Returning low back and tendon injuries to sport

The first question many athletes will ask their health professional is “When can I play again?”. Returning to sport is a complex and multifactorial process and one that requires an accurate assessment, rehabilitation that is evidence based and educational points to guide the athlete throughout the process. La Trobe university presented a 2 day course on returning the injured athlete to sport and two injury types discussed by Kellie Welkie (low back pain) and Professor Craig Purdam (tendons) have been presented in this blog.
Low back pain in athletes
Assessing LBP
- Look at F/E and look for how much movement happens in LSp
- Tone changes on a straight leg raise (SLR)
- Neuro Ax, usually L4/5 NR problems with radicular pain (have big difference)
- Slump is good for S1 // burning bottom pain
- Prone knee bend in upper Lsp
Initial phase of an injured lumbar spine disc
- analyse the sport and what range is required for it (ie. for rowers, lumbar extension is not needed and therefore is not focused on through the return to sport reha)
- Cat/camel unweighted position to get movement in low back to get a neutral flexed position (don’t push into pain) upregulate the muscle tone you want to get rid of
- Avoid extension of the low back if that brings on symptoms
- Reverse lunge is a good way to get rid of psoas tightness and is suggested 5 times on each side is a good amount to retest and look for improvement
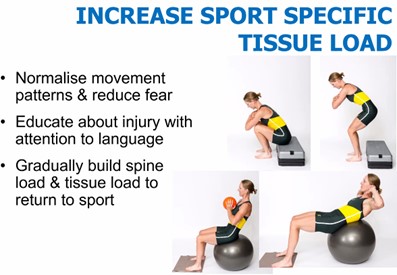
Throughout the rehab process and while loading tissues it is important that clinician’s address modifiable risk factors and consider why they got the injury in the first place. Gym modifications for those with low back pain
- Avoid axial load
- Continue to load in the gym in some way. It is advised to not take the athlete out of the gym environment completely as this has been shown to inhibit their psychology
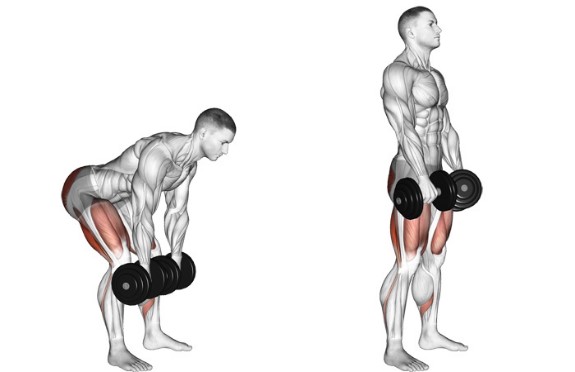
- Romanian deadlifts (seen below) are a good way to continue loading in the gym without affecting the low back. However, it is important form is checked for little to no lumbar spine movement
- Jefferson curls are appropriate as long as the movement is a requirement of the sport
- If pain in the low back lasts after the session ie into next morning then review the load that was undertaken during the session
Load variables when returning to sport
- In rowing can change seat height, middle of 8, get rate down
- Find out what their load was like just before injury and 3-4/12 prior
- this helps with knowing what to return them to
- Can use an elliptical trainer on a sore back
Summary
- Early control of pain will help normalise movement
- Address modifiable risk factors as part of rehab
- Plan is to gradually increase tolerance of tissue loading
- RTS plan should involve the athlete, coaches and/or parent
A suggestion when educating a client with low back pain is to not show the sometimes exaggerated blisters on the spine models, try to avoid showing the MRI and talk more about the tensile loads on the back that are currently alerting us. Through rehab we need to get them to calm down and to take load again without giving those pain signals.
Tendon-related injuries in athletes
When they occur Returning tendons to sport take a series of steps and progressions to return them to the load tolerance they were undertaking without symptoms prior to the injury. Professor Craig Purdum (2020) states that when a tendon related pathology occurs, it is important to back them off a little then build them back up. It is also important to note that faster athletes are found to have recurrence more frequently especially when it is an intramuscular tendon. If the tendon injury is a serious tear, it is advised not to use crutches as this will aid in avoiding stretching of the scar. Controlling the tendon tear to avoid lengthening in the early stages helps with overall recovery and rehabilitation.
Rehab
Strength
- Primary modifiable risk factor
- Formal strength program ~3 exercises, 3 sets to exhaustion, 3 times a week
- Limit range early and address the outer ranges later in rehabilitation
- Monitor each side’s strength closely throughout the rehabilitation as this may help identify complications in recovery
- Address specific activation deficits
- Progress to gym-based elastic/power stimulus
- Address synergists
- Address contributing kinetic chain elements (spine, hip, knee, ankle)
Eccentrics as an intervention
- Eccentrics stimulate adhesion as well as lengthening
- It is suggested to induce DOMS on a couple of occasions
- Potentially after the initial 4-6 weeks and once they have the range strength and control through range
- Eccentrics are understanded to be under greater consideration with those experiencing recurrent injuries
Suggested exercises:
- Soleus
- Backwards walking on treadmill
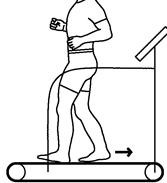
- Walking downstairs (use elevator to go back up)

- Hamstring
- Single leg 45 deg hip extension
- Sliders
- Romanian deadlifts (RDLs)
- Rectus femoris
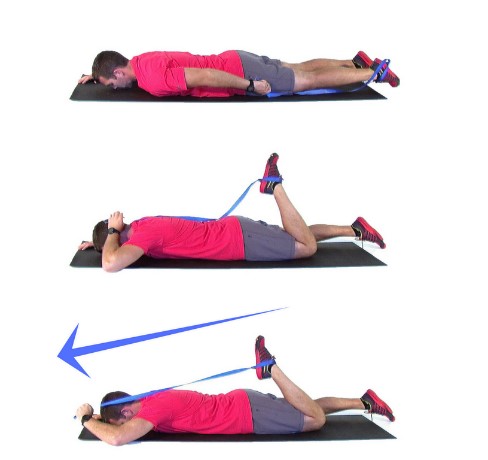
- Knee extension in prone (pulleys or theraband)

- Rectus bridge (double then progress to single)
-
- Build to 3 x 30 reps

Summary
- Most myotendinous injuries do well
- Rehabilitation follows a stepwise increase in application of both the muscle force and rate of the loading stimuli. This is followed by regeneration of this to the tendon
- Rehabilitation should be scaled to the individual and their sporting demands (ie only some sports require the highest levels)

Alec Lablache
POGO Physiotherapist
Featured in the Top 50 Physical Therapy Blog
References:
- La Trobe University. (2020). Return to sport symposium – when can I play again? [ONLINE]. Retrieved from http://semrc.blogs.latrobe.edu.au/events/return-to-play-symposium/