


Red Flags for Spinal Pathology

Low back pain is a hugely burdensome issue in Australia but just how huge is this burden you may ask…back pain costs the Australian taxpayer approximately $4.8Billion per year. It has been estimated to reduce the Australian GDP by $3.2Billion yearly and it is the most common reason to keep older Australians (45-64) out of the workforce. These large numbers are in part due to the huge prevalence of low back pain in the community. Approximately 25% of the population will suffer low back pain on any one day whilst 50% has likely suffered it in the past month. Think about being in a room of 10 people, 2-3 of them likely have back pain today and 5 or so have had it in the past month (4). That’s a lot!
If such high numbers of people suffer from lower back pain then it is important for clinicians (physio’s, doctors, allied health) to be able to identify when a client is suffering from something more serious. In this blog I am going to unpack Red Flags in Spinal Pathology; what they are, why they’re important and detail a new article that has created increased consensus on the subject.
What is a Red Flag?
One major role of physiotherapists as first contact practitioners is to assess, diagnose and determine further risk to patients presenting in our clinics. Often we need to assess whether further medical imaging is indicated or whether we need to refer this patient to their GP or potentially even the emergency department.
When assessing a patient with spinal related pain, one thing physiotherapists look for is “Red Flags”. These are signs and symptoms that raise suspicion of serious spinal pathology. When health professionals talk about Signs and Symptoms, a sign is something we can observe (swelling, reduced range of motion) whereas a symptom is something a patient reports to us (back pain, nausea). The presence of a singular Red Flag is generally not a huge cause for concern in most cases, as we know Red Flags have more value when used in combination. A thorough history taking and physical examination must also occur to ensure a clear clinical picture is obtained (1).
A new framework
A research paper was published in 2020 to establish an international framework for the identification of red flags. This is because “163 signs and symptoms have been reported as red flags, including 119 symptoms from the individual’s history and 44 signs from the physical examination”. This is an astronomical number of complaints for a therapist to be on the lookout for, thus the paper aimed to simplify the evidence and bring some clarity to the identification of red flags (1).
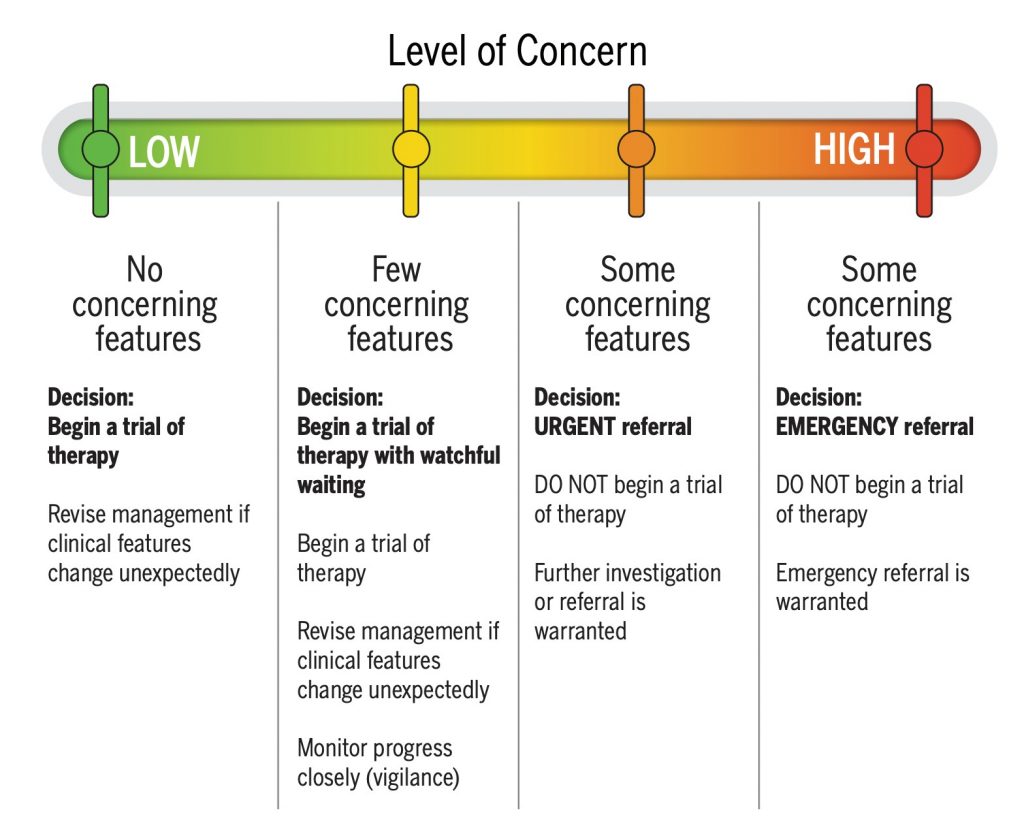
Image: Decision tool for early identification of potential serious spinal pathology,
Shown above is the author’s clinical decision making tool. This is to help clinicians when they do identify serious spinal pathologies to:
- Determine their level of concern
- Decide on a clinical action
- Consider the pathway for emergency or urgent referral
What is a serious spinal pathology?
In most cases, even though they are experiencing pain, patients are at low risk and our assessment in itself is therapy. A thorough assessment allows patients to know their pain is not from a serious cause and allow them to commence therapy, restart the activities they love or have the therapist provide alternate options in the interim.
In a low volume of cases (and I mean very low) there is serious cause for concern when someone presents with low back pain to a physio clinic. When we discuss serious spinal pathologies, we are generally talking about the following conditions Cauda Equina Syndrome (CES), Spinal Fractures (osteoporotic & traumatic), Spinal Malignancy, Spinal Infection.
The aforementioned paper details the prevalence of each of these pathologies:
- Cauda Equina Syndrome (CES); between 0.002%-0.04%
- Spinal Fractures
- Osteoporotic; between 0.7%-11% (depending on the care setting)
- Traumatic; <1%
- Spinal Malignancy; 0.0%-7% (again depending on the care setting)
- Spinal Infection; 0.01%-1.2%
As you can see, these numbers are quite low, suggesting there’s a pretty low chance that someone presenting to see a physiotherapist has a serious spinal pathology. The care setting (e.g. emergency department versus physiotherapy clinic) also changes these statistics. For example, the larger range is osteoporotic fracture prevalence is due to the presence of higher numbers presenting to an emergency department (7-11%) compared with primary care settings (0.7-4.5%). (1)
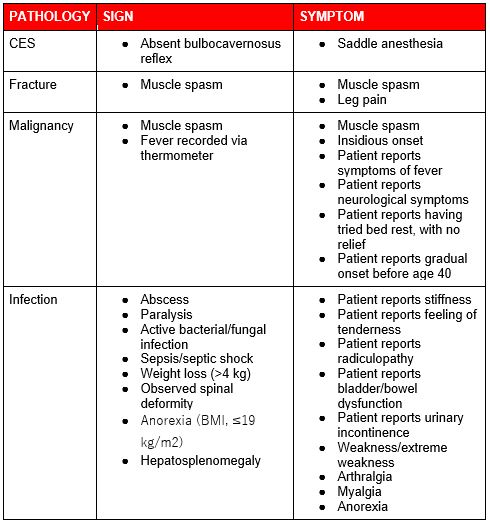
Red Flags for specific conditions
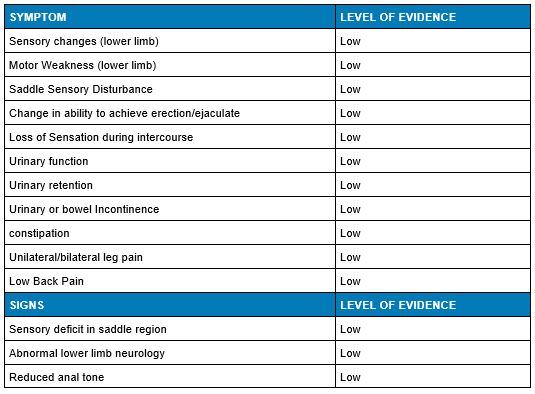
Cauda Equina Syndrome (CES)
This syndrome is most commonly associated with a disc prolapse however any space occupying lesion has the potential to lead to CES. The cauda equina (which is Latin for ‘horses tail’) is where the spinal cord terminates, it stops being a solid structure and instead spreads into 20 nerve roots. Treatment of CES needs to be extremely urgent to prevent long-term neurological deficits from occurring such as ongoing bladder, bowel and sexual dysfunctions. If suspected, an emergency MRI is needed (1,2).
Risk factors for CES include; herniated vertebral disc, lumbar spinal stenosis and spinal surgery (1).
Read more about Cauda Equina Syndrome in this detailed blog post.
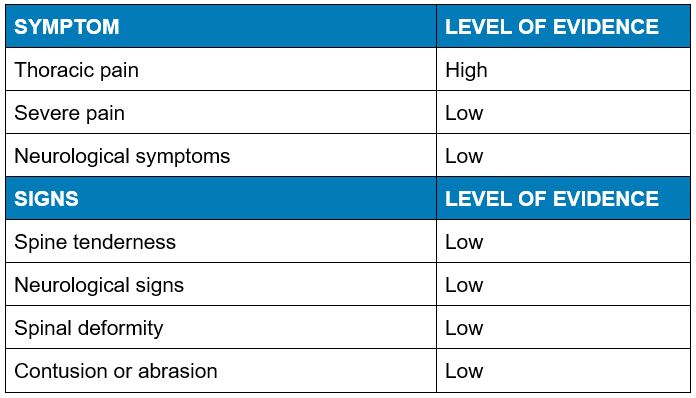
Spinal Fracture
Spinal fractures are the most common occurring serious spinal pathology and the most likely presentation within a physiotherapy clinic. Fractures may be caused from a trauma, such as a fall, as well as fracture due to insufficiency of bone (normal stress on weak bone). These patients will likely present with severe pain in the thoracolumbar region which has often occurred after a fall or lifting in a spinally flexed position. Often the pain is localised to the area of the fracture and is tender to palpate (1).
Risk factors for a spinal fracture include; history of osteoporosis, corticosteroid use (esp. >3 months use), severe trauma, female, older age, previous spinal fracture, as well as low level of evidence for a history of falls and previous cancer as risk factors (1).
Whilst insufficiency fractures are commonly thought to occur in the older populations they can also be suffered by young people. Risk increases with a history of excessive alcohol consumption (>3 drinks/day), Vitamin D deficiency, diabetes, smoking, long-term corticosteroid use (1).
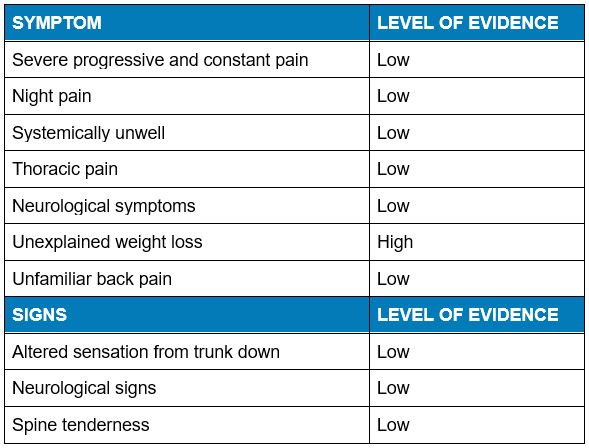
Spinal Malignancy
When cancer lesions spread to the spine (metastasise), it is known as spinal malignancy. Commonly this occurs in the bone (metastatic bone disease) and the spine is one of the commonly affected sites when it does occur. Breast, prostate, lung, kidney and thyroid cancers are the types most common to cause metastatic bone disease (1).
The risk factor for spinal malignancy is a past history of cancer which is supported by a high level of evidence.
Spinal Infection
The vertebrae, intervertebral discs and paraspinal tissues may become infected for a range of reasons. Spinal infection can result in dire complications, such as paralysis and death, when not treated adequately. Whilst presence of a fever seems like an obvious red flag for infection, only about 50% of people with spinal infection present with a fever (3).
The risk factors for developing a spinal infection include; immunosuppression (diabetes, HIV/AIDS, long term steroids plus more), invasive surgery, IV drug use, history of tuberculosis, social and environmental factors, recent infection.
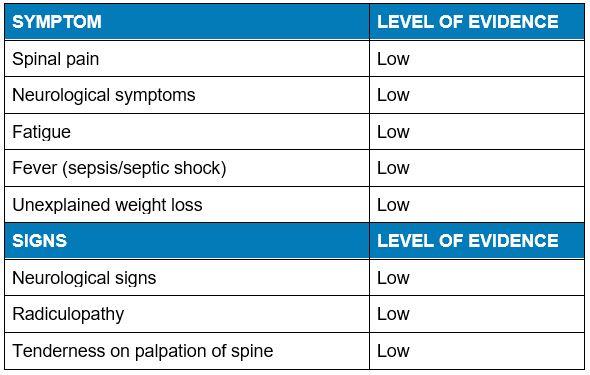
What isn’t a red flag?
Almost equally as important to identify is a consensus on signs and symptoms that are not considered to be red flags. The benefit of the new consensus article evaluating evidence on red flags is that it was also able to list the signs and symptoms that have no evidence in relation to red flags. Listed in the table below are the non-red flags.
Conclusions
This 2020 research paper has effectively summarised and brought together a wide ranging group of signs and symptoms in a clear and concise manner to establish a framework for therapists to assess and appropriately manage serious pathologies in low back pain populations. Interestingly, many of the signs and symptoms that are thought of as red flags have only low levels of evidence.
Importantly it is pertinent to recognise that the large majority of clients presenting to a physio clinic for treatment of their low back pain are at low statistical odds of having a serious spinal pathology. The prevalence of one red flag does not always warrant concern however when multiple red flags are combined they hold more clinical value. It is important for clinicians to be able to stratify risk and proceed accordingly.

James Gardiner
POGO Physiotherapist
Book an Appointment with James here.
Featured in the Top 50 Physical Therapy Blog
References
- Finucane, L. M., Downie, A., Mercer, C., Greenhalgh, S. M., Boissonnault, W. G., Pool-Goudzwaard, A. L., Beneciuk, J. M., Leech, R. L., & Selfe, J. (2020). International framework for red flags for potential serious spinal pathologies. Journal of Orthopaedic & Sports Physical Therapy, 50(7), 350-372. https://doi.org/10.2519/jospt.2020.9971
- Berg EJ, Ashurst JV. Anatomy, Back, Cauda Equina. [Updated 2020 Aug 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513251/
- Lener S, Hartmann S, Barbagallo GMV, Certo F, Thomé C, Tschugg A. Management of spinal infection: a review of the literature. Acta Neurochir (Wien). 2018 Mar;160(3):487-496. doi: 10.1007/s00701-018-3467-2. Epub 2018 Jan 22. PMID: 29356895; PMCID: PMC5807463.
- Buchbinder, R., van Tulder, M., Öberg, B., Costa, L. M., Woolf, A., Schoene, M., … Woolf, A. (2018). Low back pain: a call for action. The Lancet, 391(10137), 2384–2388. doi:10.1016/s0140-6736(18)30488-4






