


Physiotherapists are often asked questions like what are my chances of re-injury? Will I have problems in the future because of this injury? These are important questions for recreational runners through to elite performers. Here we discuss what the chances of re-injury are with common running injuries including strains (hamstring, calf), stress fractures, patellofemoral pain, tendinopathy, ankle sprains and iliotibial band syndrome. It is important to know how the current injury influences the risk of sustaining re-injury to the same area or subsequently another injury to a different area.
In sports such as running and athletics there are commonly implemented strategies, systems or training approaches to reduce the risk of injury. Time out due to injury has numerous social, financial, physical and psychological costs for the individual and those around them. Injuries can be tough to prevent and once it occurs the aim is to minimise the risk of it happening again. There are numerous factors that have been identified which increase risk of injury, one of which is previous injury. A previous injury is a strong risk factor for development of a running related injury (1). So once you have sustained an injury there is typically an increased risk of re-injury (risk of having that injury again) and subsequent injury (a new related injury to a different site).
Subsequent injuries are problematic for the people who sustain them and the professionals who manage rehabilitation from those injuries. Any injury, in spite of treatment, affects tissue integrity in both the short and long term and reduces the capacity for loading. This potentially reduces chronic workloads, and can cause biomechanical or neural pattern changes in running technique which may be related to subsequent injury. Better understanding of subsequent injuries is needed to inform the development of strategies to prevent future injury and the longer term musculoskeletal ill health burden that can arise from them (2).
Soft Tissue Injuries – Muscle Strains
Soft tissue injuries are one such area where there is increased risk of re-injury and /or subsequent injury. The new data on professional players presented here confirm that injured athletes, irrespective of their level of play, can sustain both new injuries and the same injury again and that either type of injury can be dependent upon earlier index injuries. Taken together, these data suggest that related injuries account for 1 in 8 injuries overall and about one third of all subsequent injuries (3). For example injuries to the hamstrings, quadriceps, adductors and calves were associated with a subsequent muscle injury at a different site. Hamstring or adductor injuries were associated with a significant increase in risk of future calf and quadriceps injuries. Quadriceps injuries were significantly associated with an increased risk of calf injuries. Previous calf injury was found to be associated with subsequent quadriceps or hamstring injury risk (3). The length of times in which risk of injury is elevated is variable, with one study suggesting that risk of subsequent or re-injury remains elevated 15 weeks after return to games or full intensity (4).
Patellofemoral Pain
Patellofemoral pain (PFP) or kneecap pain is a common cause of knee pain for runners. With almost 50% of running injuries occurring at the knee, of which almost half (48%) occurring at the patellofemoral joint (5). Prospective studies show that PFP is not self-limiting, with some people reporting persistent symptoms from 5-20 years (6). Notably adolescents with PFP in a 2 year follow up found that 55% still had symptoms (7). At this stage it’s unclear whether there is a relationship between PFP and development of patellofemoral arthritis. Unfortunately some studies suggest that a substantial proportion of people with PFP experience an unfavourable outcome over 12 months, irrespective of treatment. With PFP greater than 2 months duration at baseline is the most consistent predictor of poor outcome. Findings suggest that early management utilising interventions with known efficacy in reducing PFP may enhance outcomes (8).
Stress Fractures
Bone stress injuries (BSI) occur on a continuum of overload to bone; leading to stress reactions and potentially stress fracture. Reported 1-yr incidence rates in competitive track and field athletes have ranged from 8.7% (22) to 21.1% (9, 10). A prior stress fracture is a significant risk factor for sustaining a future stress fracture at the same site (11). Increased risk of subsequent stress fracture can also be related to a number of interconnected factors such as relative energy deficiency, low bone mineral density, high training loads, rapid growth during youth, overscheduling, chronic sleep deprivation and low vitamin D and calcium intake (12). It is important to identify these factors with an initial injury to assist in reducing risk of subsequent injury.
Iliotibial Band Syndrome
ITB syndrome makes up 12 percent of all running-related overuse injuries (13). ITB syndrome is interestingly one injury that doesn’t seem to have an increased risk of recurrence although studies on this are limited. One study reported ITBFS resolution and no recurrence at six months following a 6-week rehabilitation programme (14). As with many of the other injuries discussed there may be an increased risk of subsequent injury due to variables (such as a reduction in running volume) yet this has not been studied in this population.
Tendinopathy
Tendinopathy refers to a series of changes that occurs within a tendon and results in becoming symptomatic and affects the ability to complete functional activities. We have further described tendinopathies in numerous past blogs (here). Tendinopathies can be a long recovery road, with many taking over a year (15). During rehabilitation strength and plyometrics exercises are gradually increased towards the highest levels of tendon load. When someone is returned to full function and no longer has symptoms, they may still not have the structure of a normal tendon but can be considered recovered from the injury (16). Injury recurrence for Achilles tendinopathy has been estimated as 27% in one study (17). A recent study on runners experiencing new achilles tendinopathy found that at 1 year follow up 32% self reported some persisting symptoms. Previous studies have also reported approximately 35%‐60% of patients with chronic AT having persisting symptoms after a follow‐up of 5 years or longer (19-21). The range of variance here is partly explained by the way these injuries are reported, the mixed types of achilles pain diagnoses, levels of function of the individuals and not all have had treatment or best practice treatment.
Additionally many individuals may have resolution of symptoms but not be restored to full capacity, eg they can walk or jog but can’t sprint without symptoms. This incomplete rehabilitation process without reaching higher level loading may be part of the picture for tendinopathy re-injury or ‘flare-ups’ (16).
Ankle Sprains
Ankle sprains and particularly those to the lateral ankle have a high frequency of reinjury after an initial ankle sprain (22). For example, 46% of acute ankle sprains that occurred in volleyball, 43% in American football, 28% in basketball, and 19% in soccer were recurrent injuries (23). Other researchers have identified the proportion of recurrent ankle sprains as 12% to 47% (Table 1).
Table 1 Proportions of All Ankle Sprains Reported as Reinjuries (Source -23)
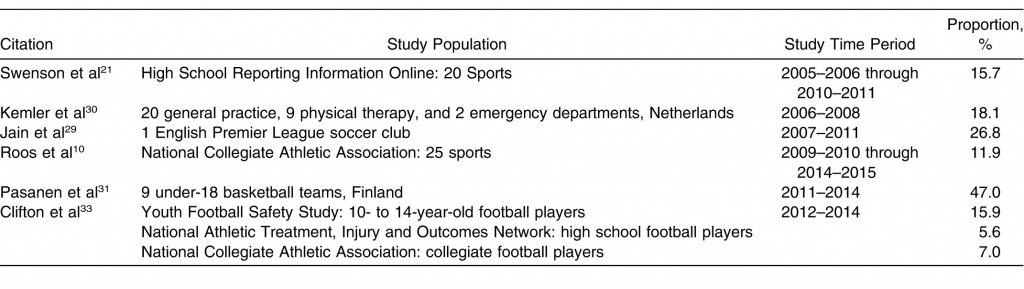
A history of lateral ankle sprain, in particular, has been described as one of the strongest risk factors for a future lateral ankle sprain. Individuals with a history of acute ankle sprain have an approximately 3.5 times greater risk of sustaining another ankle sprain compared with those who have no such history (24). In addition to an increased risk of recurrent strains an estimated 25% of active individuals go on to develop chronic ankle instability (CAI) (25). The lingering ankle instability contributes to ongoing disability and control deficits, which associate with decreased physical activity and quality of life (22).
Implications for Rehabilitation
In most cases of running injuries, sustaining an injury places you at increased risk of having the same injury again or developing a related injury at another site. Appreciating this information and understanding how long risks are elevated, helps individuals, athletes and coaches make informed decisions about returning athletes to sport or running. It also highlights a key feature of why rehabilitation programs need to be robust and take the injured person to high levels of function before returning to full training volume or sport. It is also important to reflect on contributing factors to the initial injury; such as bone mineral density, sleep hygiene, nutrition (eg quantities, Calcium or Vitamin D levels), rapid growth changes, rapid changes in training load, running technique or biomechanical variables, stress or illness.
Addressing these factors alongside a comprehensive rehab plan and gradual return to running can help mitigate risk of re-injury or subsequent injury.

Lewis Craig (APAM)
POGO Physiotherapist
Masters of Physiotherapy
Featured in the Top 50 Physical Therapy Blog
References
- Hulme, A., Nielsen, R. O., Timpka, T., Verhagen, E., & Finch, C. (2016). Risk and Protective Factors for Middle- and Long-Distance Running-Related Injury. Sports Medicine, 47(5), 869–886. doi:10.1007/s40279-016-0636-4
- Finch CF, Cook J, Kunstler BE, et al. Subsequent injuries are more common than Injury Recurrences: an analysis of 1 season of prospectively collected injuries in professional australian football. Am J Sports Med 2017;45:1921–7.
- Toohey, L. A., Drew, M. K., Cook, J. L., Finch, C. F., & Gaida, J. E. (2017). Is subsequent lower limb injury associated with previous injury? A systematic review and meta-analysis. British Journal of Sports Medicine, 51(23), 1670–1678. doi:10.1136/bjsports-2017-097500
- Orchard JW, Chaker Jomaa M, Orchard JJ, et al (2020). Fifteen-week window for recurrent muscle strains in football: a prospective cohort of 3600 muscle strains over 23 years in professional Australian rules footballBritish Journal of Sports Medicine ;54:1103-1107
- van der Heijden, R. A., Oei, E. H., Bron, E. E., van Tiel, J., van Veldhoven, P. L., Klein, S., Verhaar, J. A., Krestin, G. P., Bierma-Zeinstra, S. M., & van Middelkoop, M. (2016). No Difference on Quantitative Magnetic Resonance Imaging in Patellofemoral Cartilage Composition Between Patients With Patellofemoral Pain and Healthy Controls. The American journal of sports medicine, 44, 1172-1178.
- Nimon G, Murray D, Sandow M, et al. (1998) Natural history of anterior knee pain: a 14- to 20-year follow-up of nonoperative management . J Pediatr Orthop;18:118–22.
- Michael SR, Camilla RR, Jens LO, Sten R, Ewa MR (2016). Is knee pain during adolescence a self-limiting condition? Prognosis of patellofemoral pain and other types of knee pain. Am J Sports Med.;44(5):1165–71.
- Collins NJ, Bierma-Zeinstra SM, Crossley KM, van Linschoten RL, Vicenzino B, van Middelkoop M. (2013) Prognostic factors for patellofemoral pain: a multicentre observational analysis. Br J Sports Med.;47:227–33.
- Nattiv, A., Puffer, J. C., Casper, J., Dorey, F., Kabo, J. M., Hame, et al. (2000). Stress fracture risk factors, incidence and distribution: a 3-year prospective study in collegiate runners. Med Sci Sports Exerc, 32(suppl 5), S347.
- Bennell, K. L., Malcolm, S. A., Thomas, S. A., Reid, S. J., Brukner, P. D., Ebeling, P. R., & Wark, J. D. (1996). Risk factors for stress fractures in track and field athletes: a twelve-month prospective study. The American journal of sports medicine, 24(6), 810-818.
- Kelsey JL, Bachrach LK, Procter-Gray E, et al. (2007) Risk factors for stress fractures among young female cross-country runners. Med Sci Sports Exerc.;39(9):1457–63
- Newman P, Witchalls J, Waddington G, et al. (2013)Risk factors associated with medial tibial stress syndrome in runners: a systematic review and meta-analysis. Open Access J Sports Med;4:229–41.
- Fredericson M, Wolf C (2005) Iliotibial band syndrome in runners: innovations in treatment. Sports Med 35, 451–459
- Fredericson MD, Cookingham CL, Chaudhari AM, et al. (2000) Hip Abductor Weakness in Distance Runners with Iliotibial Band Syndrome. Cl J of Sport Med;10(3):169-175.
- Silbernagel KG, Thomeé R, Eriksson BI, Karlsson J. (2007) Continued sports activity, using a pain-monitoring model, during rehabilitation in patients with Achilles tendinopathy: a randomized controlled study. Am J Sports Med;35(6):897–906.
- Silbernagel, K. G., Hanlon, S., & Sprague, A. (2020). Current clinical concepts: conservative management of Achilles tendinopathy. Journal of athletic training, 55(5), 438-447.
- Gajhede-Knudsen M, Ekstrand J, Magnusson H, Maffulli N. (2013) Recurrence of Achilles tendon injuries in elite male football players is more common after early return to play: an 11-year follow-up of the UEFA Champions League injury study. Br J Sports Med;47(12):763–768.
- Lagas, I. F., Fokkema, T., Bierma‐Zeinstra, S. M., Verhaar, J. A., van Middelkoop, M., & de Vos, R. J. (2020). How many runners with new‐onset Achilles tendinopathy develop persisting symptoms? A large prospective cohort study. Scandinavian journal of medicine & science in sports, 30(10), 1939-1948.
- van der Plas A, de Jonge S, de Vos RJ, et al. (2012) A 5‐year follow‐up study of Alfredson’s heel‐drop exercise programme in chronic midportion Achilles tendinopathy. Br J Sports Med;46(3):214‐218
- Silbernagel KG, Brorsson A, Lundberg M. (2011)The majority of patients with Achilles tendinopathy recover fully when treated with exercise alone: a 5‐year follow‐up. Am J Sports Med;39(3):607‐613.
- Paavola M, Kannus P, Paakkala T, Pasanen M, Jarvinen M. (2000) Long‐term prognosis of patients with achilles tendinopathy. An observational 8‐year follow‐up study. Am J Sports Med;28(5):634‐642.
- Gribble PA, Bleakley CM, Caulfield BM, et al. (2016) Evidence review for the 2016 International Ankle Consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sports Med.;50(24):1496–1505
- Attenborough AS, Hiller CE, Smith RM, Stuelcken M, Greene A, Sinclair PJ. (2014) Chronic ankle instability in sporting populations. Sports Med;44(11):1545–1556.
- Kucera KL, Marshall SW, Wolf SH, Padua DA, Cameron KL, Beutler AI. (2016) Association of injury history and incident injury in cadet basic military training. Med Sci Sports Exerc.;48(6):1053–1061.
- Herzog, M. M., Kerr, Z. Y., Marshall, S. W., & Wikstrom, E. A. (2019). Epidemiology of ankle sprains and chronic ankle instability. Journal of athletic training, 54(6), 603-610.



