Managing Hip Instability (Dysplasia)

Managing Hip Pain in the Hypermobile Individual
Hip pain is a common reported pain in sedentary and athletic populations. Hip pain can present around the groin, front or side of one or both hips. There are certain challenges that a hypermobile individual faces when managing pain arising from the hip joint. Here we discuss some of the aspects to managing hip pain commonly known as ‘hip instability’ or hip dysplasia including Developmental Dislocation of the Hip, Acetabular Dysplasia and Developmental Dysplasia of the Hip (DDH).
What is Hip Dysplasia?
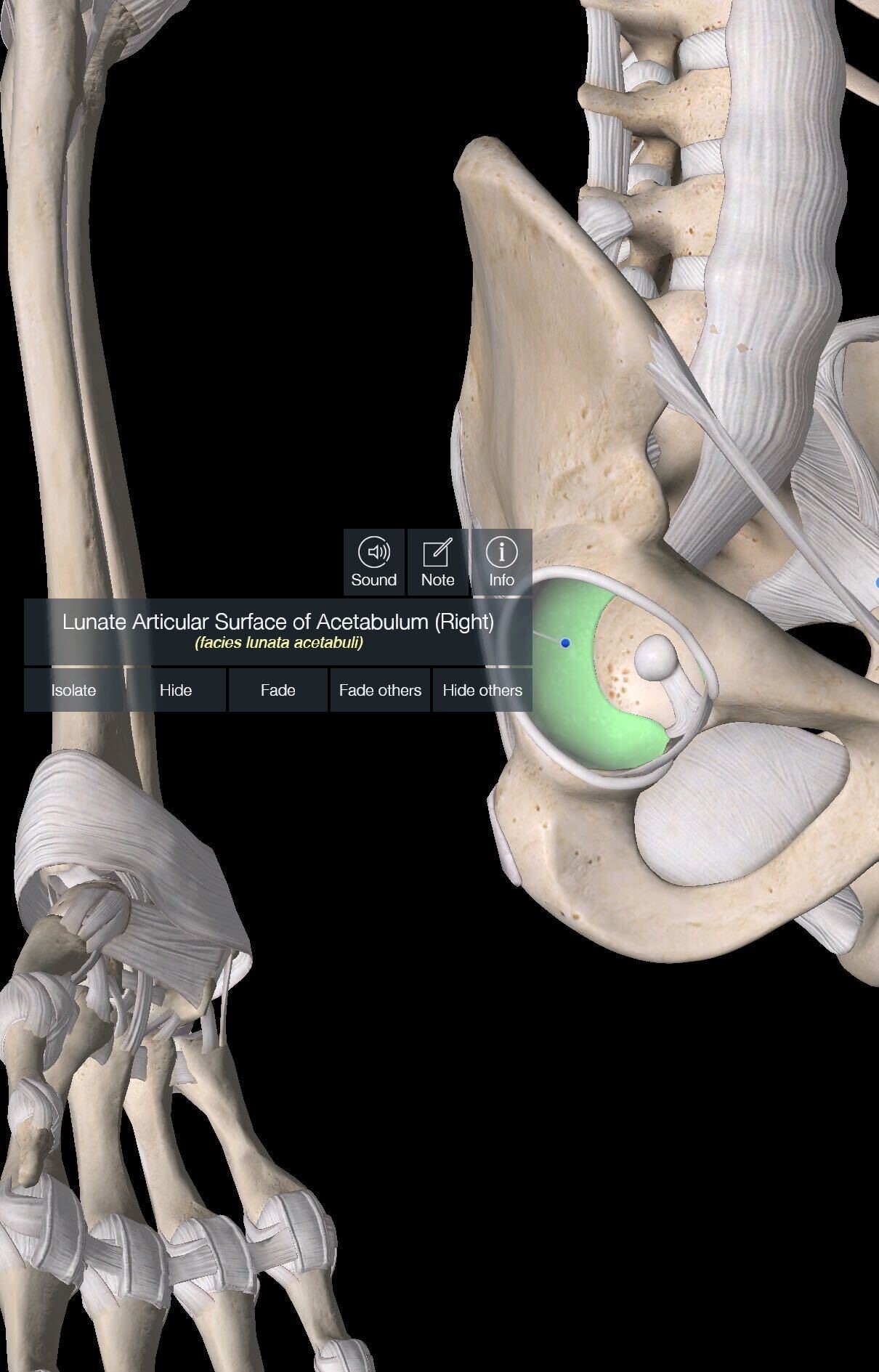
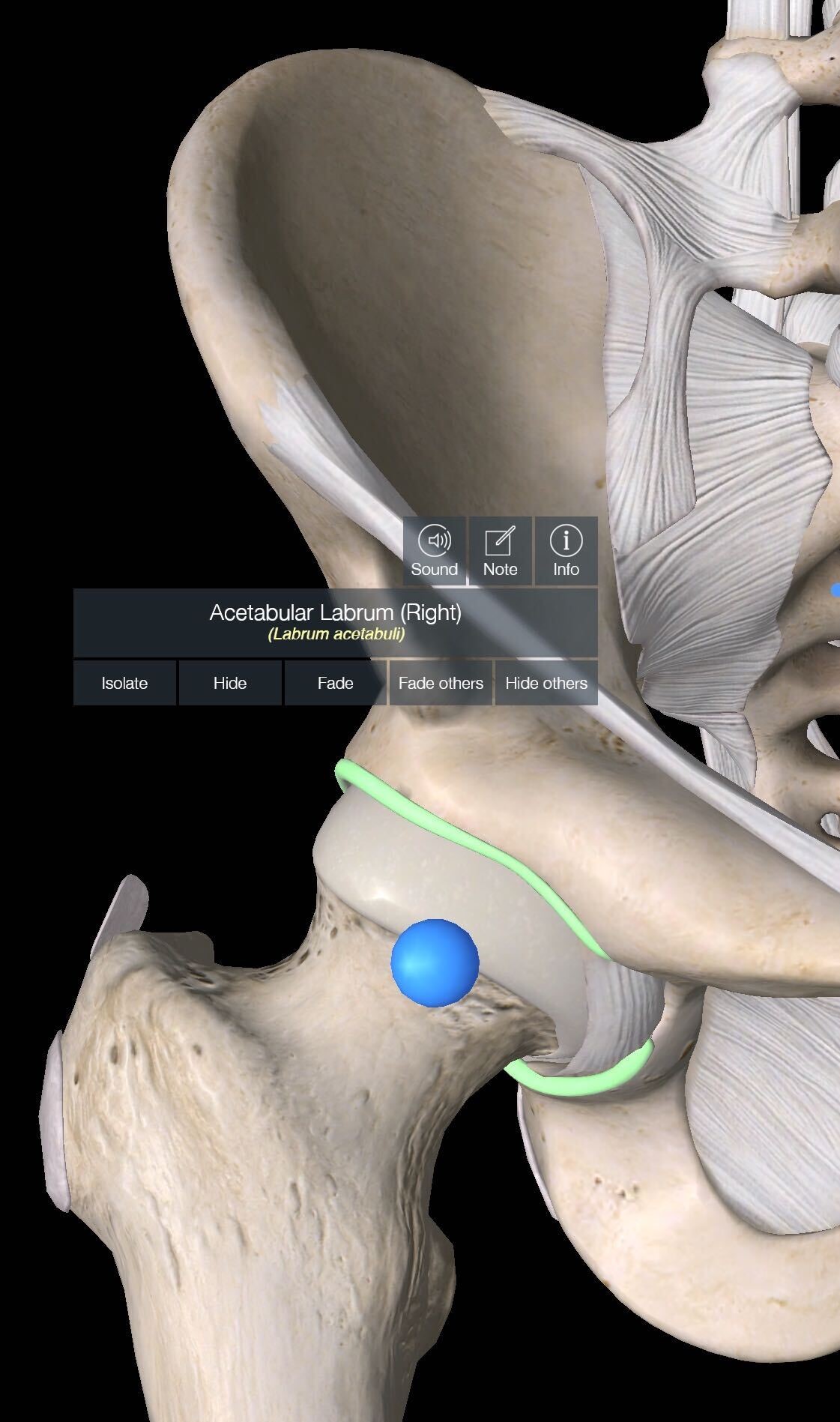
The hip joint is an inherently stable ball and socket joint that is not easily dislocated. The ball (head of femur) sits within the socket (acetabulum – pelvic bone) and is held in place by a number of large thick ligamentous tissues. It is also made more stable through a labrum lining the socket. The labrum is a triangular fibrocartilage that partially seals the hip joint and limits translation or sliding movement. It increases acetabular surface area by more than 25% and volume by 30% to help increase joint stability (highlighted in green below).
Developmental dysplasia of the hip (DDH) describes a spectrum of hypermobility and instability at the hip joint. Many people only associate it with newborns, where persistent subluxation of the hip occurs and/or when significant instability is present and plaster casting or a harness is introduced to manage this (Congenital Dysplasia). Congenital dysplasia or atraumatic instability can present later in life as adolescent or adult hip pain, particularly in females. Atraumatic instability can also arise later in life through reduced bony coverage of the femoral head (DDH, acetabular retroversion, Perthes); connective tissue disorders (Ehlers-Danlos syndrome, marfans), ligamentous laxity, surgical causes (excessive rim trim, unrepaired capsulotomy, psoas lengthening) and or repetitive micro-trauma that stress the labrum and surrounding ligaments.
The instability is not synonymous with increased risk of dislocation but rather an increased range of hip movement that is not well controlled. This translation of the head of the femur through a variety of movements can then lead to pain generators such as the labrum, capsule, synovium, chondral surfaces and local tendons. It is important to note that one can have dysplasia and be asymptomatic, with a variety of factors interlinking to lead to onset of pain at the hip.
Presentation
Pain can occur from a single incident or come on slowly over time in one or both hips. Pain is often felt around the groin, front and/or outside of the hip. It is often more prevalent in those from a background of hypermobile activities such as gymnastics, dance and martial arts. Commonly positions of ‘hip impingement’ aggravate such as bringing the knee towards the chest, getting in and out of a car, getting off the couch, up hill walking or running and prolonged sitting. The individual may also describe mechanical clicking or locking at their hip joint. These presentations can also have trouble with extension based activities such as running, stairs, wearing heels, faster walking or running. You’ll often catch this person ‘hanging off their hip’ when they stand or sway which aggravates their symptoms. This is often the position someone holding a small child leans into to make it easier to hold; shifting all weight onto one leg with a straight knee (see the right hip of the pic below).

Management
- Education; one of the pillars of managing this presentation is having a good understanding of what is happening at your hip joint, expectations for recovery and individualised needs depending on the specifics of each case. Not all cases will have the same level of symptoms, irritability or positions of instability.
- Load Modification; Understanding the various levels of stress on the hip from different activities, positions and exercises is an important aspect of settling symptoms. There are often simple modifications to everyday life such as changes to seat heights, reducing sitting time, reducing hip sway, decreasing heel heights and changing exercise volumes that can often significantly alter symptoms. For those that can manage higher level activity before onset or aggravation of symptoms changes to running volume or intensity may be incorporated.
- Reduce surrounding hypertonicity; a variety of manual therapy techniques can be incorporated to assist in reducing muscle tone and managing symptoms.
- Correct postural alignment; sometimes reducing time in sway postures or improving control in standing to reduce sway and hanging off the hip.
- Strength and Conditioning; Gradually increasing strength in the appropriate positions and with appropriate progressions is a large aspect of managing dysplasia. All major hip, trunk and lower limb muscles play a role. One large important stabiliser is the gluteus medius which stabilises the head of the femur during standing.
- Early stage rehabilitation exercises may include;
- Sway Correction
- Side-Lying Banded Hip abductions
- Prone Hip External Rotations
- Adductor Squeeze at 45 deg
- Small Range Banded Glute Bridge
- Early stage rehabilitation exercises may include;
Surgery
Surgical management is considered depending on the degree of dysplasia, patient goals, current symptoms and function. The procedure that is most effective for this presentation is a periacetabular osteotomy. It is a procedure in which a series of cuts are made to the pelvis in order to reposition the acetabulum to improve alignment. It is then fixed in place by a series of screws and new bone is formed as the hip heals. This procedure is best for younger individuals or those with minimal osteoarthritis. A progressive rehabilitation program is then used to restore strength and function over time. A video of the procedure can be found here.

Lewis Craig (APAM)
POGO Physiotherapist
Masters of Physiotherapy
Featured in the Top 50 Physical Therapy Blog
References
- Kemp, J. L., Mosler, A. B., Hart, H., Bizzini, M., Chang, S., Scholes, M. J., … & Crossley, K. M. (2020). Improving function in people with hip-related pain: a systematic review and meta-analysis of physiotherapist-led interventions for hip-related pain. British Journal of Sports Medicine.
- Kemp, J. L., Risberg, M. A., Mosler, A., Harris-Hayes, M., Serner, A., Moksnes, H., … & Ishøi, L. (2020). Physiotherapist-led treatment for young to middle-aged active adults with hip-related pain: consensus recommendations from the International Hip-related Pain Research Network, Zurich 2018. British journal of sports medicine, 54(9), 504-511.
- Palmer, A. J., Gupta, V. A., Fernquest, S., Rombach, I., Dutton, S. J., Mansour, R., … & Barker, K. L. (2019). Arthroscopic hip surgery compared with physiotherapy and activity modification for the treatment of symptomatic femoroacetabular impingement: multicentre randomised controlled trial. bmj, 364.
- Kraeutler, M. J., Garabekyan, T., Pascual-Garrido, C., & Mei-Dan, O. (2016). Hip instability: a review of hip dysplasia and other contributing factors. Muscles, ligaments and tendons journal, 6(3), 343.
- Reimer LCU, Jakobsen SS, Mortensen L, et alEfficacy of periacetabular osteotomy followed by progressive resistance training compared to progressive resistance training as non-surgical treatment in patients with hip dysplasia (PreserveHip) – a protocol for a randomised controlled trialBMJ Open 2019;9:e032782. doi: 10.1136/bmjopen-2019-032782
- Troelsen A, Rømer L, Søballe K. [Hip dysplasia: clinical assessment, radiologic evaluation and reference]. Ugeskr Laeger 2007;169:394–6
- Kuroda D, Maeyama A, Naito M, et al. Dynamic hip stability, strength and pain before and after hip abductor strengthening exercises for patients with dysplastic hips. Isokinet Exerc Sci 2013;21:95–100.
- Harris-Hayes M, Czuppon S, Van Dillen LR, et al. Movement-Pattern training to improve function in people with chronic hip joint pain: a feasibility randomized clinical trial. J Orthop Sports Phys Ther 2016;46:452–61.

![]()