


Rheumatoid Arthritis – Diagnosis & Management

Definition
Rheumatoid arthritis (RA) is a chronic systemic auto-immune inflammatory disease, which has a lifetime prevalence of up to 1% worldwide (1). Inflammation in RA primarily affects the smaller joints e.g. the fingers, and is characterized by pain & swelling. As a result of the systemic nature of RA, the wide-spread inflammation not only affects the joints, but also results in fatigue, depression and an increased risk of cardiovascular disease (3). Multiple genetic and environmental factors have been associated with an increased risk of developing RA. The factors with the strongest associations are the female sex, family history of RA, exposure to tobacco smoke and the genome the ‘shared epitope’ (5).
Diagnosis
Unmanaged RA can lead to irreversible joint damage and significant disability, therefore early diagnosis is key. Early treatment of RA has been shown to substantially slow the progression of joint damage in up to 90% of patients, thereby preventing irreversible disability (2). Studies have shown that commencing treatment for RA within the first 3 months of onset plays a major role in achieving disease remission. Patients suspected of suffering from RA should be referred immediately to a rheumatologist for early diagnosis and treatment (3).
In 2010 the American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR) revised their diagnostic criteria, which has been proven to aid in earlier diagnosis of RA in recent years. The below table is applied to patients who present with swelling of at least one joint on physical examination, where another inflammatory disorder does not account for said swelling (4).
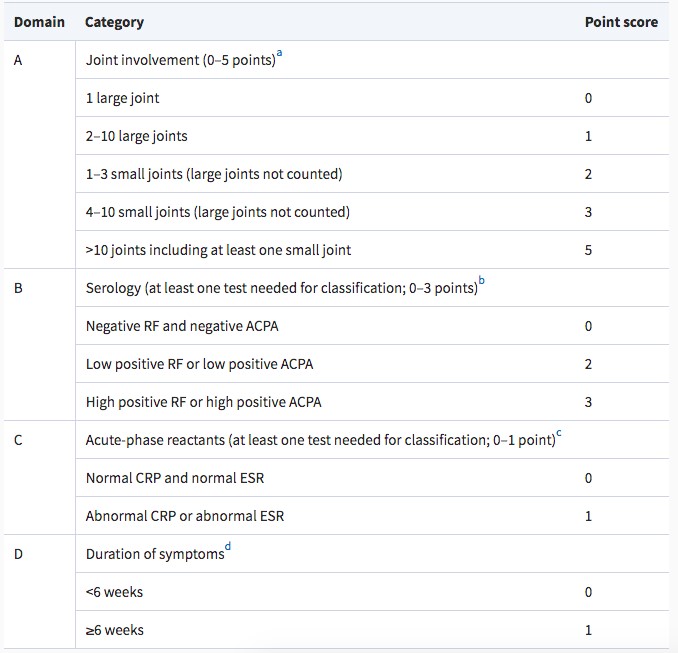
A score of >6 points is required to classify a patient as having RA.
Management
Optimal management of RA requires a multi-disciplinary approach under the overarching care of a rheumatologist. Both pharmacological and non-pharmacological treatment modailites should be employed in the treatment of RA.
Pharmacological
Disease-modifying antirheumatic drugs (DMARDs) are the first-line of treatment for RA. The goal of DMARD therapy is attaining a state of remission or at least a state of low disease activity for a greater than 6 month period. The first treatment sequence is Methotrexate in combination with glucocorticoids, optimal dosage in 25mg of methotrexate weekly; 40-50% of patients reach remission or low disease activity with this regimen. If this treatment fails, the next line of treatment is the application of biologic agents (tumour necrosis factor inhibitors) or Janus kinase inhibitors in combination with methotrexate. This treatment sequence allows 75% of patients to reach the treatment target over time (2). All pharmacologial treatment is prescribed under the care of a rheumatologist.
Physiotherapy
In addition to the well known benefits of exercise, namely improvements in cardiovascular health and reductions in metabolic syndromes and obesity, exercise has also been proven to have RA specific benefits. Targeted exercise programs have been proven to reduce pain and fatigue and improve cardiovascular and mental health in patients with RA (6).
Cardiovascular disease is highly prevalent in patients with RA, with an approximate incidence of 48% (68% incidence of myocardial infarction i.e. heart attack, 41% cerebrovascular accident i.e. stroke). The effects of both aerobic and resistance exercise on improving cardiovascular disease outcomes are well documented in the literature among all populations, and has also been proven to be both safe and effective in the RA population. A 2020 study allocated RA participants into 2 groups; a control group and exercise group. The control group was instructed to continue with their regular routine and not commence any new exercise over the 12 week period of the study. The exercise group performed weekly strength training for a 12 week period and were provided with handouts of the exercises and encouraged to continue with them independently at home. The exercise session included a 15min stretching routine and 45min of strength exercises with a resistance band. The exercise group demonstrated significant improvements in physical function, lower limb strength and mental health. These positive results were achieved with no adverse events or flare of symptoms over the 12 week period (7).
As RA affects smaller joints, it commonly leads to pain, stiffness and weakness of the hand, which can result in difficulty performing everyday activities and lowered quality of life (8). Joint protection therapy has previously been advocated as a treatment option for patients with RA or OA of the hand. A joint protection programme essentially involves reducing the amount of load placed on the joints in the hands, by minimising activities such as tight grasping, weight bearing and repetitive activities. A recent systematic review appraised the current literature with the aim of determining the efficacy of joint protection programmes for patients with RA. The conclusion was that joint protection programmes lack clinically important benefits in the domains of pain, hand function and grip strength. The National Institute of Clinical Excellence (NICE) guidelines recommend practitioners to prescribe a tailored stretching and strengthening program for pain and dysfunction of the hands in conjunction with appropriate drug therapies (9). Recent trials of a hand therapy program “Stretching and Strengthening for Rheumatoid Arthritis of the Hand” (SARAH) found exercise therapy of the hand a safe and effective adjunct treatment to drug therapy. SARAH is a 12 week tailored exercise program involving seven mobility exercises and four resistance exercises of the hand and arm. In comparison with usual care controls, the SARAH exercise program doubled the treatment effect in patient rated domains of overall hand function, activities of daily living, satisfaction and confidence to self-manage symptoms (10).
Practically speaking, we know that patients with RA will present at different times in the disease cycle, with varying symptoms and goals. Compliance to exercise therapy remains an ongoing barrier in the treatment of RA, therefore exercise programs should be designed in collaboration with the patients, taking into account personal exercise preferences and goals to maximise adherence to the program. As with all disease populations a strong educational base is required, with clear explanations of the benefits of the prescribed exercise program, with reassurance that exercise therapy is safe and effective for RA populations.
Summary
Rheumatoid arthritis is a chronic inflammatory disease that primarily affects the smaller joints such as fingers and hands and can also result in fatigue, depression and an increased risk of cardiovascular disease. Optimal management of RA requires a multi-disciplinary approach under the overarching care of a rheumatologist. A combination of pharmacological and non-pharmacological therapies is essential for best practice management of RA disease and symptoms. Various modes of exercise including aerobic, resistance and mobility exercise programs have been proven to improve quality of life outcomes in patients with RA.

Eliana Lonsdale (APAM)
POGO Physiotherapist
Book an appointment with Eliana today
Featured in the Top 50 Physical Therapy Blog
References
- Wasserman, A. (2011). Diagnosis and Management of Rheumatoid Arthritis. Am Fam Physician. 1;84(11):1245-1252.
- Aletaha, D., & Smolen, J. S. (2018). Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA, 320(13), 1360-1372. doi:10.1001/jama.2018.13103
- Rein, P., & Mueller, R. B. (2017). Treatment with Biologicals in Rheumatoid Arthritis: An Overview. Rheumatology and Therapy, 4(2), 247-261. doi:10.1007/s40744-017-0073-3
- Kay, J., & Upchurch, K. S. (2012). ACR/EULAR 2010 rheumatoid arthritis classification criteria. Rheumatology, 51(suppl_6), vi5-vi9. doi:10.1093/rheumatology/kes279
- Deane, K. D., Demoruelle, M. K., Kelmenson, L. B., Kuhn, K. A., Norris, J. M., & Holers, V. M. (2017). Genetic and environmental risk factors for rheumatoid arthritis. Best Practice & Research Clinical Rheumatology, 31(1), 3-18. doi:https://doi.org/10.1016/j.berh.2017.08.003
- Katz, P., Andonian, B. J., & Huffman, K. M. (2020). Benefits and promotion of physical activity in rheumatoid arthritis. Current Opinion in Rheumatology, 32(3). Retrieved from https://journals.lww.com/co-rheumatology/Fulltext/2020/05000/Benefits_and_promotion_of_physical_activity_in.14.aspx
- Sul, B., Lee, K. B., Joo, Y. B., Hong, B. Y., Kim, J.-S., Kim, K.-J., . . . Lim, S. H. (2020). Twelve Weeks of Strengthening Exercise for Patients with Rheumatoid Arthritis: A Prospective Intervention Study. Journal of Clinical Medicine, 9(9). doi:10.3390/jcm9092792
- Williamson, E., Srikesavan, C., Thompson, J., Tonga, E., Eldridge, L., Adams, J., & Lamb, S. E. (2020). Translating the Strengthening and Stretching for Rheumatoid Arthritis of the Hand Programme from clinical trial to clinical practice: An effectiveness–implementation study. Hand Therapy, 25(3), 87-97. doi:10.1177/1758998320948538
- National Institute for Health and Care Excellence, (2015). Addendum to Clinical Guidelines 79, Rheumatoid arthritis: the management of rheumatoid arthritis in adults. Retrieved from https://www.nice.org.uk/guidance/ng100/evidence/addendum-pdf-4902997358
- Lamb, S. E., Williamson, E. M., Heine, P. J., Adams, J., Dosanjh, S., Dritsaki, M., . . . Williams, M. A. (2015). Exercises to improve function of the rheumatoid hand (SARAH): a randomised controlled trial. The Lancet, 385(9966), 421-429. doi:10.1016/S0140-6736(14)60998-3






This article was so helpful. Thank you. I have been having pain in my finger joins for over a year now. I don’t think my symptoms add up to 6 points or more currently, but I will definitely be keeping an eye on the situation. Thanks again.