


ACL Surgery: Return to Sport Testing

ACL Surgery: Return to Sport Testing
The rehabilitation process for an ACL reconstruction is long and arduous. Imagine you’ve put in the hard work for 9+ months and the day has arrived that you get the tick of approval to return to your beloved sport. You would want to feel confident that working with your physiotherapist has prepared you well enough to recommence play. This is exactly where return to sport testing comes into play.
What is Return to Sport Testing?
There’s no doubt that an ACL rupture is a life-altering injury in multiple aspects both physically and psychologically. We know that only around 65% of patients will return to their pre-injury level of competitive sport within the 2 years after surgery. Only 38% remain at this level of sport past 2 years (6). That’s pretty low odds that an athlete will return to their former performance long-term. I do not mean to be doom-and-gloom but again there is no doubt that ACL reconstructions have a big impact on people.
Return to Sport (RTS) is the return to unrestricted training or play so think of the testing as the final hurdle to clear before getting back on the field. RTS should be differentiated from clinical tests where the physio is looking at a certain clinical measure (knee range of motion, joint laxity etc.). RTS testing is looking at functional performance and the system working as a whole. The aim is to objectively measure the athletes’ readiness to return to sport participation.
Why is it important?
Despite extensive rehabilitation, there is still a risk of a subsequent ACL injury when an athlete returns to sport. A 2014 study showed that people who had ACL reconstructive surgery and returned to cutting/pivoting sports were at 6-times higher risk of an ACL injury than other athletes, for up to 2 years post-surgery (7). Interestingly of the 29.5% of athletes with repeat ACL injuries, 20.5% occurred on the opposite leg and 9% on the previously injured knee.
RTS performance tests allow the clinician and athlete to perform sports specific movements in a controlled environment prior to an unpredictable game scenario. When the athlete passes or fails these tests, it gives a clear indication of whether or not they are physically prepared for their sport. A 2016 study found that athletes who did not meet 6 common clinical RTS tests before returning to sport were 4-times more likely to have a subsequent ACL rupture (3). Another study also found that 38.2 % of those who failed RTS criteria suffered reinjuries versus 5.6 % of those who passed when returning to cutting / pivoting sports (level 1 sport) (1).
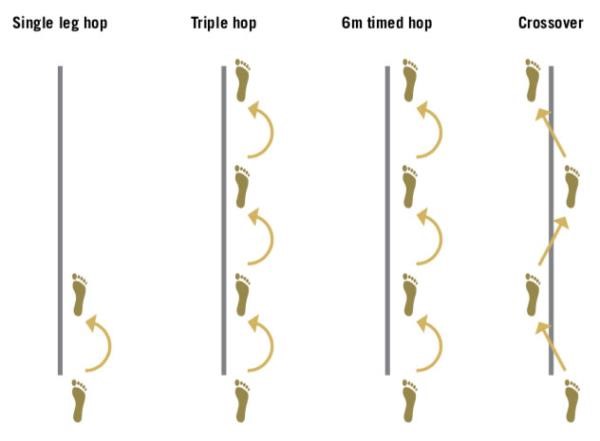
Image: commonly used hop test measures for RTS post-ACLR
What does it involve?
Theoretically, RTS tests can be any functional movement that mimics that of the athlete’s sport. Luckily for us there are some clearly defined RTS tests that have good evidence in the scientific literature.
Hop Tests
Hop testing is used as the main performance measure for RTS. It can include between 4-6 different hop and jump tasks. The aim is to achieve maximum values on all tests, comparing surgical side to normal side and aiming for >90-95% limb symmetry. The most commonly used in the research are:
- Single Hop Test
- Triple Hop Test
- Cross Over Hop Test
- 6m Timed Hop Test
- Side Hop Test
Video: 4 hop test cluster being performed and key assessments
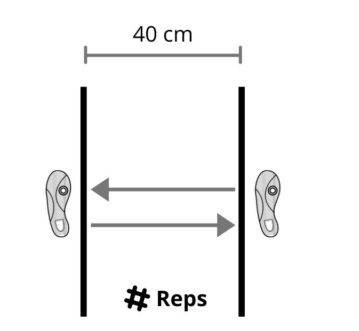
Image: 40cm side hop test set out.
Quadriceps Strength
Grindem 2016 found that of the RTS battery of tests used (including hop tests and muscle strength), the quadriceps strength deficit prior to RTS was a significant predictor of knee reinjury. In this study, 33% of patients who had <90% quads limb symmetry suffered an injury compared to only 12% who had >90% limb symmetry. Low quads strength following ACL-R also translates to reduced performance with hop testing and functional performance (4).
In research, this is generally tested on an isokinetic testing machine like a Biodex however this is hard to replicate in a clinical setting. At POGO Physio we use both hand-held dynamometry and gym equipment testing.


Image: Biodex machine for isokinetic testing (left), hand held dynamometer (right)
Agility T-Drill
An agility T-Drill should be able to be performed in under 11 seconds.
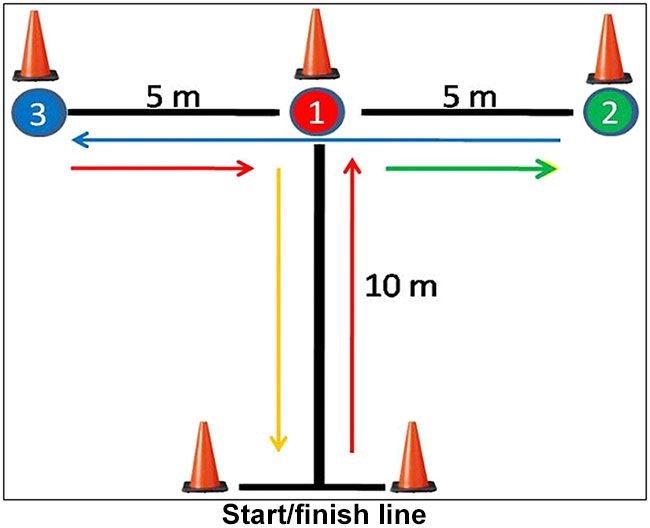
Image: agility T-drill set up
Sports Specific Drills
If the above evidence based RTS tests are cleared then it is also appropriate to implement testing that is specific to the athlete’s requirements. Whilst the above tests are commonly used in research they don’t replicate all sporting movements. This could include particular kicking, cutting/stepping, jumping, or any relevant functional tests for the individual athlete.
Potential Problems of RTS Testing
Whilst RTS testing is an extremely important part of rehab, we know that Limb Symmetry Index (LSI) overestimates knee function post-surgery. The down side of LSI is that the post-surgical leg is compared to the non-surgical leg that has also been immobilised or offloaded during the post-op period. So therefore we are comparing against an already reduced benchmark. To combat this it has been suggested that the EPIC system should be implemented. This stands for Estimated Preinjury Capacity. The EPIC system takes benchmarks from the uninjured leg preoperatively prior to the muscle strength and function declines post-surgery (5).
The 2017 study found that at 2 year follow up:
- At 6 months post-op; only 28% of patients met >90% EPIC criteria on all the strength and hop tests, however 57% achieved >90% LSI criteria on the strength and hop tests
- 11 of the 70 patients (15%) sustained a 2nd ACL injury during the 2 year follow up period
- 8 out of the 11 passed the >90% LSI criteria on all strength and hop tests at 6 months post-op
- 6 of these 8 however, did not pass the >90% EPIC criteria on all strength and hop tests at 6 months post-op
- Conclusion: >90% EPIC criteria was superior in predicting 2nd ACL injuries than the current method of >90% LSI. (2)
Does timing of RTS matter?
Yes, it does and 9-months seems to be the golden number. Any return to sport prior to 9-months puts the athlete at increased reinjury risk. In that first 9 months post-op, for every month RTS is delayed, reinjury risk decreases by 51%. Between 9-23 months post-op, there is no significant difference in injury risk solely due to time alone (1).
Psychology: Not just strength and performance!
More recently there has been a greater appreciation for the psychological aspects of RTS and their impact following ACL rehab. It is not surprising that after a traumatic injury, followed by a lengthy ‘protection’ and rehabilitation process that people have changed perceptions about their knee function, and this can inhibit their RTS.
It’s been reported up to 82% of patients have some level of reduced knee confidence with one quarter being very fearful of movement. Even 12 months post-surgery half of patients may have negative psychological readiness to return-to-sport. This tells us that there has been a severe change to people’s own self-confidence. Higher levels of fear of movement and fear of re-injury translate to poorer patient-reported function at the one year mark whereas higher positive psychological return to sport readiness is associated with better function and greater odds of returning to pivoting sports one year after (8).
Conclusion
RTS testing has been developed to ensure athletes are physically and mentally ready to return to sport following their rehab. Whilst we know passing RTS testing greatly reduces risk of injury there is always a risk of injury when playing sport. In a period that can be filled with uncertainty, RTS should provide some objectivity that your knee is good to go!

James Gardiner
POGO Physiotherapist
Book an Appointment with James here.
Featured in the Top 50 Physical Therapy Blog
References
- Grindem, H., Snyder-Mackler, L., Moksnes, H., Engebretsen, L., & Risberg, M. A. (2016). Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. British journal of sports medicine, 50(13), 804–808.
- Hughes, M. (2017, July 13). ACL Rehab: Make it EPIC! mickhughesphysio. https://www.mickhughes.physio/single-post/2017/07/13/acl-rehab-make-it-epic
- Kyritsis, P., Bahr, R., Landreau, P., Miladi, R., & Witvrouw, E. (2016). Likelihood of ACL Graft rupture: Not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. British Journal of Sports Medicine, 50(15), 946-951.
- Schmitt, L. C., Paterno, M. V., & Hewett, T. E. (2012). The impact of quadriceps femoris strength asymmetry on functional performance at return to sport following anterior cruciate ligament reconstruction. Journal of Orthopaedic & Sports Physical Therapy, 42(9), 750-759.
- Wellsandt, E., Failla, M. J., & Snyder-Mackler, L. (2017). Limb symmetry indexes can overestimate knee function after anterior cruciate ligament injury. Journal of Orthopaedic & Sports Physical Therapy, 47(5), 334-338.
- van Melick N, van Cingel REH, Brooijmans F, et alEvidence-based clinical practice update: practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensusBritish Journal of Sports Medicine 2016;50:1506-1515.
- Paterno, M. V., Rauh, M. J., Schmitt, L. C., Ford, K. R., & Hewett, T. E. (2014). Incidence of Second ACL Injuries 2 Years After Primary ACL Reconstruction and Return to Sport. The American Journal of Sports Medicine, 42(7), 1567–1573.
- Hart, H. F., Culvenor, A. G., Guermazi, A., & Crossley, K. M. (2020). Worse knee confidence, fear of movement, psychological readiness to return-to-sport and pain are associated with worse function after ACL reconstruction. Physical Therapy in Sport, 41, 1-8.






