


Sports Hernia

Prevalence
Sports hernia has been described as the most common cause of chronic groin pain in athletes (3). Sports hernias, in fact, make up 5-7% of all injuries in sports such as soccer, ice/field hockey, tennis and Australian rules football (3). They are more commonly found in men and occur during athletic activities that involve cutting, pivoting, kicking and sharp turning (3). Although it’s high prevalence, sports hernia remains to be one of the most poorly understood and defined problem with the human body with limited research surrounding it (3)(3).
Risk Factors and Cause
Factors identified that put an individual at risk of developing a sports hernia include reduced hip movement (range of motion), poor muscle balance around the pelvis, limb length discrepancy and an unstable pelvis (4).
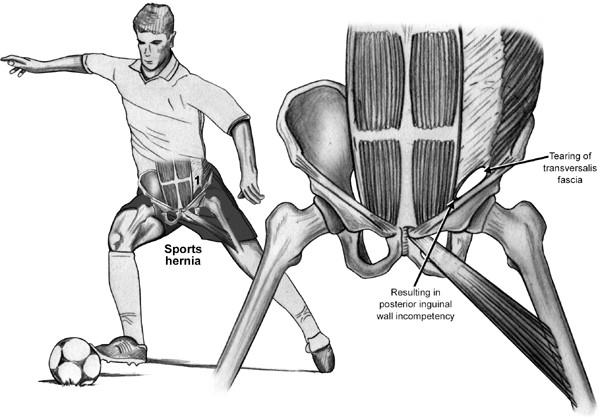
Unlike other sources of groin pain, the sports hernia usually presents without a sudden traumatic event (3). Research states sports hernia is likely caused by excessive or frequent shear forces applied to the lower abdomen (posterior inguinal wall) and the front of the pelvis (symphysis pubis disc) (3). These shear forces are a result an abnormal balance of hip adductor and abdominal muscle activation (3). The pain experienced with the condition is not usually felt at rest and is often associated with inner thigh (adductor tendon pain) on both sides (bilateral) (3).
Diagnosis
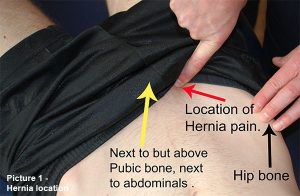
Diagnostic factors include tenderness felt when pressure is applied over a muscle attachment (lower rectus) to the pubic bone (3). In most cases, pain is experienced when resisting pressure on the inner thigh (resisted hip adduction). Some clients can feel an impulse when applying some pressure to the affected area while coughing (3).
Management
Like many conditions, there are operative and nonoperative approaches to management. The conservative approach typically involves 6-8 weeks of rest followed by progressive inner thigh strengthening and stretching.The final stage involves sports-specific or functional tasks with a gradual return to full activities (3). Other conservative methods include anti inflammatory medications and steroid injections (3). Traditional conservative management of sports hernia, however, has low success rates (3). If there is little to no improvement after 3 months of the traditional method, then operative options are explored (3). Research suggests that while many other types of groin pain can be managed conservatively – sports hernias rarely improve without a surgical intervention (3).
The two most effective surgical methods are the open and the laparoscopic approach (3)(3)(4). These reinforce the abdominal muscles and/or fascia near the inguinal ligament (3). Success rates vary between 63-97% with either of the two techniques (3). It is argued that both laparoscopic and open repair techniques are as effective as each other, however research suggests that the laparoscopic approach enables the client faster rehabilitation progression and therefore an earlier return to sport or physical activity (3). In addition to these methods, a surgical release of a portion of the inner thigh (adductor muscles) from the pubic bone has been found to help improve the balance between the clients abdominal and inner thigh muscle forces (3).
Post-op Rehabilitation
Following surgery, rehabilitation is required for the client to return to full exercise or physical activity. The principles of rehabilitation are essentially to:
- Remove or reduce risk factors, causes and compensatory strategies
- Implement core stabilisation exercises
- Improve motor control and strength around the pelvis, with focus on single-leg positions (3).
Research states that post-surgical return to sport for open repairs was 13.1 weeks, compared to 4.5 weeks for those that underwent laparoscopic repairs (3). However, this is dependent on the client outcome, measurements and activity level assessments (3). Therefore, it is vital that progression through the rehabilitation program is safely monitored and the correct objective measures are undertaken.
A strong focus of rehab is core activation and control with coordination of inner thigh (adductor) motor control and strength (3).
Core progression (3)(4)
 1st stage (week 1-2)
1st stage (week 1-2)
- Initial core exercises involve a static contraction of the deep abdominal muscles with focus of correct activation
2nd stage (week 2-3)
- Addition of limb movements to challenge the core muscles in less stable positions.
- Traditional sit-ups
3rd stage (week 3-4)
- Progress to more functional positions such as single leg stance with an external pressure applied or a distraction being incorporated
4th stage (week 4-6)
- Progress to dynamic positions with controlled side-to-side (lateral) movement and the addition of a skateboard
Strength training is another focus for post-op rehabilitation. Research suggests a pattern of squats and lunges that are progressed to single-leg squats and multi-directional lunges are effective at restoring optimal hip and abdominal muscle ratios, power and coordination (4). These exercises also stabilise the pelvic ring in dynamic postures – reducing the risk of re-injury.
Strength progression (3)
 Week 1
Week 1
- Isometric abdominal and hip exercises
Week 2
- Progress to active exercises without resistance
Week 3
- Add resistance-bands or hand-held small weights to the hip and abdominal exercises
Week 4
- Progress the resistance/weight appropriately and begin upper body exercises with light resistance
Week 5
- Progress resistance for abdominal exercises and begin functional tasks with a gradual return to sports or physical activity
Week 6
- Unrestricted exercise training, return to competitive sport if appropriate
Another risk factor targeted with rehabilitation is hip movement (range of motion),movement of the lumbar spine, general strengthening and returning to exercise (3).
Mobility/exercise progression (3)(4).
Week 1
- Walking at 5km/h is encouraged and is increased by 5 minutes per day
Week 2

- Stationary cycling is another exercise to improve hip movement and strength and can be added to the clients program two weeks post-operation
Week 3
- Progress to resistance-band hip exercises are added and walking pace can increase to a jog or swim
Week 4
- Forward running, no cutting, pivoting or turning
Week 5
- Sprinting, multi-directional running
- Light ball skills and kicking if appropriate
Week 6
- Unrestricted exercise training, return to competitive sport if appropriate

Conclusion
Sports hernia is a groin disruption injury that is believed to be caused by pelvic instability, however remains to be poorly understood and difficult to diagnose (3)(4). Diagnosis is via a thorough assessment of the client’s history, a physical examination and imagery findings however none of which is reliable in isolation (4). It is most common in sports involving cutting, pivoting or kicking with risk factors such as reduced hip movement, poor muscle balance, uneven leg length and an unstable pelvis. If conservative management lasting at least 3 months fails, then a surgical approach and appropriate post-op rehabilitation is encouraged. Laparoscopic repairs are the preferred method due to their faster recover time resulting in the client returning to the physical activity or sport they love sooner.

Alec Lablache (APAM)
POGO Physiotherapist
Featured in the Top 50 Physical Therapy Blog
References
- Buckingham, M. (n.d). Sports hernia symptoms, tests and treatment. Realbuzz. Retrieved from https://www.realbuzz.com/articles-interests/running/article/sports-hernia-symptoms-tests-and-treatment/
- Caudill, P., Nyland, J., Smith, C., Yerasimides, J., & Lach, J. (2008;2007;). Sports hernias: A systematic literature review. British Journal of Sports Medicine, 42(12), 954-964. doi:10.1136/bjsm.2008.047373
- Diaco, D. S., Diaco, J. F., & Lockhart, L. (2005). Sports hernia. Operative Techniques in Sports Medicine, 13(2), 68-70. doi:10.1053/j.otsm.2004.09.004
- Garvey, J. F. W., Read, J. W., & Turner, A. (2010). Sportsman hernia: What can we do? Hernia, 14(2), 17-25. doi:10.1007/s10029-009-0611-1
- Surgeryrome.com. (2018). What is a sports hernia. Retrieved from https://www.surgeryrome.com/what-is-a-sports-hernia/
- Oxfordherniaclinic.com. (2016). Sports hernia surgery. Retrieved from https://www.oxfordherniaclinic.com/types-of-hernia/sports-hernia-surgery
- Trackactive.co. (2017). Exercises. Retrieved from https://app.trackactive.co/practices/1011/exercises






