


Running, Pelvic Floor Function and Incontinence

Running is a popular form of exercise with numerous health benefits. However, for some men and women it can lead to urinary incontinence, a condition characterised by the involuntary leakage of urine. This can create a barrier to exercise, with over 75% finding it bothersome and for some symptoms are moderate to severe (1, 5). In this blog we explore the relationship between urinary incontinence, running and pelvic floor strength and function.
Pelvic Floor Anatomy and Function
The pelvic floor is a complex structure consisting of muscles, ligaments, and connective tissues that support the organs within the pelvis. In females, the pelvic floor muscles include a deep layer called the levator ani (pubococcygeus, iliococcygeus, and puborectalis muscles) and a superficial layer (bulbospongiosus, external anal sphincter and external urethral sphincter). These muscles form a hammock-like structure that supports the bladder, uterus, and rectum. These muscles, alongside ligaments and connective tissue form the pelvic floor and play a crucial role in supporting the pelvic organs, maintaining continence and sexual function. Additionally, in males the levator ani muscles support the pelvic organs, while bulbospongiosus and ischiocavernosus muscles are involved in erectile function and ejaculation. Key nerves in this region include the pudendal nerve, inferior rectal nerves, perineal nerve, nerve to levator ani which branch from the sacral nerves (S2-S5). These nerves innervate the pelvic floor muscles to maintain pelvic floor muscle tone and function.
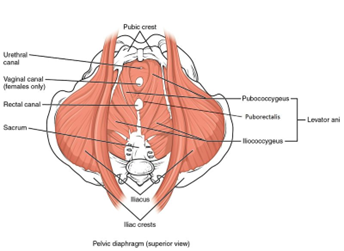
Source: physio-pedia
To summarise both males and females, the pelvic floor serves 3 crucial functions, including:
- Supporting the pelvic organs; including the bladder, uterus (in females), and rectum.
- Maintaining urinary and faecal continence
- Assisting in sexual function by controlling the muscles involved in erection (in males) and supporting vaginal tone (in females).
Prevalence and Risk Factors for Incontinence
Incontinence can be broadly separated into urinary incontinence or faecal incontinence, for the purposes of today’s article we will focus more on urinary incontinence. It can be categorised into different types, including stress urinary incontinence (SUI), urge urinary incontinence (UUI), and mixed urinary incontinence (MUI). SUI is often associated with physical activities that cause a large or sudden increase in intra-abdominal pressure; which can then lead to leakage. High-impact activity, such as running, is associated with a sudden rise in intra-abdominal pressure (1). This may also include during coughing, sneezing, strength training or other forms of impact exercise. Running can be considered high impact due to the ground reaction forces acting on the body (1.5-2.5 times body weight) with not all of these absorbed by the lower limb muscles (2).
There are various reports on the prevalence of SUI in runners. A review of female recreational runners from 2023 reported a prevalence of UI during running was 16% (3). Another study which also did not include pregnant women reported a prevalence of 13%. Additionally most runners reporting UI did not consult health care providers (70%) (3). A review of the prevalence of UI in female nulliparous (never given birth) athletes during exercise ranges from 5.7% to 80% (5). The prevalence rates differ according to the types of sports of which the highest prevalence of UI was observed in trampolinists. Of the studies that included runners, prevalence was reported as 35% (6), 11% in a second study (7) and 26% in a group of track athletes (8). In this review, 50%- 92% of athletes had never discussed the problem with anyone (5), highlighting the importance of education and discussion of various prevention and treatment strategies that may be available.
There is less data available for prevalence in male athletes. A 2021 study looking at the prevalence of UI among elite athletes found thirty-three percent of the athletes suffered UI (females 45.1%, males 14.7%)(17). In males increased training frequency and volume did not increase risk and within athletics higher prevalence was observed in the athletics disciplines of mountain running and sprints. Risk of urinary incontinence in men is increased following radical prostatectomy, along with increasing age and diabetes (29). Urinary incontinence is not unique to the adult population with prevalence also reported in adolescent female athletes of 14.4% (15-19 year olds) (18, 19).
The risk of urinary incontinence is increased during and after pregnancy (9). The prevalence of urinary incontinence during pregnancy was 3.3 times higher compared with a control group of nulliparous women (females who have never given birth) . After 1 year, the difference was reduced, but still 2.5 times higher in the group who had given birth (9). After having a baby, the pelvic floor is commonly weakened or injured (10), and as a result pelvic floor muscle training is recommended in this muscle population and there is a strong evidence background that is reducing and preventing incontinence (11). Additionally, guidelines for return to running after pregnancy have been developed to provide a guide on how to do so without injury, pain or incontinence (12).
Risk factors for UI included number of deliveries, number of vaginal deliveries, the 40- to 44-year-old age range, and the perimenopausal phase (3). Other factors that may be relevant to running populations include intensity of running, with a recent study finding ‘high effort’ runners present a higher incidence of pelvic floor dysfunction in comparison to ‘moderate effort’ runners (4). Other factors that have been correlated with an increased risk of UI include constipation, a family history of UI, and a history of urinary tract infection (UTI) in female athletes (20). Eating disorders in female athletes are a risk factor for UI with higher prevalence of SUI in athletes with eating disorders, compared to those without (21). UI is also more prevalent in adolescent female athletes with low energy availability in comparison to female athletes with adequate energy availability (18, 19). These terms and their importance are expanded upon below.
Of the reports of urinary incontinence across most studies athletes mentioned that they experience leakage only during their sport activities (5). Repeated intra-abdominal pressure during sport may fatigue the pelvic floor, and this may reduce the effectiveness of the continence mechanism (5). This theory is supported by a 2007 study, which observed fatigue of the pelvic floor muscles after strenuous exercise in nulliparous females with SUI (22).
Problems with continence can occur because of a defect in bladder storage (overactive bladder) and this may be neurogenic or nonneurogenic in origin (23). Alternatively there may be a defect in the urethral sphincter mechanism or the defect may lie in the supports of the urethra, in particular the pelvic floor (23). Together there are multiple risk factors and mechanisms that influence each individuals presentation.
RED-S
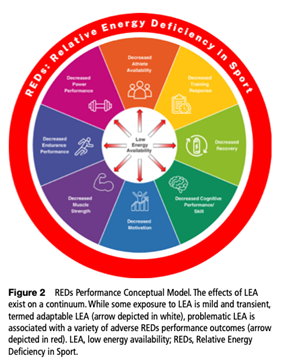
Consideration of the risk of Relative Energy Deficiency in Sport (RED-S), a more comprehensive term for what was previously referred to as the Female Athlete Triad Syndrome (24), is not to be overlooked for runners with urinary incontinence. Low energy availability (LEA) is any mismatch between dietary energy intake and energy expended in exercise, that leaves the body’s total energy needs unmet (24). That is, there is inadequate energy to support the functions required to maintain health and perform optimally. If this is severe or sustained over a longer term this can lead to a syndrome of impaired physiological and/or psychological functioning experienced by male or female athletes termed RED-s. The detrimental outcomes include but are not limited to decreases in; energy metabolism, reproductive function , musculoskeletal (bone) health, immunity, glycogen synthesis, cardiovascular and haematological health. This is best summarised in the infographics below.

It describes the impairment of bodily functions due to excess energy expenditure without adequate replacement as a result of excessive activity or other lifestyle factors. Postnatal women with RED-S are at increased risk of stress fractures (25), pelvic floor dysfunction and fertility issues (26) . Additionally as the tissues involved in the female continence mechanism are oestrogen sensitive, it is possible that oestrogen deficiency may be an aetiological factor in the development of urinary incontinence (27). Among adult and adolescent female athletes with eating disorders, where UI was more prevalent in those with LEA in comparison to controls with adequate EA. With twice the likelihood of UI even within the same sports category and menstrual function (21). These findings suggest a potential place for awareness of genitourinary disorders amongst the impaired physiologic functions associated with low EA in athletes/RED-S (21).
Incontinence Signs and Symptoms
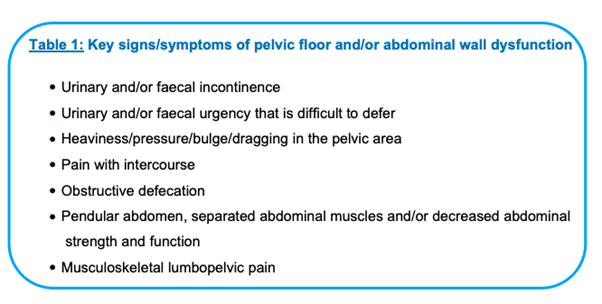
The following table is from the return to running guidelines postpartum (10) and highlights some of the potential signs and symptoms of pelvic muscle or abdominal wall dysfunction. In addition to this every postnatal mother, regardless of delivery mode, should be offered the opportunity to receive a pelvic health assessment (from 3 weeks postnatal) with a specialist physiotherapist to comprehensively assess the abdominal wall and pelvic floor including vaginal and or anorectal examination as indicated. Pelvic floor assessment is an important aspect of determining strength, endurance and coordination (10). As previously mentioned, the high level evidence supports pelvic floor rehabilitation for the management of all types of urinary incontinence (11, 13).
Pelvic Floor Muscle Training
The pelvic floor muscles play a crucial role in maintaining urinary continence by providing support to the bladder, urethra, and other pelvic organs as discussed above. There is evidence supporting individualised pelvic floor rehabilitation for the management of urinary incontinence (11,13), pelvic organ prolapse (14) the prevention of pelvic organ prolapse (15) and sexual dysfunction (16). Pelvic floor muscle training is recommended to be done with a pelvic health or women’s health physiotherapist where assessment of pelvic floor coordination, strength and endurance is performed. The consensus of this guide is that running is less advisable if there is lower than grade 3 Modified Oxford Manual Muscle Testing (MOMMT) score during digital vaginal or ano-rectal examination (12, 28). Testing is completed in both crook lying and functional positions such standing to get a true indication of pelvic floor function and pelvic organ support (12). In the postpartum population, the recommended baseline in standing is the ability to perform 10x fast reps, 8-12 reps of 6-8 second maximum voluntary contraction and a 60 seconds submaximal 30-50% contraction (12).
Women who present with less than grade 3 MOMMT score without identifiable compromise in their fascial support may be considered appropriate for graded return to running if no other signs or symptoms are present during load impact testing. In some women however pelvic floor muscle strength may be high, yet injury or deficits to fascia/ligamentous supports may still lead to incontinence. Some women in consultation with their health care professional may have fascial support deficits addressed via a pessary or other support devices prior to return to running (16).
Men’s health physiotherapists can also assess the ability for men to perform pelvic floor exercises. In the clinic, often an ultrasound of your pelvic floor muscles is performed to assess their function and strength. Commonly used cues include ‘squeeze your anus,’ ‘shorten the penis,’ ‘elevate the scrotum’ and ‘stop the flow of urine (31). Combining the right cues and feedback males too can train the strength and endurance of their pelvic floor. For those unsure men’s health physiotherapists are a good contact source (https://www.menshealth.physio/).
Load Tests for Return to Running
In those who are not already running there are guides available for load and impact assessment. In a version adapted for return to running post pregnancy the assessment in successfully completed if the following can be done without pain, heaviness, dragging or incontinence (12):
- Walking 30 minutes
- Single leg squat 10 repetitions each side
- Jog on the spot 1 minute
- Forward bounds 10 repetitions
- Hop in place 10 repetitions each leg
Pelvic floor muscle training can be utilised whilst performing other exercises to determine levels of stress the pelvic floor can manage without incontinence.
Other Management Strategies for Runners
- Incontinence Aids (eg pessary)
- Running Technique: Maintaining good running may help minimise the impact on the pelvic floor muscles. Whilst there is numerous variation on what good running form looks like, one variable often associated with injury risk is overstriding (31). Numerous lower limb injuries may benefit from small increases in cadence (number of steps per minute) 5-7.5% or running ‘softer’ (31). A case study from 2023 provides an example of a running with SUI having a meaningful improvement in symptoms with gait retraining with a focus on running softer (32).
- Progressive overload and Cross training: Gradually increasing running intensity and volume may allow the pelvic floor muscles to adapt and strengthen over time. Sudden spikes in activity levels, such as rapidly increasing running distance or intensity, may overload the pelvic floor and increase the risk of urinary incontinence episodes. Run – walk breaks may also be a method of reducing overall stress whilst running.
Summary
Urinary incontinence is a common concern among runners. By understanding the relationship between urinary incontinence, pelvic floor strength, and running, individuals can take proactive measures to mitigate symptoms and enjoy the benefits of running without incontinence. Incorporating pelvic floor exercises, potentially modifying running technique, and gradually progressing training intensity are key strategies for promoting pelvic floor health in runners. Consultation with your men’s or women’s health physiotherapist or specialist is a key step for any assessment and individualised management plan as we only bridge the surface on a detailed and complex topic.

Lewis Craig (APAM) – With oversights from my Wife and Women’s Health Physiotherapist, Emily
POGO Physiotherapist
Masters of Physiotherapy
Featured in the Top 50 Physical Therapy Blog
References
- Leitner, M., Moser, H., Eichelberger, P., Kuhn, A. and Radlinger, L. (2016) Evaluation of pelvic floor muscle activity during running in continence and incontinence women: An exploratory study. Neurourol Urodynam 9999, 1–7
- Gottschall, J.S. and Kram, R. (2005) Ground reaction forces during downhill and uphill running. Journal of Biomechanics 38, 445-452.
- Hamilton, H. M., Mariano, M., & Kakar, R. S. (2023). Prevalence and Associated Factors of Urinary Incontinence in Female Recreational Runners. Journal of Women’s Health Physical Therapy, 47(2), 75-89.
- Sade, S., Naor, I., Rotem, R. et al. Pelvic floor disorders among amateur runners. Arch Gynecol Obstet (2024). https://doi.org/10.1007/s00404-023-07351-8
- Almousa, S., & Bandin Van Loon, A. (2019). The prevalence of urinary incontinence in nulliparous female sportswomen: A systematic review. Journal of sports sciences, 37(14), 1663-1672.
- Poświata, A., Socha, T., & Opara, J. (2014). Prevalence of stress urinary incontinence in elite female endurance athletes. Journal of Human Kinetics, 44(1), 91–96.
- Santos, E. S. D., Caetano, A. S., Tavares, M. D. C. G. C., & Lopes, M. H. B. D. M. (2009). Urinary incontinence among physical education students. Revista Da Escola De Enfermagem Da USP, 43(2), 307–312.
- Nygaard, I. E., Thompson, F. L., Svengalis, S. L., & Albright, J. P. (1994). Urinary incontinence in elite nulliparous. Obstetrics & Gynecology, 2, 183–187.
- Hansen, B. B., Svare, J., Viktrup, L., Jørgensen, T., & Lose, G. (2012). Urinary incontinence during pregnancy and 1 year after delivery in primiparous women compared with a control group of nulliparous women. Neurourology and urodynamics, 31(4), 475-480.
- Bø, K. Artal, R., Barakat, R., Brown, W. J., Davies, G. A. L., Dooley, M., Evenson, K. R., Haakstad, L. A. H., Kayser, B., Kinnunen, T. I., Larsénm K., Mottola, M. F., Nygaard, I., van Poppel, M., Stuge, B., Khan, K. M. (2017) Exercise and pregnancy in recreational and elite athletes: 2016/17 evidence summary from the IOC Expert Group Meeting, Lausanne. Part 3-exercise in the postpartum period. Br J Sports Med 51(21), 1516-1525
- Dumoulin, C., Cacciari, L. and Hay-Smith, E.C. (2018) Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews Issue 10 [Accessed online 24/02/19] doi: 10.1002/14651858.CD005654.pub4.
- Goom, T., Donnelly, G., & Brockwell, E. (2019). Returning to running postnatal–guidelines for medical, health and fitness professionals managing this population. Sports Medicine.
- Price, N., Dawood, R. and Jackson, S.R. (2010) Pelvic floor exercise for urinary incontinence: A systematic literature review. Maturitas 67(4), 309-315.
- Hagen, S., Stark, D., Glazener, C., Dickson, S., Barry, S., Elders, A., Frawley, H., Galea, M.P., Logan, J., McDonald, A., McPherson, G., Moore, K.H., Norrie, J., Walker, A. and 33 Wilson, D. (2014) Individualised pelvic floor muscle training in women with pelvic organ prolapse: a multicenter randomised controlled trial. The Lancet 282(9919), 796-806.
- Hagen, S., Glazener, C., McClurg, D., Macarthur, C., Elders, A., Herbison, P., Wilson, D., Toozs-Hobson, P., Hemming, C., Hay-Smith, J., Collins, M., Dickson, S. and Logan J. (2017) Pelvic floor muscle training for secondary prevention of pelvic organ prolapse (PREVPROL): a multicenter randomized controlled trial. The Lancet 389(10 067), 393-402.
- Brækken, I. H., Majida, M., Ellström Engh, M. and Bø, K. (2015). Can Pelvic Floor Muscle Training Improve Sexual Function in Women with Pelvic Organ Prolapse? A Randomized Controlled Trial. The Journal of Sexual Medicine, 12(2), 470–480.
- Rodríguez-López, E. S., Calvo-Moreno, S. O., Basas-García, Á., Gutierrez-Ortega, F., Guodemar-Pérez, J., & Acevedo-Gómez, M. B. (2021). Prevalence of urinary incontinence among elite athletes of both sexes. Journal of science and medicine in sport, 24(4), 338-344.
- Whitney, K. E., Holtzman, B., Parziale, A., & Ackerman, K. E. (2019). URINARY INCONTINENCE IS MORE COMMON IN ADOLESCENT FEMALE ATHLETES WITH LOW ENERGY AVAILABILITY. Orthopaedic Journal of Sports Medicine, 7(3_suppl), 2325967119S0011. doi:10.1177/2325967119s00115
- Whitney KE, Holtzman B, Cook D, et al. Low energy availability and impact sport participation as risk factors for urinary Incontinence in female athletes. J Pediatr Urol 2021;17:290.
- Almeida, M.B.A.; Barra, A.A.; Saltiel, F.; Silva-Filho, A.L.; Fonseca, A.M.R.M.; Figueiredo, E.M. Urinary incontinence and other pelvic floor dysfunctions in female athletes in Brazil: A cross-sectional study. Scand. J. Med. Sci. Sports 2016, 26, 1109–1116.
- Kruger, J.A.; Dietz, H.P.; Murphy, B.A. Pelvic floor function in elite nulliparous athletes. Ultrasound Obstet. Gynecol. 2007, 30, 81–85.
- Ree ML, Nygaard I, Bø K. Muscular fatigue in the pelvic floor muscles after strenuous physical activity. Acta Obstet Gynecol Scand. 2007;86(7):870-6. doi: 10.1080/00016340701417281. PMID: 17611834.
- Keane, D. P., & O’Sullivan, S. (2000). Urinary incontinence: anatomy, physiology and pathophysiology. Best Practice & Research Clinical Obstetrics & Gynaecology, 14(2), 207-226.
- Mountjoy, M., Ackerman, K. E., Bailey, D. M., Burke, L. M., Constantini, N., Hackney, A. C., … & Erdener, U. (2023). 2023 International Olympic Committee’s (IOC) consensus statement on relative energy deficiency in sport (REDs). British journal of sports medicine, 57(17), 1073-1097.
- Mountjoy, M., Sundgot-Borgen, J., Burke, L., Carter, S., Constantini, N., Lebrun, C., … & Ljungqvist, A. (2014). The IOC consensus statement: beyond the female athlete triad—relative energy deficiency in sport (RED-S). British journal of sports medicine, 48(7), 491-497.
- Carvalhais, A., Da Roza, T., Vilela, S., Jorge, R. N., & Bø, K. (2018). Association between physical activity level and pelvic floor muscle variables in women. International journal of sports medicine, 39(13), 995-1000.
- Cody JD, Jacobs ML, Richardson K, Moehrer B, Hextall A. Oestrogen therapy for urinary incontinence in post-menopausal women. Cochrane Database Syst Rev. 2012 Oct 17;10(10):CD001405. doi: 10.1002/14651858.CD001405.pub3. PMID: 23076892; PMCID: PMC7086391.
- Laycock, J. O., & Jerwood, D. (2001). Pelvic floor muscle assessment: the PERFECT scheme. Physiotherapy, 87(12), 631-642.
- Shamliyan TA, Wyman JF, Ping R, Wilt TJ, Kane RL. Male urinary incontinence: prevalence, risk factors, and preventive interventions. Rev Urol. 2009 Summer;11(3):145-65. PMID: 19918340; PMCID: PMC2777062.
- Ben Ami N, Feldman R, Dar G. Verbal Instruction for Pelvic Floor Muscle Contraction among Healthy Young Males. Int J Environ Res Public Health. 2022 Sep 23;19(19):12031. doi: 10.3390/ijerph191912031. PMID: 36231333; PMCID: PMC9566287.
- Barton, C. J., Bonanno, D. R., Carr, J., Neal, B. S., Malliaras, P., Franklyn-Miller, A., & Menz, H. B. (2016). Running retraining to treat lower limb injuries: a mixed-methods study of current evidence synthesised with expert opinion. British journal of sports medicine, 50(9), 513-526.
- Steimling, M., Roberto, M., & Steimling, M. (2023). Running Gait Retraining in the Management of a Multiparous Runner With Chronic Stress Urinary Incontinence: A Case Study. The Journal of Women’s & Pelvic Health Physical Therapy, 47(2), 114-121.






