Due to the condition being a tendinopathy, and not an acute tear, the only way to return the injured tendon to normal function is through applying a load to it and progressing it as pain and strength allows. A loading program alone is rarely delivered as a treatment protocol in the management of LE. Strengthening exercises are also used in combination with a range of physiotherapy modalities namely soft tissue releases, rock-taping, bracing and extracorporeal shockwave therapy (ESWT). These modalities will be touched on further in part 2.
Loading program
A good exercise to being the loading program for this condition is via an isometric hold against a theraband. Starting at 5 x 20 second holds and progressing via longer holds, increasing tension on the theraband or increasing the theraband strength if not at the highest level. The video below demonstrates this exercise: How to Treat Tennis Elbow Pain: Exercise-Isometrics
The second exercise useful for improving pain and function for those with LE is dumbbell hammers. This activates the wrist extensor muscles eccentrically and is effective at progressing strength of these affected muscles.

Alec Lablache POGO Physiotherapist
Featured in the Top 50 Physical Therapy Blog
References
- Cho, Y., Hsu, W., Lin, L., & Lin, Y. (2018). Kinesio taping reduces elbow pain during resisted wrist extension in patients with chronic lateral epicondylitis: A randomized, double-blinded, cross-over study. BMC Musculoskeletal Disorders, 19(1), 193-193. doi:10.1186/s12891-018-2118-3
- Dimitrios, S. (2016). Lateral elbow tendinopathy: Evidence of physiotherapy management.World Journal of Orthopedics, 7(8), 463-466. doi:10.5312/wjo.v7.i8.463
- Dobreci, D., & Dobrescu, T. (2014). The effects of extracorporeal shockwave therapy (ESWT) in treating lateral epicondylitis in people between 40 and 50 years old. Procedia – Social and Behavioral Sciences, 137, 32-36. doi:10.1016/j.sbspro.2014.05.248
- Gialanella, B., & Prometti, P. (2011). Effects of corticosteroids injection in rotator cuff tears. Pain Medicine, 12(10), 1559-1565. doi:10.1111/j.1526-4637.2011.01238.x
- Khattab, E. M., & Abowarda, M. H. (2017). Role of ultrasound guided platelet-rich plasma (PRP) injection in treatment of lateral epicondylitis. The Egyptian Journal of Radiology and Nuclear Medicine, 48(2), 403-413. doi:10.1016/j.ejrnm.2017.03.002
- Kim, J. Y., & Kim, S. Y. (2016). Effects of kinesio tape compared with non-elastic tape on hand grip strength. Journal of Physical Therapy Science, 28(5), 1565-1568. doi:10.1589/jpts.28.1565
- Kroslak, M., Pirapakaran, K., & Murrell, G. A. (2019). Counterforce bracing of lateral epicondylitis: A prospective, randomised, double blinded, placebo controlled clinical trial. Journal of Shoulder and Elbow Surgery, 28(8), e286-e287. doi:10.1016/j.jse.2019.04.030
- Malliaras, P. (2016). What is the best way to load a pathological tendon. Tendinopathy Rehabilitation. Retrieved from: https://www.tendinopathyrehab.com/blog/tendinopathy-updates/what-is-the-best-way-to-load-pathological-tendon
- Saccomanni, B. (2010). Corticosteroid injection for tennis elbow or lateral epicondylitis: A review of the literature. Current Reviews in Musculoskeletal Medicine, 3(1-4), 38-40. doi:10.1007/s12178-010-9066-3
- Vicenzino, B., Cleland, J. A., & Bisset, L. (2007). Joint manipulation in the management of lateral epicondylalgia: A clinical commentary. Journal of Manual & Manipulative Therapy, 15(1), 50-56. doi:10.1179/106698107791090132
- Wuori, J. L., Overend, T. J., Kramer, J. F., & MacDermid, J. (1998). Strength and pain measures associated with lateral epicondylitis bracing. Archives of Physical Medicine and Rehabilitation, 79(7), 832-837. doi:10.1016/S0003-9993(98)90366-5