


Ischiofemoral Impingement Syndrome
Anatomy & Aetiology
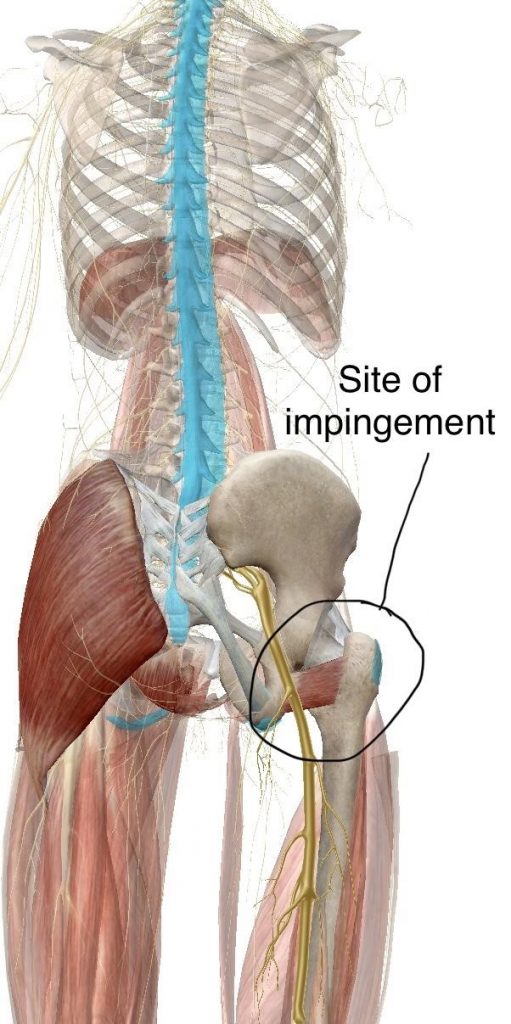
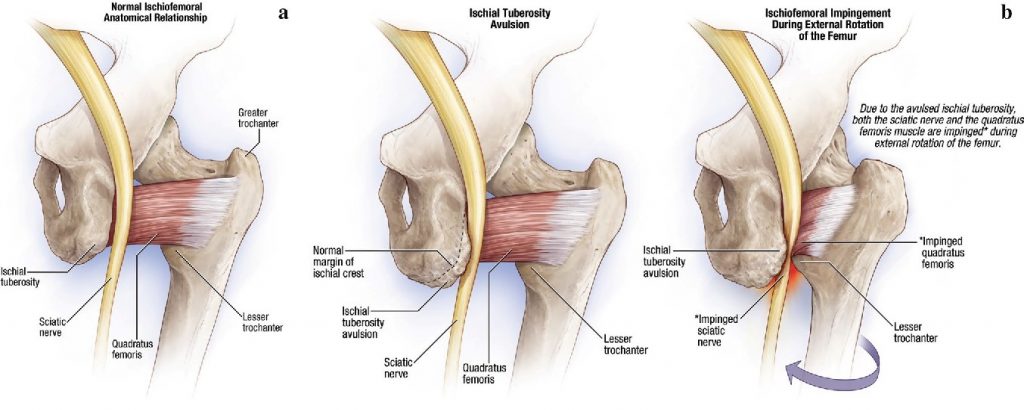
The Quadratus femoris is a flat, quadrilateral muscle arising from the lateral border of the ischial tuberosity (AKA sit bones) and inserting into the quadrate tubercle and linea quadrata of the femur (Inside of the thigh bone): it is therefore at risk of impingement if the ischiofemoral space is narrowed 6.
Originally described in a case report by Johnson 2 in 1977 – Ischiofemoral Impingement was described as hip pain persisting after hip replacement surgery from pinching of the quadratus femoris muscle and sciatic nerve between the lesser trochanter of the femur and the ischial tuberosity (commonly known as sits bone) as pictured above 3.
Since then, Ischiofemoral Impingement Syndrome has been identified as an uncommon potential cause of hip, buttock &/or groin pain, more commonly seen in older women post hip/pelvic trauma or hip surgery 1-6. Symptoms commonly include hip pain that can radiate towards the knee if the sciatic nerve is involved. Pain will often worsen with movements such as hip extension, adduction and/or external/internal rotation that compress or impinge the irritated quadratus femoris muscle and/or sciatic nerve and surrounding tissue 7. Additional symptoms commonly reported include snapping or locking sensations in the hip joint 5.
Diagnosis
Ischiofemoral Impingement Syndrome is quite an uncommon diagnosis for hip and groin pain – thus it is important that more common conditions like those listed below, are ruled out by a qualified Medical Professional and Physiotherapist before considering it as a diagnosis:
- Lumbar disc disease
- Spinal stenosis
- Bursitis
- Osteoarthritis
- Rheumatoid arthritis
- Cancer
- Inguinal hernias
- Inguinal lymphadenopathy
- Menstrual conditions
- Urinary tract problems
- Pelvic inflammatory diseases
- Femoroacetabular impingement/piriformis syndromes 5
Source: Spencer-Gardner et al., 2017
The current gold standard for diagnosis of Ischiofemoral Impingement Syndrome is a combination of the following:
- MRI findings of reduced ischiofemoral space (<15mm),
- MRI findings of swelling/atrophy of the quadratus femoris muscle with
- Clinical findings of pain in the hip, buttock and/or groin 1,5
Whilst narrowing of the ischiofemoral space is predictive of Ischiofemoral Impingement 5, just one or two of the above findings are not adequate for a clear diagnosis of Ischiofemoral Impingement Syndrome as narrowing of the ischiofemoral space and changes in the quadratus femoris muscle have been seen patients without hip or groin pain 1.
Additional structures such as the Psoas and Hamstring muscles can also be affected by Ischiofemoral Impingement as they both insert/arise from the affected region 7. Thus Chronic Bursitis of the Psoas or Hamstrings may indicate, and even lead to Ischiofemoral Impingement 7.
Treatment
Due to the rarity of Ischiofemoral Impingement, treatment for the condition has varied on a case by case basis. However, conservative treatment is broadly recommended as a first line approach to resolving the condition. Current conservative treatment strategies in the literature for Ischiofemoral Impingement Syndrome include:
- Nonsteroidal anti-inflammatory drugs and Gabapentin for pain associated with quadratus femoris muscle and sciatic nerve irritation 4
- Heat, Ultrasound, and Interferential current therapies applied around the hip area 4
- An individually prescribed exercise program by a Physiotherapist targeting muscles like the quadriceps femoris, piriformis in order to adequately reduce pain and increase the range of motion in the hip joint. 4
- CT-guided steroid and local anesthetic injection around the QFM may provide pain relief 5
Surgical intervention in order to correct/decompress anatomical pathology such as that first described by Johnson in 1977 is reserved for cases that do not respond to conservative therapy 2,5,7. Potential surgical interventions include excision of the lesser trochanter (in those experiencing pain post hip surgery), and more recent/popular peri-articular endoscopic decompression around the hip 2,7. Further research is required to better understand Ischiofemoral Impingement Syndrome – its causes, at risk populations and optimal management strategies- both conservative and surgical. As this condition is not yet widely recognised and understood.
If you are experiencing abnormal pain in the groin, hip or buttock exaggerated with moving the leg into extension and adduction – seek the help of a qualified Physiotherapist and/or Medical Practitioner.

Oliver Crossley (APAM)
POGO Physiotherapist
Featured in the Top 50 Physical Therapy Blog
References
Singer, Adam D., Ty K. Subhawong, Jean Jose, Jonathan Tresley, and Paul D. Clifford. “Ischiofemoral impingement syndrome: a meta-analysis.” Skeletal radiology 44, no. 6 (2015): 831-837
Johnson, K. A. “Impingement of the lesser trochanter on the ischial ramus after total hip arthroplasty. Report of three cases.” JBJS 59, no. 2 (1977): 268-269
Spencer-Gardner, Luke, Asheesh Bedi, Michael J. Stuart, Christopher M. Larson, Bryan T. Kelly, and Aaron J. Krych. “Ischiofemoral impingement and hamstring dysfunction as a potential pain generator after ischial tuberosity apophyseal fracture non-union/malunion.” Knee Surgery, Sports Traumatology, Arthroscopy 25, no. 1 (2017): 55-61
Lee, Soyoung, Inhwan Kim, Sung Moon Lee, and Jieun Lee. “Ischiofemoral impingement syndrome.” Annals of rehabilitation medicine 37, no. 1 (2013): 143
Tosun, Ozgur, Oktay Algin, Nadir Yalcin, Nurdan Cay, Gokhan Ocakoglu, and Mustafa Karaoglanoglu. “Ischiofemoral impingement: evaluation with new MRI parameters and assessment of their reliability.” Skeletal radiology 41, no. 5 (2012): 575-587.
Ali, Adam Mohsan, Duncan Whitwell, and Simon J. Ostlere. “Case report: imaging and surgical treatment of a snapping hip due to ischiofemoral impingement.” Skeletal radiology 40, no. 5 (2011): 653-656.
Stafford, G. H., and R. N. Villar. “Ischiofemoral impingement.” The Journal of bone and joint surgery. British volume 93, no. 10 (2011): 1300-1302.






