


The elbow is the second most commonly dislocated joint in adults, following the shoulder and most common dislocation in children (1). Elbow dislocations can be broadly classified as simple or complex, where complex dislocations include a fracture of the radial head or neck, olecranon, coronoid or humeral condyles or epicondyles (6). This blog will focus on the early management and rehabilitation of simple elbow dislocations.
Elbow Anatomy
Stability of the elbow joint is provided by congruity of the bony structures, stabilising ligaments and the forces of the muscles that cross the joint. The bony articulation between the ulna and humerus and the medial and collateral ligaments are the primary stabilisers. The radial head, anterior capsule and muscles that cross the elbow joint are considered secondary stabilisers (4).
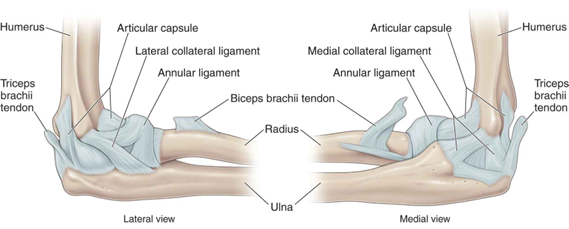
(5)
Mechanism of Injury
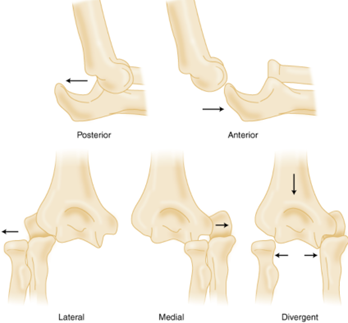
Dislocations are commonly the result of a large axial force or a fall onto an outstretched hand, with around 40% of dislocations being the result of a sporting injury (6). Elbow dislocations can be further classified, based on the direction of the dislocation, anterior or posterior, and then subdivided to include medial or lateral. The most common elbow dislocation is in the posterolateral direction.
Contrary to the name, simple elbow dislocations are a complex injury to the capsuloligamentous structures of the elbow (3). There are two models of injury described in the literature. The first is a valgus, compression, supination model, which would result in soft tissue disruption from lateral to medial, described as the ‘Horii’ circle as described by Horii and O’Driscoll et al. The alternative model of injury more recently described by Scheiber et al., postulates a valgus, hyperextension injury, in which the elbow widens on the medial side first, tearing first the medial ligament and then the lateral ligament. Various studies including MR, radiographic, cadaver and video analysis findings have reported on soft tissue findings. Common to all studies is the finding that elbow dislocations result in a varied spectrum of soft tissue disruption (2,8).
Early Management
Immediate management of elbow dislocation involves diagnosis via radiography, and orthopaedic reduction, typically performed in the emergency department. Following the reduction radiographs should be taken to verify adequate reduction and clinical tests undertaken to determine stability (7). The elbow should be stable through full range of motion to be classified as clinically stable and allow confident early mobilisation. If high grade instability is present post reduction, immediate orthopaedic follow up (within 3-5 days) is required and MR imaging is recommended to determine ligamentous integrity. If high grade instability remains and the ligaments are not intact surgical repair may be indicated in some cases. Due to the varied nature of soft tissue disruption following dislocation, it can be expected that the prognosis is quite heterogeneous.
Following an adequate and stable elbow reduction, conservative (non-surgical) management is widely accepted as best practice management of simple elbow dislocations. Historically, conservative management consisted of immobilisation in a Plaster of Paris cast for 3 weeks post dislocation. However, the most appropriate method of conservative management has been studied, and it has been shown that early mobilisation is best practice management (3). Early mobilisation consists of sling use (+/- bandaging) outside of Physiotherapy / exercise sessions (6).
A 2020 systematic review (6) analysed results of randomised control trials comparing outcomes of immobilisation versus early mobilisation. The results of these studies showed that the early mobilisation group achieved an earlier return of full flexion and extension active range of motion (ROM), and earlier return to work and sport. However, the early mobilisation group does demonstrate higher pain levels in the first 6 weeks compared to immobilisation. At 12 month follow up only one study showed superior results in the early mobilisation group, with the results of the other studies equalling out between the two groups by this time. Redislocation rates were similar, and low, in both groups at 12 month follow up, with a lower incidence of heterotopic ossification (abnormal bone growth within soft tissues following trauma) in the early mobilisation group.
Rehabilitation Protocols
Several of the studies within the 2020 systematic review detailed rehabilitation protocols to follow during the early mobilisation period, commencing 2 days following dislocation. Protocols should be followed under the supervision of your Orthopaedic specialist and Physiotherapist.
Below is the outline of the early mobilisation protocol:

(6)
Weeks 0-3: Early Protected ROM (in the supine position)
The exercises are performed in supine with the shoulder flexed to 90degrees, adducted and in a neutral to external rotation position as per the below image. This position minimises the effect of gravity and limits posteriorly directed force.
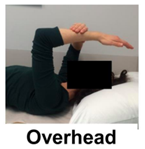
(9)
As per the below image the following exercises can be performed in the described position:
- A: Elbow flexion
- B: Elbow extension
- C: Supination (twisting palm to face upwards)
- D: Pronation (twisting palm to face downwards)
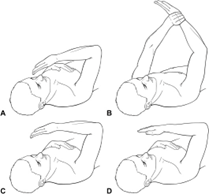
(4)
Each of these exercises can be performed without range of motion restrictions, as this is a protected position for the elbow. Range of motion limits should be dictated by the patient’s tolerance levels (4).
Weeks 3-6: Full Active ROM (in the dependant position)
At this stage joint stability should be achieved, which is assessed with a lateral extension elbow radiograph to ensure joint congruency. If the joint is stable the sling can be removed and full active ranging commenced in the dependent position. The degree of motion is based on the patients level of stability and comfort levels.

(9)
Week 6 Onwards: Full ROM and Strengthening
From the 6 week mark there are no restrictions on range of motion and strength and endurance exercises can commence. The goals of the progressive exercise therapy is to restore strength to the affected side, as well as regain proprioception and stability. It is at this point that patients can expect to return to normal activities such as driving and working, however higher demand activities such as sport may take longer to phase back into.
Physiotherapy Role
The treating Physiotherapist will be able to guide patients who have sustained an elbow dislocation through the above mentioned protocols. As with all injuries there is no one size fits all rehabilitation protocol, and Physiotherapists will continually monitor the patients progress throughout the entire rehabilitation process and may make adjustments as appropriate, based on healing, stability and pain levels.
As part of the rehabilitation process, from the 6 week mark, Physiotherapist’s will prescribe strengthening exercises. These exercises will primarily target muscles of the arm that cross the elbow joint, as well as the wider kinetic chain. As with all exercise prescription, programs should be designed in collaboration with the patient, taking into account current rehabilitation progress, exercise preferences and goals. Return to high demand workplace duties and sporting endeavours should be completed in a progressive manner, as guided by the treating Physiotherapist. Timeline on return to such activities is varied and depends on the patient’s rehabilitation progress relative to the demands of the desired activities.
Summary
Simple elbow dislocations are defined as those without a concomitant fracture, however despite the name they constitute a substantial capsuloligamentous injury, with varied levels of soft tissue disruption. Best practice management of simple elbow dislocation, once a stable reduction is achieved, involves early mobilisation. Early mobilisation involves 3 weeks of protected range of motion in the overhead position, 3 weeks of full active range of motion in the dependent position. After 6 weeks patients can return to normal activities, move through full range of motion without restrictions and commence progressive strength and endurance exercises. Full return to work and sport will be guided by the treating team taking into account progress, stability and workplace / sporting demands. All rehabilitation should be completed under the guidance of the treating Physiotherapist and Orthopaedic specialist.

Eliana Lonsdale (APAM)
POGO Physiotherapist
Book an appointment with Eliana today
Featured in the Top 50 Physical Therapy Blog
References
- Robinson, P. M., Griffiths, E., & Watts, A. C. (2017). Simple elbow dislocation. Shoulder & Elbow, 9(3), 195-204. doi:10.1177/1758573217694163
- Watts, A. C. (2022). 39 – Traumatic Elbow Ligamentous Injury. In G. E. Garrigues, M. J. Richard, & M. J. Gage (Eds.), Skeletal Trauma of the Upper Extremity (pp. 315-326). Philadelphia: Elsevier.
- Hackl, M., Beyer, F., Wegmann, K., Leschinger, T., Burkhart, K. J., & Müller, L. P. (2015). The treatment of simple elbow dislocation in adults. Deutsches Arzteblatt international, 112(18), 311-319. doi:10.3238/arztebl.2015.0311
- Schreiber, J. J., Paul, S., Hotchkiss, R. N., & Daluiski, A. (2015). Conservative Management of Elbow Dislocations With an Overhead Motion Protocol. The Journal of Hand Surgery, 40(3), 515-519.
- Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011
- Catapano, M., Pupic, N., Multani, I., Wasserstein, D., & Henry, P. (2020). Early functional mobilization for non-operative treatment of simple elbow dislocations: a systematic review. Shoulder & Elbow, 1758573220957631. doi:10.1177/1758573220957631
- van der Horst, A. S., Stephens, A. R., Wei, G., Presson, A. P., Tashjian, R. Z., & Kazmers, N. H. (2021). Prognostic Factors Affecting Long-Term Outcomes After Elbow Dislocation: A Longitudinal Cohort Study. Journal of Hand Surgery Global Online. doi:https://doi.org/10.1016/j.jhsg.2021.05.011
- Schnetzke, M., Ellwein, A., Maier, D., Wagner, F. C., Grützner, P.-A., & Guehring, T. (2021). Injury patterns following simple elbow dislocation: radiological analysis implies existence of a pure valgus dislocation mechanism. Archives of Orthopaedic and Trauma Surgery, 141(10), 1649-1657. doi:10.1007/s00402-020-03541-0
- Manocha, R. H. K., Kusins, J. R., Johnson, J. A., & King, G. J. W. (2017). Optimizing the rehabilitation of elbow lateral collateral ligament injuries: a biomechanical study. Journal of Shoulder and Elbow Surgery, 26(4), 596-603. doi:https://doi.org/10.1016/j.jse.2016.09.038




