


Ankle Syndesmosis Injuries

Ankle syndesmosis injuries are relatively frequent in sports such as skiing, ice hockey and soccer (1). These types of ankle injuries make up for 1-18% of all ankle sprains (1). Identification is important as missed cases with repeated episodes of instability can lead on to early degenerative changes in the ankle (1). Surgical intervention is indicated when a clear gap (diastasis) between the shin and calf bone. Conservative management for the less severe presentations remains controversial and due to its long rehabilitative nature – often professional athletes opt for a more aggressive approach via surgical treatment (1).
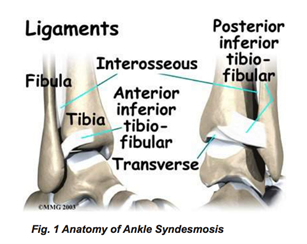
The syndesmosis is a strong ligamentous complex that connects the bottom portion of the fibula (calf bone) and the tibial notch (shin bone) (1). The syndesmosis also includes the anterior inferior tibiofibular ligament (AITFL), the interosseous ligament (IOL), the posterior inferior tibiofibular ligament (PITFLT) and the transverse tibiofibular ligament (TIFL). While the ankle is a stable joint – there remains movement between the fibula and tibia and the above ligaments help prevent them from widening.
Causation
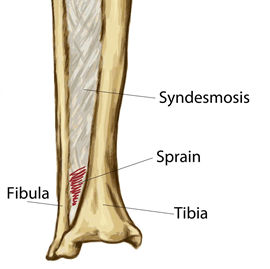
Ankle syndesmosis or “high ankle sprains’ involve the AITFL being stretched or ruptured. This typically will occur in extreme positions where the foot is moved into hyper dorsiflexion, pronation and external rotation (ie. foot bent upward and twisted outwards away from the other foot).
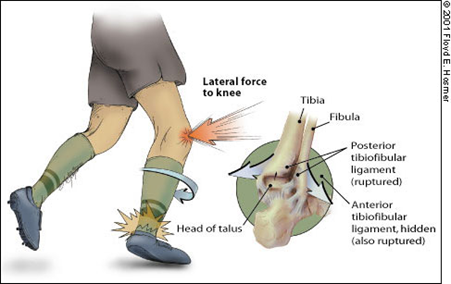
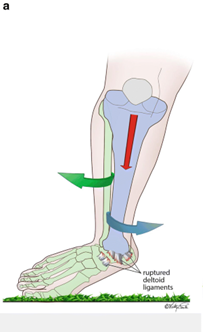
Another mechanism of injury is when the ankle is at full plantar flexion (ie foot and toes pointed away from shin) and is forced into external rotation (ie heel and bottom of foot rotated away from other foot).
Assessment and diagnosis
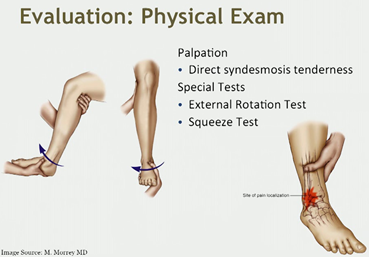
Grade I
On examination of a grade I ankle syndesmosis you would find pain with the squeeze or external rotation stress test. Tenderness around the area would be mild, the client would be able to full weight-bear and have minimal edema. On radiography you would find no mortise widening (3).
Grade II
These presentations are similar to grade I in terms of the physical examination with pain on the squeeze or external rotation stress test. They would have moderate tenderness and would find it difficult to weight-bear with a grade II. Similar to the grade I, grade II’s on radiograph imagery have no mortise widening but have moderate edema around the area (3).
Grade III
Again, on examination the squeeze or external rotation stress tests are positive. They have intense tenderness, it is impossible to weight bear on these ankles and have diffuse edema. Differing to the other grades, grade III has mortise widening on radiographs (3).
Management for each grade
Grade I:
- Boot until pain free
- Transition to brace
- Have on field progression
- Bracing and taping
- Aim to return to play after 3 weeks (3).



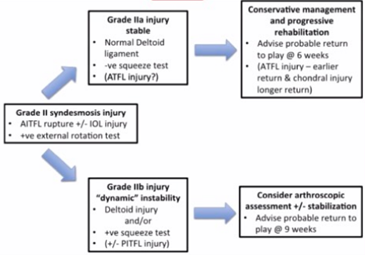
Grade II
- Difficult to manage
- Have to appropriately decide when the injured person needs an operation or whether we feel the person is able to rehabilitate conservatively
- Cader et al. (as seen below) came up with an algorithm for proposed management after assessment is completed on day 5 post injury (3).
Grade III
- Operative management
- Reduction of syndesmosis
- Tightrope fixation method
- Post operative RTS rehab
- 2 weeks non-weight bearing in boot
- Then get to weightbearing
- Return to sport program (3).
Management for syndesmotic injuries
Those without diastasis usually heal after a period of conservative management. There are generally three phases of this process.
Phase 1 (acute)
Protect the ankle and limit the both inflammation and pain (RICE regime is used). Immobilisation and reduced weight bearing status is recommended depending on the level of injury (ie which grade it is) (1). However, no matter the grade, weight-bearing should be reduced somewhat if it is painful and until walking is pain-free (1).
Phase 2 (subacute)
In this phase, joint mobilisation, strength training and restoration of basic ankle function are all recommended steps to be taken (1, 3).
Phase 3 (return to sport)
The third and final phase recognises that the individual undertakes training that involves the proprioception, balance and neuromuscular control that the ankle will need to return to. This is typically done through sport-specific drills such as weaving, cutting, pivoting, accelerating and jumping (1). Research suggests that this three phase process of treatment will provide an overall rate of good to excellent outcomes of 86-100% return of pre-injury function and almost all of those included in the study achieved a full return to sport (2).
Conclusion
Injuries involving the syndesmosis of the ankle are rather difficult to manage and can often lead to significant time less from sport as well as the risk of disability, chronic instability and/or degenerative changes within the joint. An accurate diagnosis as well as appropriate early and later phases of treatment/rehabilitation are pivotal aspects in the prevention of these detrimental results to the individual’s physical pursuits no matter the level. As mentioned earlier, obvious gapping between the bones requires surgical intervention and whether non-operative treatment is pursued or not depends on the person’s physical pursuits, grading of injury and what their goals are.
If you have symptoms similar to, or any questions regarding CTS then feel free to contact myself (details below) or your trusted healthcare professional.

Alec Lablache
POGO Physiotherapist
Featured in the Top 50 Physical Therapy Blog
Book an Appointment with Alec here
References:
- Del Buono, A., Florio, A., Boccanera, M. S., & Maffulli, N. (2013). Syndesmosis injuries of the ankle. Current Reviews in Musculoskeletal Medicine, 6(4), 313-319. doi:10.1007/s12178-013-9183-x
- Amendola A, Williams G, Foster D (2006). Evidence-based approach to treatment of acute traumatic syndesmosis (high ankle) sprains. Sports Med Arthrosc, 12(n.d), 232–6.
- Maor, D. (2020). Foot and Ankle Injuries – Treatment, Rehab and Returning to Sport: A new webinar with Dr. Dror Maor [online].






