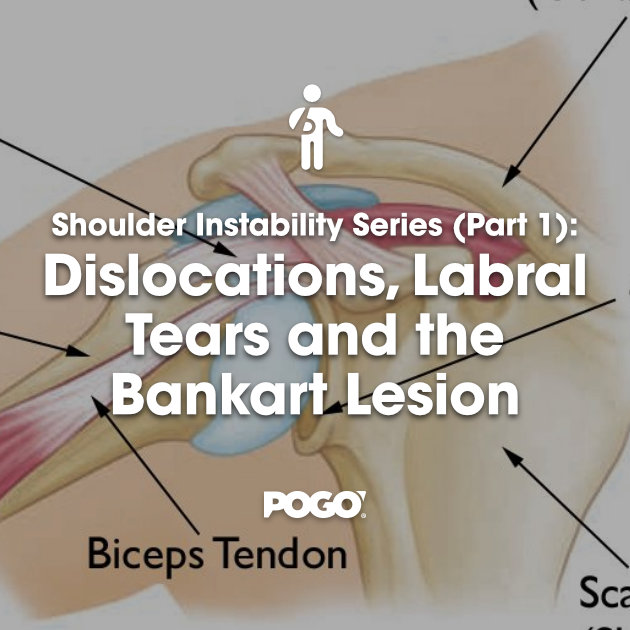
Shoulder Instability Series (Part 2): Rehabilitation and Return to Sport
Risks of returning to sport and importance of rehabilitation
For those under the age of 20, the risk of recurrence following an initial anterior shoulder dislocation is very high. It is for this reason; caution must be taken when a young athlete of any level sustains a shoulder instability episode.
An athletic study in 2014 showed that when a shoulder dislocation or subluxation occurred, 73% of the injured athletes returned to their sport that season – with an average injury time of 10 days. However, of those that returned – just 27% successfully completed the season without subsequent instability (1). Interestingly, the study found that regardless of whether the initial injury was a subluxation or dislocation – the recurrence of shoulder instability was common (1).
Rehabilitating the unstable shoulder
A systematic review of the literature concluded that when the conservative approach is undertaken, rather than surgical, rehabilitation should be consistent with the following:
- Immobilisation for three to four weeks
- A structured 12-week rehabilitation program consisting of
- Shoulder range of motion
- Glenohumeral (shoulder) and scapular (shoulder blade) stability exercises
These recommendations are most appropriate for clients with primary dislocations that are not undergoing surgery and wish to return to premorbid activity levels (4).
Phase 1: Initial
A large focus is placed on the dynamic stability of the shoulder when rehabilitating the joint following a dislocation or any kind. The rotator cuff play a large role in stabilising the shoulder in a dynamic manner and is therefore at the forefront of its rehabilitation.
Closed chain exercises involving the rotator cuff enhance joint stability, stimulate muscular contraction and increase proprioception (3). Exercises that involve weight-bearing or a fixed base of support are the focal point of this phase as they encourage muscle coactivation and scapula stability without applying a shear force to the shoulder (3).
Early submaximal isometric exercises for the rotator cuff that are within pain free limits are encouraged also, to improve the stability of the shoulder joint in the early stages of rehabilitation (3). Some examples of these exercises are called isometric holds, and are shown in the below images.
Isometric holds internal and external rotation


It is important to note that early feedback of posture and shoulder positions during exercises is crucial in avoiding the development of incorrect motor patterning and strengthening (3). Postural tape and sensory feedback techniques (e.g mirror) that facilitate correct muscle activation should be used in this initial phase – if it is found to be an issue (3).
Shoulder postural taping technique



Phase 2: Intermediate
After early rotator cuff activation and good postural alignment is achieved then the first phase is completed. Following this, the focus then shifts to performing these tasks through the full range of movement (3). Achieving full passive range of the shoulder is important before movements are performed with any resistance (including gravity). This can be done either by a trained medical professional, or at home by using the unaffected arm and a stick.
Keep in mind, when performing them at home – do not push the shoulder any further if instability and/or pain is felt.
Active assisted shoulder range of movement

Once full passive range is gained, it is time for the rotator cuff to be activated through range and against gravity. Exercises proven to be effective at achieving this are demonstrated in the photos below. Note that the position is on your side, this is due to the other muscles having less input in this position as well as on your stomach when you externally and internally rotating your shoulder. This allows greater concentration and activation of the rotator cuff muscles.
Side-lying internal and external rotation with weight




When progressing from these exercises greater resistance is needed to further strengthen the shoulder. Research shows rotator cuff exercises with a small amount of resistance (10-40% of maximal contraction) are more effective at optimising muscles such as the infraspinatus (3).
Resisted shoulder internal and external rotation






Resisted shoulder external and internal rotation in 90 degrees abduction
After gaining strength of the rotator cuff against resistance, the client is then ready to progress to strengthening exercises that are more functional or involve other parts of the body. Some examples of these are the lateral band walks as well as side and front planks. These include scapula (shoulder blade) stability as well as the involvement of core.
Shoulder lateral band walks


Front and side planks


I have already touched on the importance of the rotator cuff muscles in shoulder instability rehab – as they are the dynamic stabilisers of the shoulder. However, the muscles that stabilise your shoulder blade (scapula) are another vital group of muscles that are required to be strong in order to have a stable shoulder joint.
Scapula strengthening exercises
- Upper trap shrug




- Seated low row


- Serratus punches


Supine scapular retractions with weighted internal/external rotation
Phase 3: Functional/Return to Sport
The third, and final, stage of shoulder stability rehabilitation is the functional/return to sport phase. Exercises are now performed at speed and with high repetitions to prepare the shoulders for the sport they are returning to. These exercises not only help with motor retraining but also regains confidence in the affected limb (3).
I’ve included a short clip showing four return to sport exercises – chest passes/catches, overhead throw-ins, basketball dribbling and sideways passing. Exercise selection should be based on the sport type and level and be completed with the same or similar equipment that will be used in training/game scenarios. For example, cricketers must practice single arm throwing and catching with a cricket ball and goalkeepers in football/soccer must practice safe landing and getting up with their rehabilitated shoulder.
VIDEO – Shoulder instability: return to sport exercise ideas
This concludes the Shoulder Instability Series. I hope that further understanding surrounding shoulder dislocation, labral tears, Bankart lesions and rehabilitation from all of these injuries was achieved. If you haven’t read part 1 of the series, click HERE

Alec Lablache
POGO Physiotherapist
Featured in the Top 50 Physical Therapy Blog
References
- Dickens, J. F., Owens, B. D., Cameron, K. L., Kilcoyne, K., Allred, C. D., Svoboda, S. J., . . . Rue, J. (2014). Return to play and recurrent instability after in-season anterior shoulder instability: A prospective multicenter study. The American Journal of Sports Medicine, 42(12), 2842-2850. doi:10.1177/0363546514553181
- Gibson, K., Growse, A., Korda, L., Wray, E., & MacDermid, J. C. (2004). The effectiveness of rehabilitation for nonoperative management of shoulder instability: A systematic review.Journal of Hand Therapy, 17(2), 229-242. doi:10.1197/j.jht.2004.02.010
- Jaggi, A., & Lambert, S. (2010). Rehabilitation for shoulder instability. British Journal of Sports Medicine, 44(5), 333-340. doi:10.1136/bjsm.2009.059311
- Pogson, C. (2013). Shoulder rehab for professional athletic performance: Case study in restoring shoulder function at an elite level after dislocation. Rehab Management, 26(9), 40.
- Soliaman, R. R., da Cunha, R. A., Pochini, A. d. C., Andreoli, C. V., Cohen, M., & Ejnisman, B. (2016). Less than 60% return to preinjury sports activities after primary anterior shoulder dislocation treated with immobilisation only. Journal of ISAKOS: Joint Disorders & Orthopaedic Sports Medicine, 1(4), 198-201. doi:10.1136/jisakos-2015-000034
- Trackactive.co. (2017). Exercises. Retrieved from https://app.trackactive.co/practices/1011/exercises