


Polymyalgia Rheumatica – Diagnosis & Management

Definition
Polymyalgia Rheumatica (PMR) is the most common inflammatory disease in the elderly population. PMR is characterised by pain and stiffness most commonly affecting the shoulder joints and upper arms, and less frequently in the neck, pelvis and upper thighs. PMR patients typically experience morning stiffness that lasts for greater than 45 minutes and also suffer from symptoms such as general fatigue and malaise, low mood and loss of appetite. Onset of symptoms can be as rapid as overnight, with progressive aggravation over the following days-weeks. Symptoms are often aggravated by high joint loading activities, with stiffness returning throughout the day after prolonged periods of inactivity. PMR rarely occurs in patients under 50 years old, with the highest onset in those over 65 years of age (1). PMR is more common in females than males and particularly those of Northern European ancestry (2).
Diagnosis
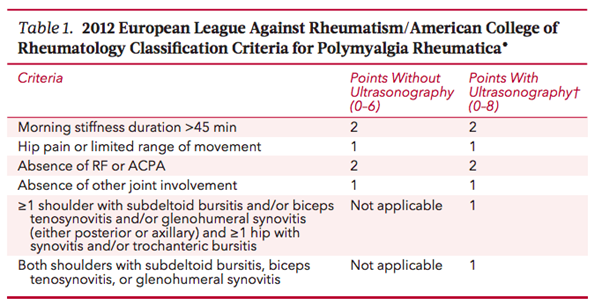
There are no universal diagnostic criteria for PMR, and patients often have symptoms for 2-3 months before a diagnosis is made (2). In 2012 the European League Against Rheumatism (EULAR) developed provisional classification criteria, which can be found in the table below. It is important to note that these criteria do not constitute a definitive diagnosis of PMR, but are intended for classification purposes in clinical studies. Given the non-specific nature of the clinical symptoms and the current lack of understanding of the pathophysiology PMR is essentially considered a diagnosis of exclusion and can only be made in the absence of another diagnosis (e.g. a chronic infection or rheumatic disease such as Rheumatoid Arthritis).
Clinical Presentation:
- Rapid onset of pain & stiffness in neck, shoulders, hips
- Morning stiffness >45mins
- Stiffness worse after periods of rest
- Radiation pattern of shoulder pain to elbows and hip pain to knees
- 40-50% of patients may also experience systemic symptoms such as fatigue, depression, anorexia, weight loss and low grade fever
Physical Examination:
- Wide spread shoulder pain
- Restricted and painful active range of motion of the shoulders, neck and hips (particularly shoulder flexion and hip flexion)
- Passive range of motion is often reduced
- Tenderness to palpation, around the neck, shoulders and greater trochanter
- Muscle weakness is not common, although may be present secondary to pain
- Normal neurological examination
Management
PMR patients are generally diagnosed and treated within the primary care system, however should be considered for specialist referral if the patient presents with atypical features.
Atypical presentations would include;
- Peripheral arthritis
- Gradual onset >2 months before full features evolve
- Lack of shoulder involvement
- Lack of inflammatory stiffness
- Neurological signs
- Age <60 years
- Normal or extremely high ESR or CRP levels
- Signs and symptoms of giant cell arteritis such as jaw pain and claudication, fevers, vision disturbances, severe head pain (typically in the temple region)
- Consistent flare ups would also be grounds for specialist referral
Pharmacological
Oral glucocorticoids (e.g. prednisolone) is the mainstay of PMR pharmacological treatment. Whilst effective, long term glucocorticoid use is associated with significant adverse effects, therefore most treatment involves an initial dosage to induce remission followed by a tapering period to avoid long term glucocorticoid exposure (4). Unfortunately during the attempted tapering period relapses are common, which may lead to longer term glucocorticosteroid use (4). Well known adverse effects of long term glucocorticosteroid include a decrease in bone formation which can lead to osteoporosis, and muscle myopathy leading to muscle weakness. PMR patients should be assessed for osteoporosis and fracture risk and if necessary bone sparing medications such as bisphosphonates may also be prescribed for those at higher risk (5).
Physiotherapy
The EULAR guidelines recommends “prescription of an individualised exercise program with the goals being maintenance of muscle strength, function and falls prevention, particularly in eldery sufferers”.
Resistance exercise has been proven to improve bone mineral density and reduce the risk of fractures in individuals with osteoporosis. In addition to this, studies show that resistance exercise also results in improved physical function, quality of life and ease of activities of daily living in those with osteoporosis (6). Given the higher risk of osteoporosis in PMR patients, due to long term glucocorticoid use, resistance exercise should be considered to attempt to attenuate bone and muscle loss. A history or high risk of falls is another risk factor of osteoporotic fracture and clinical attention should be paid to assessing and managing falls risk, which can be undertaken by a Physiotherapist (5).
There is currently a gap in evidence regarding the efficacy of non-pharmacological interventions for PMR, however a recent cohort study reported on patient perceptions of non-pharmacological interventions. It was reported that most participants reported change in exercise (85%), massage (86%) and hydrotherapy (81%) as being helpful interventions. It was also reported that the uptake of non-pharmacological interventions is lower in the PMR group compared to studies of Rheumatoid Arthritis and Osteoarthritis, which was speculated to be due to a better developed evidence base in those populations compared with PMR (4). Multiple studies show that compliance to exercise therapy is low in those with PMR due to uncertainty regarding which exercises are beneficial and fear of a flare up in symptoms (4). Therefore, as with all prescriptive exercise programs, an individualised and collaborative approach should be used, with programs based on patient preferences and individual response to therapies. Additionally, a strong educational base is required, with clear explanations of the benefits of the prescribed exercise program, and reassurance that exercise therapy is safe for PMR populations.
Summary
Polymyalgia Rheumatica is an inflammatory disease which results in pain and stiffness in the shoulders, neck and hips and morning stiffness lasting longer than 45 minutes. PMR is primarily managed pharmacologically with glucocorticoids. Physiotherapy interventions can assist in maintaining strength, range of motion and improving function, as well as reducing side effects associated with long term glucocorticoid use.

Eliana Lonsdale (APAM)
POGO Physiotherapist
Book an appointment with Eliana today
Featured in the Top 50 Physical Therapy Blog
References
- González-Gay, M. A., Matteson, E. L., & Castañeda, S. (2017). Polymyalgia rheumatica. The Lancet, 390(10103), 1700-1712.
- Matteson, E. L., & Dejaco, C. (2017). Polymyalgia rheumatica. Annals of internal medicine, 166(9), ITC65-ITC80.
- Pipitone, N., & Salvarani, C. (2013). Update on polymyalgia rheumatica. European journal of internal medicine, 24(7), 583-589.
- Weddell, J., Hider, S. L., Mallen, C. D., & Muller, S. (2022). What non-pharmacological treatments do people with polymyalgia rheumatica try: results from the PMR Cohort Study. Rheumatology International, 42(2), 285-290. doi:10.1007/s00296-021-05036-6
- Sokhal, B. S., Hider, S. L., Paskins, Z., Mallen, C. D., & Muller, S. (2021). Fragility fractures and prescriptions of medications for osteoporosis in patients with polymyalgia rheumatica: results from the PMR Cohort Study. Rheumatology Advances in Practice, 5(3), rkab094. doi:10.1093/rap/rkab094
- Wilhelm, M., Roskovensky, G., Emery, K., Manno, C., Valek, K., & Cook, C. (2012). Effect of resistance exercises on function in older adults with osteoporosis or osteopenia: a systematic review. Physiotherapy Canada. Physiotherapie Canada, 64(4), 386–394. https://doi.org/10.3138/ptc.2011-31BH





