


Best Practice Rehabilitation Following Total Hip Replacement

Total Hip Arthroplasty or Total Hip Replacement (THR) is a common surgical procedure for long term hip joint related pain. In Australia over 37000 replacements were done in 2017 (1). It can improve quality of life and decrease pain for those with long term hip pain (2-4). Despite being a common surgical procedure, navigating decision making before surgery and after can be difficult for those undergoing a THR. Many people are unaware of how long recovery will take or what is involved. Common questions we are asked in the clinic include; “do I need a hip replacement? What can I do to help my hip? What does rehabilitation after surgery look like? When will I be back to normal?”.
In this blog we aim to increase understanding of indications for a total hip replacement and what best practice rehabilitation looks like.
Hip Joint Anatomy and Prosthesis
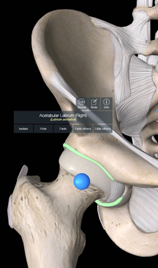
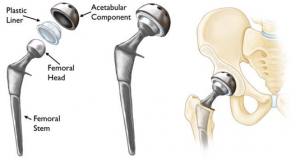
The hip joint is a ball and socket joint connecting the femur (ball) with the pelvis at the acetabulum (socket) A total hip replacement (THR), as its name suggests, is a surgical procedure where the head of the femur and the acetabulum are replaced with a metallic prosthetics that replicate the function of the joint.


Reasons for Total Hip Replacement
The principal causes for total hip replacement are osteoarthritis (which accounted for 90% of procedures in the UK in 2017), fractured neck of femur (5%), avascular necrosis (2%), dysplasia (2%), and inflammatory arthritis (1%) (5). Osteoarthritis (OA) is a painful chronic joint disease characterised by structural changes to the whole joint, including loss of articular cartilage, development of osteophytes, synovial inflammation, subchondral bone changes, muscle weakness, and ligamentous laxity. It results from a complex interplay of genetic, metabolic, biomechanical, and biochemical factors (6). Although previous joint injury is a risk factor, OA is not simply wear and tear of the joint (11). Symptoms are not reliably associated with the degree of structural disease on imaging (13). This means on imaging the disease process may look significant yet improvements in pain and function can still be made without surgery. Despite a diagnosis of OA, the minority, 10% people in their lifetime will go on to need a joint replacement and prognosis is generally favourable and the trajectory of symptoms is largely flat (11). This means that symptoms will not necessarily just get worse and focus can be on the things that help with the disease and improve pain and function. Optimal conservative management is outlined below in ‘Prehabilitation, .’ As part of this management, best practice guides recommend exercise as essential for all patients, irrespective of disease severity, age, comorbidity, pain severity, or disability. Similar improvements in pain and function can be seen with exercise as those achieved with analgesics and non-steroidal anti-inflammatory drugs (NSAIDs) (7). Alongside exercise consultation with dietician and community providers to support weight loss. The benefits of weight loss are not only to reduce mechanical loads through the joint but to reduce systemic markers of inflammation (12).
So when does one end up with an elective hip replacement? THR is often reserved for patients with severe disease defined as persistent moderate to severe pain, functional limitation (this may mean limited walking, difficulty sitting, difficulty putting on shoes and socks, unable to do regular daily activities), and reduced quality of life despite optimal conservative treatment (longer than 3 months), together with radiological markers of disease.
For those going on to receive a THR, most patients can expect their prosthesis to function without complications for more than 20 years (5). There are increased challenges for THR performance for young patients and older patients who are active. Overall, an unfavourable pain outcome was seen in at least 4.8% and up to 20.5% of patients after hip replacement (8). Age at surgery has a significant effect on revision risk or need for another (revision) hip replacement. The lifetime risk of revision for male patients aged 50–54 years is approximately 30%, compared with 8% for their counterparts aged 70–74 years. This large risk differential may lead some patients to delay surgery, and increase attempts to manage and prehab their hip with best practice management (below) (9). Other studies looking at THR survivorship rates have shown increasing positive longevity with 97% lasting up to 22 years (25), 73% at 30 to 40 years (26) and 75% at 22 years (27).
Causes of revision surgery include aseptic loosening (most common 48% of revisions), dislocation (with 77% of them affected within the first year), joint infection, periprosthetic fracture and implant malpositioning. Age, muscle tone, non-compliance with avoidance of specific movements, surgical approach, and component position and size influence the dislocation rate (5). Overall risk of complication and dislocation are considered low, particularly with anterolateral and anterior approaches.
Surgical Approaches
Once a decision to undergo surgery has been made, the decision about which approach to do will be made by the surgeon.
There are 3 common approaches for a hip replacement;
1. Posterior
2. Anterolateral
3. Direct anterior.
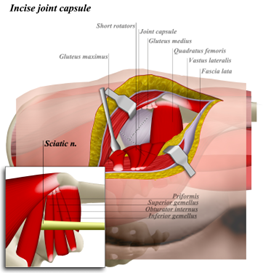
1. Posterior
A posterior approach is the most commonly used approach for THR (15). The patient is placed in the lateral position and the incision is made over the posterior aspect of the greater trochanter. It has the benefit of not interfering with the abductor mechanism, however, there is a low risk of damage to the sciatic nerve during dissection or compression under retractors, as it lies over the external rotator muscles. The inferior gluteal artery may be damaged as it leaves the pelvis beneath the piriformis and supplies the gluteus maximus muscle. The main disadvantage of this approach is a rate of dislocation of about 3.23% for the posterior approach (3.95% without posterior repair and 2.03% with posterior repair), 2.18% for the anterolateral (16). From a rehabilitation perspective, incisions to the large gluteus maximus and deep hip rotators affect strength and function and can change recommended exercise programs post-surgery.

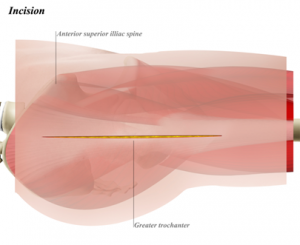
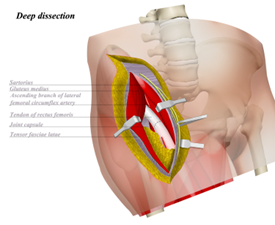
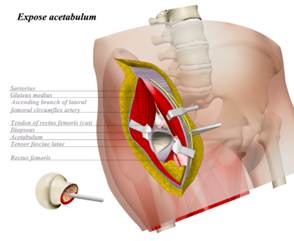
2. Anterolateral
The anterolateral approach was described separately by Watson-Jones in 1936 (15). The patient is placed in either the supine or lateral position and the plane between tensor fascia lata and gluteus medius is incised. The abductor mechanism (tensor fascia lata and gluteus medius) are the lateral stabilisers of the hip and must be released to allow adequate view of the anterior capsule of the hip. This release can be done either by a trochanteric osteotomy or a release of the gluteus medius. This can mean more effect to lateral stability post surgery, however there are mixed reviews on a number of studies looking at functional differences between posterior and anterolateral approaches. One such study reported that 107 patients (25%) who underwent THR using a lateral approach described developing a limp post-operatively. This was more than twice as many as in those who underwent THA using the direct anterior or posterior approaches (17).
3. Direct Anterior
The direct anterior approach which was initially described by Hueter and subsequently by Smith-Petersen and Judet and Judet (15) is associated with a reduced risk of dislocation, faster recovery, less pain and fewer surgical complications (15, 19). With the patient lying on their back an incision is made between the tensor fascia lata and sartorius muscles to access the hip. This avoids detachment of muscle from bone. The disadvantages of the anterior approach are thought to include a steep learning curve to do the procedure and the need for further release of tendon and capsule and the difficulty of using it in obese patients (19). 20)
Prehabilitation – Pre-Surgery Rehabilitation
Prehabilitation or pre surgery exercise can be helpful to improve outcomes post surgery, by leading to an increased platform of strength, aerobic exercise and function. Most individuals with advanced hip arthritis are more likely to have a lower level of muscle strength (23) exercise tolerance, and reduced aerobic capacity (24) in comparison with healthy individuals. Increased pain and deterioration of the hip also leads to decreased mobility and reduced independence in some activities of daily living. As most common causes of THR are due to osteoarthritis exercise can have a positive effect on reducing symptoms from the disease and in some cases lead to delay of surgery or cancellation of surgery due to improvements in pain, function and QOL. A sample 8-week pre surgery exercise program improved levels of pain, stiffness, physical function, hip flexion ROM, and muscle strength in patients with end-stage hip disease (22). In this study these benefits over a control group (without exercise) were maintained into the postoperative period (22). Clinical evidence suggests that fit, strong patients generally rehabilitate more quickly after surgery compared with patients who are less fit (22).
Prehabilitation involves assessing baseline strength of key movements at the hip (abduction, adduction, flexion, extension) and/or key muscle groups; gluteus maximus, gluteus medius/minimus, quadriceps, hamstrings, adductors and calves. This can be used to identify specific deficits and imbalances as well as monitor progress over time. Functional measures can be taken such a 6 minute walk test (distance walked in 6 minutes), timed up and go (a test to see how quickly one can rise from a chair walk 3 metres around a cone and return to a chair), weighted best efforts of full body exercises such as squats, split squats or deadlifts. For example, how many 10kg squats can you do? Outcome measures or questionnaires can be used to give comparison measures of before and after and to track progress. Sample questionnaires include the HOOS or HAGOS.
Key features of the rehabilitation phase include; education, symptom modification, early load introduction and focused strength work. These are similar to post-surgery guides, however time frames may differ. For example education may centre around the benefits of lifestyle change, discussion with other health professionals around weight loss and working on developing strategies to achieve goals of the individual. For example a common goal is to be able to play with grandkids; this is where strength work can aim to make it easier to get on and off the ground or picking up the grandchild from the floor. Commencing a walking program can improve endurance and cardiovascular health. As there are many overlapping features of a prehabilitation program or preventative program to a post operative rehabilitation program we will group these together in this article; with the first 2 phases below often of much shorter duration than for the postoperative group.
Post Surgery Rehabilitation
Conceptually it is nice to work in simple stages for post operative rehabilitation. It assists clients to know the goals and aims for the next few weeks and highlight progress when moving through stages. There is considerable overlap between stages and individual differences depending on variables such as surgery type, age, pre-operative fitness and strength. Routinely those undergoing a hip replacement are informed that rehab can take a full year. Time to be pain free and complete normal activities of daily living can be much sooner than this but to achieve return to strength and full function it is helpful to set up a sustainable long term rehabilitation path.
Stage 1 – Protection and Mobilising (Day 0 – 8 Weeks)
Protection and mobilising are the first goals post surgery. We want to look after the surgical site, keep pain well managed and begin regular movement. This begins the day of surgery or the following day in the hospital when a physiotherapist visits the ward. Early physiotherapy includes:
- Simple bed exercises are taught (circulation exercises, upper limb exercises, assisted lower body exercises and bridging with the non operative leg)
- Mobilising with an aid such as forearm support frame and assistance
- Getting in and out of bed
- Sitting out in a chair and getting up out of the chair
- Education about movements to avoid (this is aimed at preventing dislocation) and primarily for the first 3 months.
- Posterior Approach – Avoid crossing legs, avoid flexing hip past 90 degrees, avoid low chairs, avoid sleeping on the operative side.
- Anterolateral Approach – Avoid hyperextending the hip or turning it outwards and crossing legs, sometimes no movements to avoid
- Direct Anterior – Commonly no restrictions (occasionally outward rotation)
- The use of hip precautions have been questioned in studies in recent years. A 2017 study reported that routine use of hip precautions in the primary setting appears unnecessary and potentially detrimental (28). A 2015 systematic review concluded that in anterolateral approaches the rate of dislocation is low and is not improved by hip precautions. These precautions are associated with a slower return to activities, significant expense, and decreased patient satisfaction (29). Often precautions are guided by the surgeon on an individual case to case basis.
Over the next 2-3 days you will progress how far you can walk with a frame and then crutches and stairs are taught. Criteria to be discharged include safe and independent walking with an aid (typically crutches), can transfer from bed/chair safely, can ascend and descend stairs with supervision and have adequate home assistance and support. Discharge exercises are given and can vary significantly. Once discharged from hospital there are multiple options and variance in subsequent care;
- In house rehabilitation facility – typically for those who are not ready to be discharged home (1-2 weeks)
- Home Exercise following guide from hospital physiotherapist
- Follow up outpatients physiotherapy at the hospital
- Physiotherapy at home from a mobile rehabilitation provider
- Physiotherapy at a private practice
This author would suggest follow-up with physiotherapy within 2 weeks following discharge from hospital. This follow up will provide opportunity to discuss symptoms, home set-up, current challenges day to day, get hands on relief as needed and make modifications to crutches and home exercises. A sample home exercise program at this stage may look like this; 1 set of 6 twice a day:
- Gentle range of movement exercises
- Sit to stand (high chair)
- Glute bridge
- Adductor squeeze (at shoulder width)
- Supine Hip Abduction
- Calf Raises
- Additional harder single leg exercises can be completed on the non-operative leg; eg leg press, step ups, leg extensions, single leg calf raises and single leg bridges.
Stage 2 – Load Introduction (6 weeks – 12 weeks)
The second stage of recovery can be considered load introduction, here we progress from simply getting moving and letting symptoms settle and begin to introduce more resistance exercise into the system. Our priorities in this phase are to progress off crutches and maintain a smooth normal gait (walking pattern) and familiarise ourselves with key strength patterns to move into stage 3. Early in this phase we will retake our key tests from the pre-surgery phase to monitor progress.
One of the primary difficulties for people in this post-operative phase is to regain a normal gait pattern (31-33). With anterolateral approaches the surgical incisions go through large musculature lateral hip muscles which affect postoperative strength, combining that with weakness that exists pre-operatively can be part of the challenge to regain normal walking mechanics. One study looked at the gait mechanics of THR patients and found that walking pattern did not return to normal even at 10.6 months, on average (±2.6 mo), following surgery (31). THR patients walked with lower operated-hip abduction moments (more hip collapse), sagittal-plane range of motion, as well as lower generated and absorbed power. This may be consequential to pain-avoidance strategies adopted pre-operatively, apprehensions associated with their new prosthesis (31) and/or weakness through hip abductors and hip extensors (TFL, Gluteus medius/minimus/maximus) (32). This will often present as a Trendelenberg sign when standing on one leg, where the opposite side of the hip drops excessively (below we can see this when standing on the left leg – noting the pelvis isn’t level and the angle made with the thigh is more acute).


Strategies to improve gait/walking mechanics can be considered bottom-up approaches: they act on the distal physical level (bottom) or aiming at influencing the neural system (top), being able to rehabilitate the patients due to the mechanisms of neural plasticity and motor learning (34). In this phase we include exercises targeted at both; increasing the strength of the hip muscles and distal muscles (quadriceps, hamstrings and calves – the latter of which can really aid propulsion in cases of hip pain) as well as motor learning exercises to help regain normal walking. A sample snapshot of exercises during this phase may look like:
- Gait Drills
- Wall March – high heel lift versus high knee lift


-
- March with Arm Reach overhead


-
- Walking with hands overhead (aim for high hands)
- Box Squat
- Feet elevated Glute bridge
- Adductor squeeze (at shoulder width)
- Supine Hip Abduction (Iso push)
- Calf Raises
- Additional harder single leg exercises can be completed on the non-operative leg; eg leg press, step ups, leg extensions, single leg calf raises and single leg bridges.
Stage 3 – Strength (10 weeks onwards)
This is the longest phase of recovery and the most important. As pain settles and activity increases it is important to regain a normal gait, cardiovascular endurance and specific strength. In this phase we want to work towards strength measures equalling the non operative side and surpassing prehabilitation scores. There are a lot of options for strength work in this phase including compound movements such as squats, deadlifts and split squats. These can be included alongside gait drill progressions from stage 2 and exercises to address specific muscle deficits. Cardiovascular options include increasing walking volume as gait is improving and soreness is minimal. Alternatives include swimming, elliptical and riding. Some find riding difficult due to the amount of hip flexion and a higher handlebar and upright body position may be easier.
Over a series of months weights can be added, then increased as sets and rests move from higher volume of low resistance such as 3 sets of 15 reps; towards 4 sets of 5-6 reps.
Key variables from this phase are to increase the strength and hypertrophy of key muscle groups. Another important aspect in this phase is self-efficacy. Self-efficacy can be considered an individual’s belief in their capacity to act in the ways necessary to reach specific goals. Essentially one’s assertion of their ability to improve and progress has a significant effect on their progress (10). Experiences of possessing required skills, inspiration by other group participants, encouragement from physiotherapy staff and altered interpretations of symptoms contributes to increased self efficacy and maintenance of physical activity in the long run (10). This is in part why we advocate for some rehabilitation in this phase to be done in a group setting; to help with more physiotherapist feedback and input, closer supervision, support and encouragement from multiple staff and fellow participants.
A common question from this stage is how do I know when to stop or how long is it going to take. This is a combined decision based on level of function, strength scores and future goals. At this point it is good to reflect on the physical activity guidelines; where it is recommended that strength training for adults take place at least twice a week (35). The honest answer is often you should continue the exercises or some form of modified strength exercises twice a week for the rest of your life. This is partly why developing self efficacy is important. Maintaining this practice of strength work can have numerous benefits including (35);
- Strong muscles and bones
- Reduce the risk of, or help manage, type 2 diabetes and cardiovascular disease
- Maintain or improve blood pressure, cholesterol and blood sugar levels
- Reduce the risk of some cancers
- Prevent unhealthy weight gain and help with weight loss.
Here many people continue strength based exercises in some form for longevity; this may then look like various forms of gym training, home strength exercise, reformer or mat pilates, yoga and or callisthenics.
Stage 4 – Return to Performance (6 months onwards)
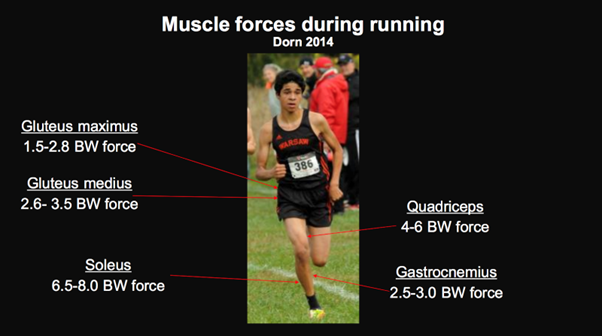
The final stage of rehabilitation is returning to performance. Once a good base of strength has been achieved rehabilitation exercise can move towards the requirements of a sport or activity. This can take many months and overlap with ongoing strength work in stage 3. For running based sports or activity this often means the inclusion of jumps and plyometric work as you build towards the demands of running. As you can see from the image below muscle forces during running can be quite high. A good starting point can be running drills and low amplitude plyometrics (A skips, b-skips, pogos). Light sport specific drills and small sided games should be implemented prior to full training, full intensity or full games. Volume of exercise can be slowly increased as it is comfortable and tolerable. For those returning to performance it is increasingly important to continue strength based exercises into the future to ensure tissue capacity remains higher than the demand of the sport or activity.

Lewis Craig (APAM)
POGO Physiotherapist
Masters of Physiotherapy
Featured in the Top 50 Physical Therapy Blog
References
- Australian Orthopaedic Association. Australian National Joint Replacement Registry annual report 2018. 2018. https://aoanjrr. sahmri.com/annual-reports-2018 (accessed Oct 1, 2018).
- March LM, Cross MJ, Lapsley H, et al. Outcomes after hip or knee replacement surgery for osteoarthritis. A prospective cohort study comparing patients’ quality of life before and after surgery with age-related population norms Med J Aust 1999; 171(5): 235-8.
- Jones CA, Voaklander DC, Johnston DW, Suarez-Almazor ME. Health related quality of life outcomes after total hip and knee arthroplasties in a community based population J Rheumatol 2000; 27(7): 1745-52.
- Ethgen O, Bruyere O, Richy F, Dardennes C, Reginster JY. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature J Bone Joint Surg Am 2004; 86-A(5): 963-74.
- Ferguson, R. J., Palmer, A. J., Taylor, A., Porter, M. L., Malchau, H., & Glyn-Jones, S. (2018). Hip replacement. The Lancet, 392(10158), 1662–1671.doi:10.1016/s0140-6736(18)31777-x
- Hunter, D. J., March, L., & Chew, M. (2020). Osteoarthritis in 2020 and beyond: a Lancet Commission. The Lancet, 396(10264), 1711-1712.
- Bennell, K. L., Hunter, D. J., & Hinman, R. S. (2012). Management of osteoarthritis of the knee. Bmj, 345.
- Beswick, A. D., Wylde, V., Gooberman-Hill, R., Blom, A., & Dieppe, P. (2012). What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ open, 2(1), e000435.
- Most patients can expect their prosthesis to function without com- plications for more than 20 years. Ongoing challenges include further improvements to implant performance for young patients and older patients who are active, ensuring the safe introduction of new implants, and developing strategies to identify osteoarthritis early and slow its progression, to reduce the number of patients requiring major surgery.
- Hammer, N. M., Bieler, T., Beyer, N., & Midtgaard, J. (2016). The impact of self-efficacy on physical activity maintenance in patients with hip osteoarthritis–a mixed methods study. Disability and rehabilitation, 38(17), 1691-1704.
- https://podcasts.apple.com/gb/podcast/the-shoulder-physio-podcast/id1605866322
- Messier, S. P., Mihalko, S. L., Legault, C., Miller, G. D., Nicklas, B. J., DeVita, P., … & Loeser, R. F. (2013). Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: the IDEA randomized clinical trial. Jama, 310(12), 1263-1273.
- Hunter, D. J., McDougall, J. J., & Keefe, F. J. (2008). The symptoms of osteoarthritis and the genesis of pain. Rheumatic Disease Clinics of North America, 34(3), 623-643.
- https://orthoinfo.aaos.org/en/treatment/total-hip-replacement/
- Meermans, G., Konan, S., Das, R., Volpin, A., & Haddad, F. S. (2017). The direct anterior approach in total hip arthroplasty: a systematic review of the literature. The bone & joint journal, 99(6), 732-740.
- Masonis JL, Bourne RB. Surgical approach, abductor function, and total hip arthroplasty dislocation. Clin Orthop Relat Res2002;405:46–53.
- https://www.orthobullets.com/approaches/12021/hip-anterolateral-approach-watson-jones
- Amlie E, Havelin LI, Furnes O, et al. Worse patient-reported outcome after lateral approach than after anterior and posterolateral approach in primary hip arthroplasty. A cross-sectional questionnaire study of 1,476 patients 1-3 years after surgery. Acta Orthop 2014;85:463–469. Crossref, Medline, ISI, Google Scholar
- Barrett WP, Turner SE, Leopold JP. Prospective randomized study of direct anterior vs postero-lateral approach for total hip arthroplasty. J Arthroplasty 2013;28:1634–1638. Crossref, Medline, ISI, Google Scholar
- https://www.orthobullets.com/approaches/12020/hip-anterior-approach-smith-petersen
- https://www.orthobullets.com/approaches/12023/hip-posterior-approach-moore-or-southern
- Gilbey, Helen J. PhD*; Ackland, Timothy R. PhD*; Wang, Allan W. MBBS**; Morton, Alan R. EdD*; Trouchet, Therese PGdip (Ot)†; Tapper, Jeff BASc‡. Exercise Improves Early Functional Recovery After Total Hip Arthroplasty. Clinical Orthopaedics and Related Research: March 2003 – Volume 408 – Issue – p 193-200
- Murray M, Brewer B, Zuege R: Kinesiologic measurement of functional performance before and after McKee-Farrar total hip replacement. J Bone Joint Surg 54A:237–256, 1972
- Minor M, Hewett J, Webel R, Dreisinger T, Kay D: Exercise tolerance and disease related measure in patients with rheumatoid arthritis and osteoarthritis. J Rheumatol 15:905–911, 1988.
- Kiran, M., Yadav, A., Johnstone, L., McLeod, G., & Jariwala, A. (2019). Comparative analysis of different total hip replacement implants used in a single health region of the United Kingdom-minimum 15 years follow-up. Acta Orthop Belg, 85(2), 192.
- Wroblewski BM, Siney PD, Fleming PA. Charnley low- frictional torque Arthroplasty. Follow-up for 30 to 40 years. J Bone Joint Surg (Br) 2009 ; 91B : 447-450.
- Keeling, P., Howell, J. R., Kassam, A. A. M., Sathu, A., Timperley, A. J., Hubble, M. J., … & Whitehouse, S. L. (2020). Long-term survival of the cemented exeter universal stem in patients 50 Years and younger: an update on 130 hips. The Journal of Arthroplasty, 35(4), 1042-1047.
- Lee GR, Berstock JR, Whitehouse MR, Blom AW. Recall and patient perceptions of hip precautions 6 weeks after total hip arthroplasty. Acta orthopaedica. 2017 Sep 3;88(5):496-9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5560211/ (last accessed 24.4.2019)
- Barnsley L, Barnsley L, Page R. Are hip precautions necessary post total hip arthroplasty? A systematic review. Geriatric orthopaedic surgery & rehabilitation. 2015 Sep;6(3):230-5. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4536510/ (last accessed 24.4.2019)
- Galea MP, Levinger P, Lythgo N, Cimoli C, Weller R, Tully E, McMeeken J, Westh R. A targeted home-and center-based exercise program for people after total hip replacement: a randomized clinical trial. Archives of physical medicine and rehabilitation 2008;89(8):1442-7.
- Beaulieu, M. L., Lamontagne, M., & Beaulé, P. E. (2010). Lower limb biomechanics during gait do not return to normal following total hip arthroplasty. Gait & posture, 32(2), 269-273.
- Foucher KC, Hurwitz DE, Wimmer MA. Preoperative gait adaptations persist one year after surgery in clinically well-functioning total hip replacement patients. J Biomech 2007;40(15):3432–7.
- Nantel J, Termoz N, Vendittoli PA, Lavigne M, Prince F. Gait patterns after total hip arthroplasty and surface replacement arthroplasty. Arch Phys Med Rehabil 2009;90(3):463–9.
- Belda-Lois, J. M., Mena-del Horno, S., Bermejo-Bosch, I., Moreno, J. C., Pons, J. L., Farina, D., … & Rea, M. (2011). Rehabilitation of gait after stroke: a review towards a top-down approach. Journal of neuroengineering and rehabilitation, 8(1), 1-20.
- https://www.health.gov.au/health-topics/physical-activity-and-exercise/physical-activity-and-exercise-guidelines-for-all-australians




