Achilles Tendon Pain – What is your diagnosis?

Achilles Tendon pain is a common complaint from runners, sporting athletes and the general population. The most common pathology seen is Midportion Achilles Tendinopathy; with pain and tenderness in the middle of the tendon belly with activities such as running and hopping. However Midportion Achilles Tendinopathy is not the only source of pathology in this region. The Achilles Insertion, Achilles paratenon, sural nerve, retrocalcaneal bursa, superficial calcaneal bursa and, or the Plantaris Tendon can be a source of symptoms. As management of these conditions can vary considerably it’s important to get the diagnosis correct.
Here we discuss some of the distinguishing features of pain in the Achilles region.
Anatomy
The long and thick achilles tendon stores and releases energy to help provide propulsion for walking and running. The gastrocnemius muscle (Figure1, 2) and the deeper soleus muscles (Figure 3, 4 ) both combine into the achilles tendon, which inserts onto the heel bone (calcaneus). Between these two muscles and running along the inside border of the calf is the long skinny plantaris tendon, which has numerous anatomical variations (Figure 3, 4). Overlying the calcaneus is the superficial calcaneal bursa. Tracing the outside border of the Achilles tendon is the sural nerve.
Figure 1 and 2: Has highlighted the Gastrocnemius (outer calf muscle).
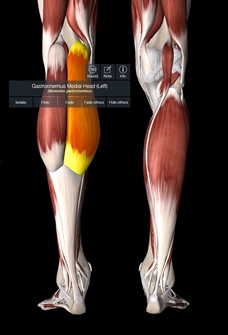
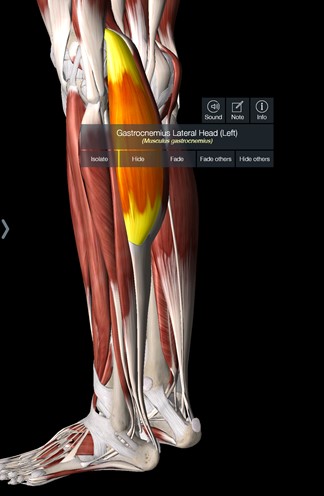
Figure 3 and 4 – Deep to the Gastrocnemius is the highlighted Soleus (inner calf muscle). Also visible in this figure 3 is the long tendon skinny tendon of plantaris.
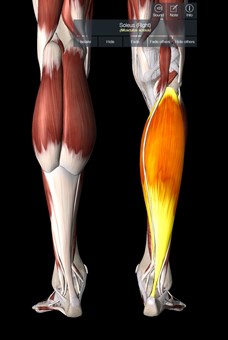
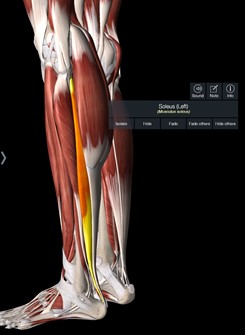
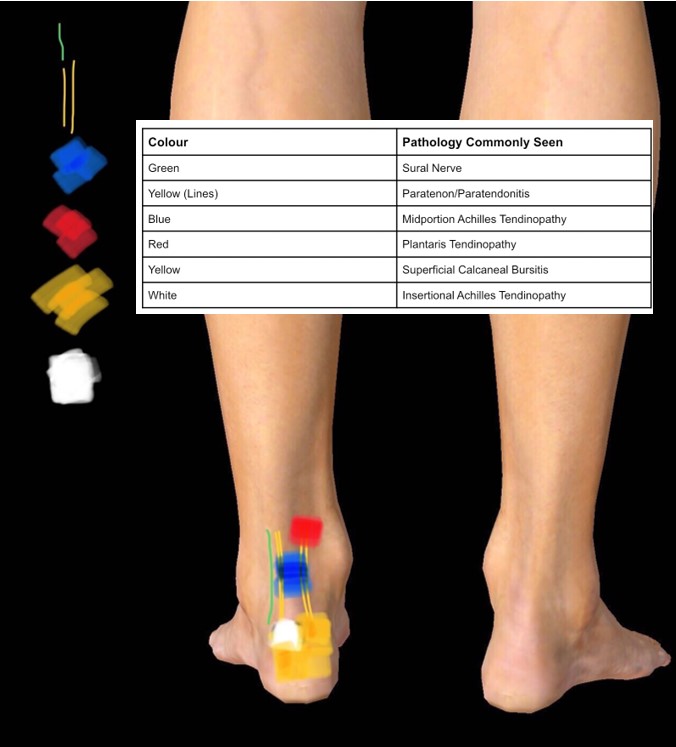
Figure 5: Common Pain Locations of Different Pathologies
Sural Nerve
The sural nerve is a sensory nerve that travels down the calf and moves to the outside of the Achilles. Compression or irritation of the sural nerve can result in lateral achilles pain, with or without pins and needles or numbness into the foot. Pain can be localized by finger pressure in the middle part of the calf, just lateral to the musculotendinous junction of the Achilles tendon. Palpation of the nerve can often help identify if it is symptomatic, alongside not fitting a typical pattern of tendon pain (see below)(1). Irritation of the sural nerve may also co-exist with irritation of the tendon sheath and may not be best treated (initially) with a strength based program.
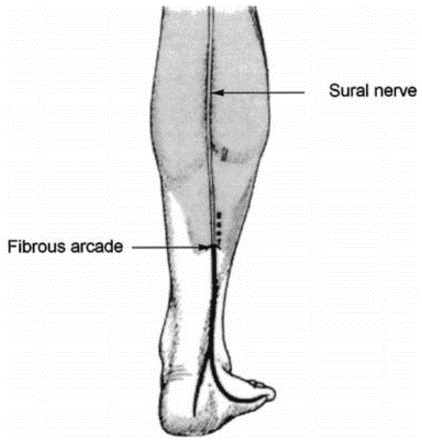
Figure (6) Anatomic drawing depicting the surgical incision of both the fibrous arcade and the superficial sural aponeurosis (dotted line) where entrapment may occur (from Fabre et al. 2000).
Midportion Achilles Tendinopathy
Midportion Achilles Tendinopathy is the most common form of Achilles pain. It is characterised by localised pain with a squeeze test or 1 finger pain area in the middle of the tendon. It typically follows a pattern of being sore at the start of activity, ‘warming up’ and being painful over the next 24-48hrs after exercises. It will have pain localised to its location that is worse with higher levels of tendon load or ‘springy loads’; so for example a calf raise may have slight pain, a double leg jumps more painful, forward single leg hops more painful again. Faster running is often associated with more significant symptoms. We have previously written about managing this type of presentation here.
Insertional Achilles Tendinopathy
Insertional Achilles Tendinopathy is a distinct clinical entity which differs midportion achilles tendinopathy in its behaviour. Its location is lower and often on the outside of the achilles where it inserts onto the heel bone (calcaneus). Due to its location insertional achilles tendinopathy is often aggravated by compressive loads. These presentations will be more likely to be aggravated from decline calf raises (heels below ground level such as off a step) (2) and will prefer to be in shoes rather than barefoot. These cases are often rehabilitated with a progressive strengthening program and exposure to springy loads whilst minimising activities and positions of compression. Wearing shoes with a higher heel or external wedge can often be helpful for these cases.
Achilles Paratenonitis
The paratenon is the sheath that surrounds the tendon. Achilles Paratenonitis refers to an inflammation of this tendon sheath. It is often aggravated by friction rather than a typical stretch shorten cycle or ‘springy’ load. It can occur in cyclists, swimmers, dancers, rowers as well as runners. These presentations often do not follow the typical warm-up behaviour of a mid-portion tendinopathy and will get worse with activity the longer it goes on. Visible inspection of the tendon often looks puffy with localised swelling. This type of Achilles tendon pain is important to recognise as it will often be aggravated by traditional strength based achilles rehabilitation and management may first need to focus on settling the localised inflammation.
Retrocalcaneal Bursitis
A bursa is a fluid filled sac that is found at numerous sites around the body where tendons and muscles move over bony joint areas. There are two notable bursae in the achilles region; the retrocalcaneal bursa and superficial calcaneal bursa. The retrocalcaneal bursa sits in retrocalcaneal recess, a space above the calcaneus and behind the achilles tendon. Pain in this location on activity may indicate involvement of the bursa. Due its close relationship with the Achilles insertion these may have co-existing pathology.
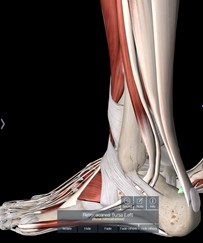
Figure 7 (Highlighted in green- Retrocalcaneal Bursa)
Superficial Calcaneal Bursitis
The Superficial (or subcutaneous) calcaneal bursa sits on the posterior aspect of the heel and partially overlaps the insertion of the Achilles tendon. As the name subjects the superficial bursa sits quite close to the surface of the skin. As a result it can become irritated through compression or friction from footwear. Testing an activity with one shoe, then performing the same activity barefoot (or with other footwear modification) with significant improvement in symptoms may suggest this is the cause. Modifying footwear with appropriate padding can then often assist in settling symptoms.
Figure 8 (Highlighted in green – Superficial or Subcutaneous Calcaneal Bursa)

Plantaris Tendinopathy
Pain location of plantaris tendon pain is typically medial (inside), where the plantaris sits adjacent to the Achilles. Pain is typically high, 6-8 cm above the Achilles insertion, where the plantaris merges with the Achilles tendon and its tendon sheath. The pattern of symptoms is often similar to an Midportion Achilles tendinopathy, with start up pain, then decreasing with greater duration of physical activity. Symptoms can then also increase higher tendon loads such as jumping and hopping. Plantaris tendinopathy often behaves more like an insertional achilles with pain into dorsiflexion (such as a calf raise over the edge of a step) and not liking being barefoot, but has a much higher pain location (3). There can also be an increased suspicion of these cases in those who have described a history of soleus strains.
Further information on planters tendinopathy can be found here.
Other
Any of the pathologies mentioned above can occur in combination. Other possibilities of pain include referral from the lumbar spine or posterior ankle impingement. Posterior ankle impingement can have symptoms in an area similar to the retrocalcaneal bursa. It is more common in sports like dancers where aggravation of the joint occurs at the end range plantarflexion (such as right at the top of a calf raise).
Recognising the differences in the location and behaviour of Achilles pain is important in the diagnostic process. Getting this right can ensure an appropriate and efficient management path is undertaken.

Lewis Craig (APAM)
POGO Physiotherapist
Masters of Physiotherapy
Featured in the Top 50 Physical Therapy Blog
References
- Fabre, T., Montero, C., Gaujard, E., Gervais-Dellion, F., & Durandeau, A. (2000). Chronic calf pain in athletes due to sural nerve entrapment. The American journal of sports medicine, 28(5), 679-682.
- Wiegerinck, J. I., Kerkhoffs, G. M., Van Sterkenburg, M. N., Sierevelt, I. N., & Van Dijk, C. N. (2013). Treatment for insertional Achilles tendinopathy: a systematic review. Knee Surgery, Sports Traumatology, Arthroscopy, 21(6), 1345-1355.
- O’Neill, S. (2015) Physio Edge 042 Treatment of Plantaris & Achilles Tendinopathy with Seth O’Neill., D. Pope.