


Headaches – More than just a pain in the brain!

Headache disorders are one of the most common disorders of the nervous system, estimated to affect almost 50% of the adult population at least once every year, globally (1). Despite this prevalence, the World Health Organisation recognises that headaches have been traditionally underestimated, under-recognised and under-treated worldwide (1). Substantial burden is placed on those suffering from headaches, not only due to their recurrent and painful nature. In 2013, the Global Burden of Disease Study found migraines to be the sixth highest cause of worldwide years lost, while headache disorders collectively placed third highest (1, 2). Like many chronic conditions, the long term effects of headache disorders can be disabling. Anxiety and depression, for example, are significantly more prevalent in those with migraines when compared to healthy individuals (1).
Classification of Headaches
A headache is a symptom that can be attributed to a primary clinical condition, such as a migraine, or may be secondary to another underlying issue, like trauma to the head or neck.
The International Classification of Headache Disorders, 3rd edition, (ICHD-3) is the most recognised, hierarchical classification systems outlining more than 200 headaches disorder presentations (2). Headaches are categoried into three broad groups; primary, secondary and cranial neuropathies and neuralgias. Within these categories, 14 further sub-categories are identified, each with explicit diagnostic criteria. Figure 1 provides a summarised version.
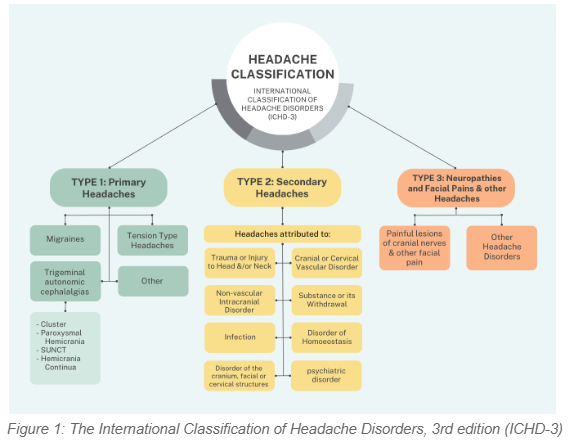
These 14 sub-groups further outline multiple levels of disorders denoted by sequential numbering, allowing for an extremely specific and detailed diagnosis. As a practitioner, you may not need this detailed classification system for common presentations such as migraines and tension-type headaches; however, it proves useful in circumstances where the diagnosis is uncertain (2).
Primary vs Secondary Headaches
Primary headaches are the most common type of headache, accounting for 90% of all headaches disorders (3). They are typically chronic in nature, and include migraines, tension-type headaches, trigeminal autonomic cephalalgias and other causes whereby the headache is the disease itself.
Secondary headaches, accounting for the other 10% of headache types, are a result of varying underlying causes, inclusive of infectious, inflammatory, vascular, traumatic or structural origins (4).
It is crucial clinicians can accurately differentiate primary and secondary headache syndromes, as failure to do so significantly worsens morbidity and mortality (4).
Some useful green and red flags have been outlined below to assist clinicians in identifying red flags that may suggestive of a secondary headache, and green flags that assist in the recognition of frequently “benign” primary headaches.
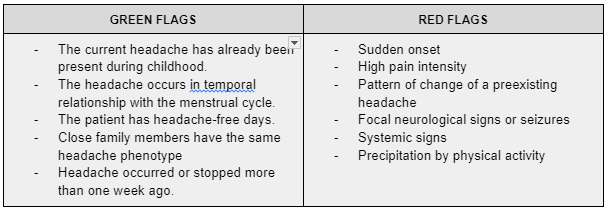
Table 1 Green & red flags for primary and secondary headache discrimination in clinical practice (4)
In the case of a suspected secondary headache, the ‘SNNOOP10 list” has been proposed as a useful checklist that allows practitioners to identify more dangerous clinical features of secondary headache disorders (5). They are as follows:
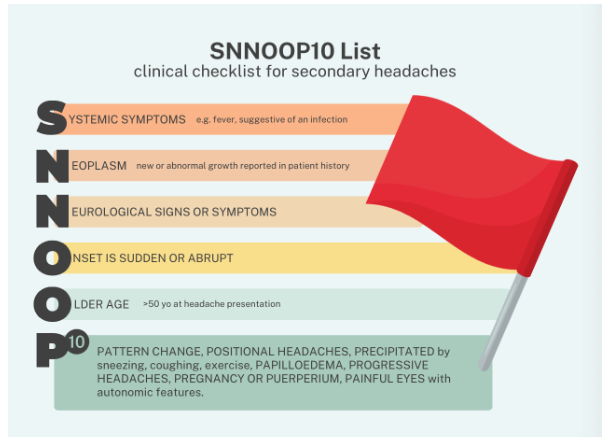
Figure 3 SNNOOP10 List adapted from the paper ‘Red and Orange flags for secondary headaches in clinical practice’ (5)
For more details on SNNOOP10 as well as red and green flags for secondary headaches, Wijeratne et al., published a fantastic article in the National Library of Medicine titled, “Secondary headaches – red and green flags and their significance for diagnostics”.
Common Headache Disorders
Migraine
There are two major types of migraine
- Migraines without Aura – characterised by headache with specific features and associated symptoms (e.g. nausea, vomitting)
- Migraines with aura – characterised primarily by transient focal neurological symptoms, that usually precede or sometimes accompany the headache (e.g. flashes of light, blind spots, or tingling in the hands or face).
Both types are primary headache disorders, with migraines without aura being typically more common than those with aura (2). Aura has been likened to a ‘warning sign’ of a migraine. Migraines are caused when a mechanism deep within the brain is activated, releasing pain-producing, inflammatory substances that affect the nerves and blood vessels of the head (1).
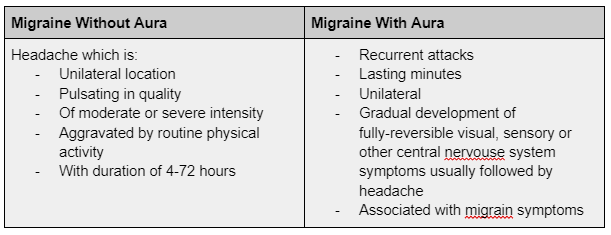
Table 2 Clinical characteristics of the two major types of migraines
Menstrual headaches
Migraines related to menstruation are most commonly without aura, however, may also include aura, and may be the result of endometrial bleeding or the related hormonal changes a woman undergoes throughout their cycle. Menstrual migraines are considered a primary headache disorder and affect 60% of female migraine sufferers (4).
Tension-type Headaches
Tension-type headaches (TTH) are the most common primary headache disorder. This type includes episodic and chronic presentations, whereby episodic TTH (occuring on <15 days per month) affect more than 70% of some populations (1). This type of primary headache affects three women to every two men, with onset typically occurring during teenage years. TTH can last anywhere between minutes to days and is often described as a band-like pressure or tightness around the forehead and temples, occasionally involving the neck. The exact cause, or mechanism of TTH is not known, but it is hypothesises that both peripheral pain and central pain mechanisms are involved depending on the patients specific subtype of TTH.
Diagnostically, it can be challenging to differentiate between TTH and mild forms of migraine without aura due to the fact that patients with frequent headaches are often suffering from both (2).
Cluster Headaches
Another primary headache disorder, far less common than that of migrains or TTH, affecting less than 1 in 1000 adults (1). Onset usually occurs in individuals in their 20s or older, and is more common in men than women. Cluster headaches are described as frequently recurring (sometimes several times a day), extremely severe but fleeting headaches around one eye, typically causing tearing and redness of the affected eye and occasionally the eyelid may droop, along with a runny or blocked nose on the affected side.
Post-traumatic Headaches
Headaches attributed to trauma or injury to the head and/or neck are one of the most common secondary headache disorders (2) and include headaches resulting from head and/or neck trauma, whiplash and craniotomies. This is separate to cervicogenic headaches.
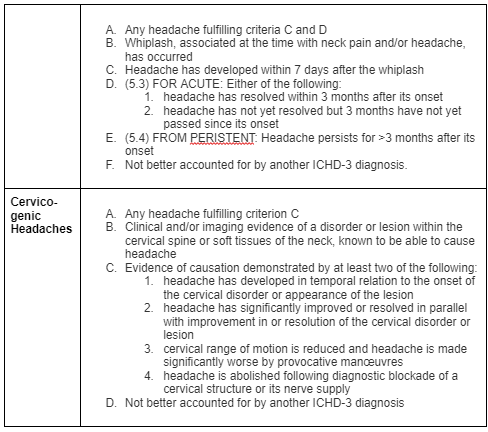
Cervicogenic Headache
A cervicogenic headache result from a disorder of the cervical spine and its bony, disc and/or soft tissue components that is usually (but not always) accompanied by neck pain (2). It is a secondary headache, falling under the subtype 11. Disorder of the cranium, facial or cervical structures. Cervicogenic headaches can be discriminated from migraine and TTH headaches by the following:
- Side-locked pain
- Provocation of typical headache by palpation on the neck muscles
- Provocation of typical headache by head movements
- Posterior-to-anterior radiation of pain
However, it is worth noting these features aren’t unique to cervicogenic headaches and they do not necessarily confirm a causal relationship.
If you’re struggling with headaches, we are here to help. An accurate assessment, diagnosis, treatment and comprehensive management plan will help you treat and manage your headaches so you can get back to doing the things you love and reach your Physio Finish Line. To book in with one of our physiotherapists, call our reception team on
(07) 5572 0133 or book online here
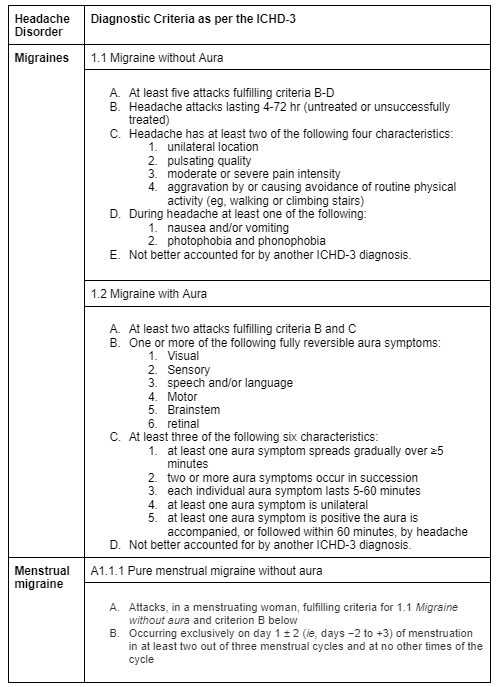
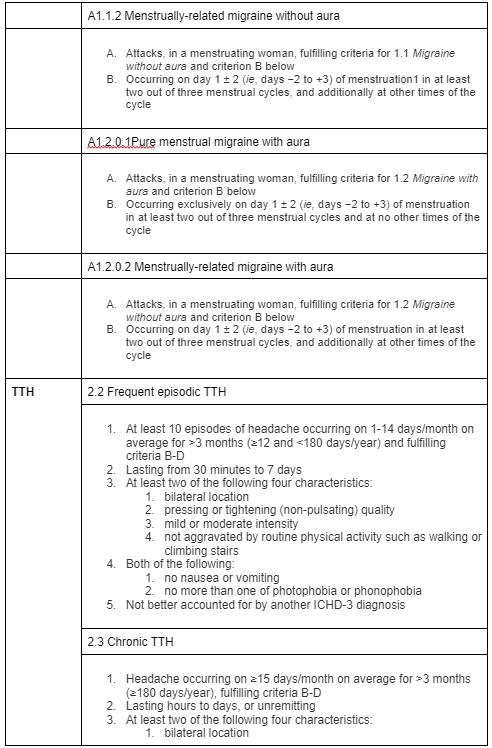
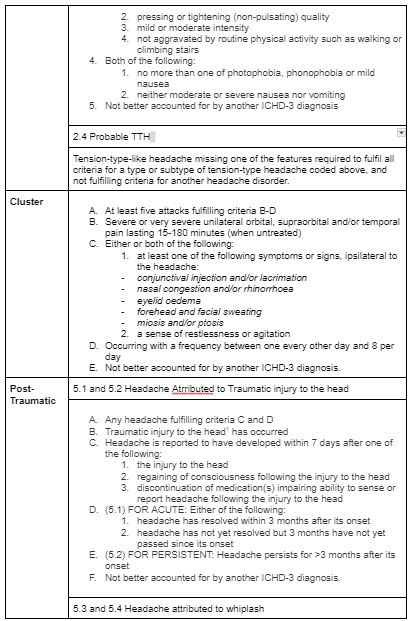
For the ICHD-3 diagnostic criteria for each of the headaches outlined above, see appendix 1. For more details on the ICHD-3, it can be found online for free or use this link.
APPENDIX
Diagnostic criteria for Headaches outlined above

Sarah Ellis B. Exercise Science (APAM)
POGO Physiotherapist
Doctor of Physiotherapy
Book an Appointment with Sarah here
References
- Headache disorders. (n.d.). World Health Organisation. https://www.who.int/en/news-room/fact-sheets/detail/headache-disorders
- Ihsclassification. (2016). ICHD-3 The International Classification of Headache Disorders 3rd edition. ICHD-3 the International Classification of Headache Disorders 3rd Edition. https://ichd-3.org/
- Coni, R., Bone, H., & Bone, R. C. and H. (2023, January 15). Headache classification. Life in the Fast Lane • LITFL. https://litfl.com/headache-classification/
- Wijeratne, T., Wijeratne, C., Korajkic, N., Bird, S., Sales, C., & Riederer, F. (2023). Secondary headaches – red and green flags and their significance for diagnostics. ENeurologicalSci, 32, 100473. https://doi.org/10.1016/j.ensci.2023.100473
- Do, T. P., Remmers, A., Schytz, H. W., Schankin, C., Nelson, S. E., Obermann, M., Hansen, J. M., Sinclair, A. J., Gantenbein, A. R., & Schoonman, G. G. (2018). Red and orange flags for secondary headaches in clinical practice. Neurology, 92(3), 134–144. https://doi.org/10.1212/wnl.0000000000006697





