


Hyper-Extension Elbow Injuries
Hyper-extension Elbow Injuries
I don’t think my elbow is supposed to bend like that?
Hyper-extension injuries of the elbow occur when the elbow is bent backwards beyond its normal range of motion. This places increased stress through numerous elbow structures and can cause injury to ligaments, bones and other soft tissue structures of the elbow. Hyper-extension injuries can range from minor pinching to severe pain and inability to bend the elbow.
Accurate diagnosis and early management is important to ensure full recovery and return to normal activities.
Mechanism of Elbow Hyper-extension Injury
Most hyper-extension injuries occur due to a fall from height or during sports and strenuous physical activity. The injury can occur acutely in football or throwing sports with a hyper-extension movement or commonly in martial arts after an arm-bar. Another common cause is a fall on an outstretched arm (FOOSH) in which the elbow is forced into extension, bending excessively due to the impact and body weight. This is most common during falls greater than body height.
Most hyper-extension injuries occur due 2a fall from height or during sports & strenuous activity #physio #elbow Share on X
Signs & Symptoms
With a single acute mechanism of hyper-extension symptoms will include instant pain, muscle spasm, swelling and loss of strength. In some cases, with fractures or dislocations the elbow may be deformed or the hand circulation may be affected and requires immediate medical treatment.
Hyper-extension injures can also occur gradually overtime in many throwing sports such as water polo, baseball, softball or cricket, with excessive ongoing extension or valgus (medial) stress on ligamentous structures. The injury may also occur during gymnastics as the elbow is prone to hyper-extension during handsprings and walkover stunts, particularly during fatigue. These injuries are more common with greater hyper-extension forces through the elbow and hypermobile individuals.
Click HERE to learn about your mobility status as determined by your genetics.
Symptoms that occur with a slow, gradual onset due to repetitive overload can have anterior or posterior elbow pain. Pain may be reproduced with end of range extension (or hyperextension) or during through the throwing movement.
What’s Injured?
The elbow joint is a hinge joint – moving in one plane (bending and straightening). The humerus (trochlea) articulates with the ulna (olecranon) to form the humero-ulnar joint. The humerus (capitulum) also articulates with the radius (radial head) forming the humeroradial joint. Together with an attachment between the radius and ulnar these joints form the elbow.
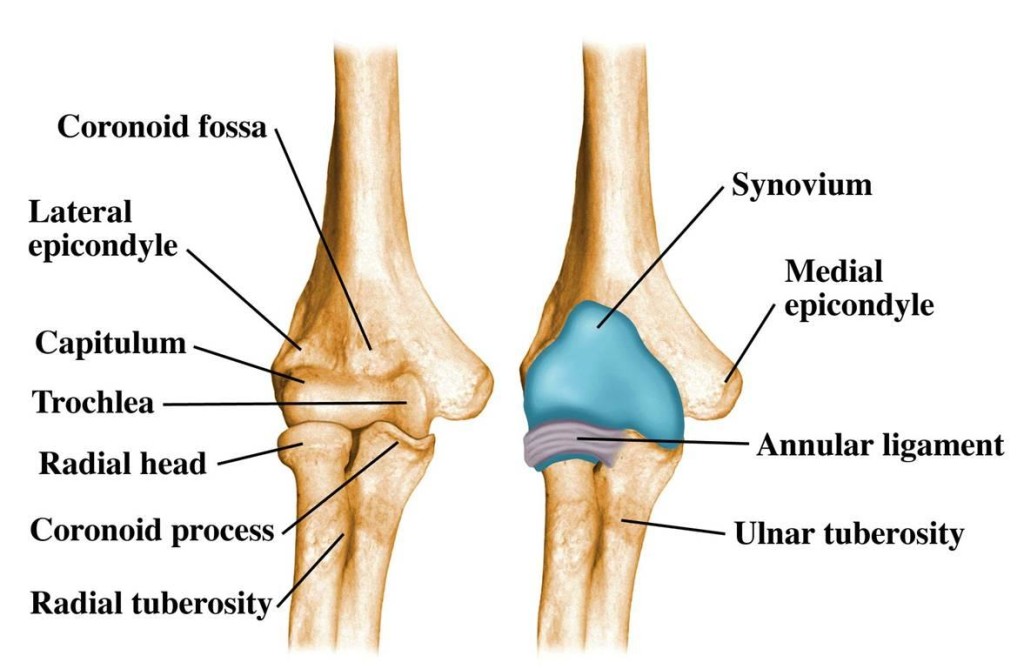
The bony anatomy of the elbow.
Ligamentous stability to the elbow is provided by 4 main structures – the joint capsule, ulnar collateral ligament, radial collateral ligament, and annular ligament. During a hyper-extension injury the anterior structures of the elbow are overstretched and the posterior structures are compressed together. Commonly the anterior joint capsule is overstretched and sprained. With increasing degrees of hyperextension the potential for tissue injury increases. High degrees of force are required to produce an elbow dislocation or fracture (5).
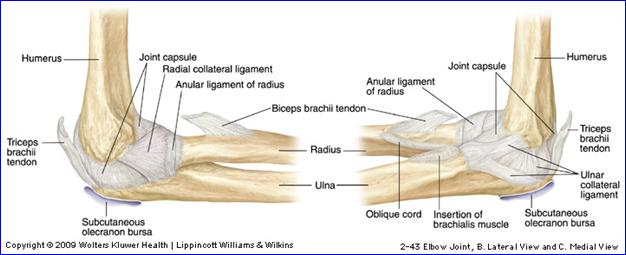
The ligamentous anatomy of the elbow
Compression of the posterior structures of the elbow is often termed posterior impingement. This abutment of bony and soft tissues in the posterior compartment of the elbow can arise from repetitive microtraumatic processes, such as increased hyperextension and valgus forces on the elbow or a single traumatic event. This can result in posterior elbow pain, loss of full elbow movement, locking, and crepitation (noises), particularly at the limits of elbow extension.
Pathology can be then present at the articular (joint) surfaces of the posterior trochlea and the anterior, medial olecranon in the form of oedema, synovitis and/or cartilage defects. These changes can also be coupled with injury to the anterior compartment, such as loose bodies and degenerative chondromalacia (softening of the cartilage) of the radio-capitellar joint. Posterior impingement of the elbow can be the primary cause leading to clinical presentation or it can be a secondary result of pathology. Both aspects should be addressed as part of a comprehensive treatment plan (1, 2).
Treatment of Elbow Hyper-Exetension Injuries
If an acute elbow hyper-extension injury occurs, with strong pain and notable deformity immediate medical management should occur. Immobilization of the elbow and x-ray can be utilised to rule out fracture and or dislocation.
If an acute elbow hyper-extension injury occurs, with strong pain & deformity immediate medical management should occur #physio #elbow #injury Share on X
Immediate Management
Immediate treatment options include ice or cold therapy and compression to reduce swelling and pain. Rest from aggravating activities and immobilization of the elbow joint in a brace may be necessary. In severe cases, surgery may be required if structures to the elbow joint have been completely torn, fractured, or severely injured.
Physiotherapy Management
Physiotherapy management may incorporate numerous joint mobilisations and soft tissue techniques to assist in restoring full of range of movement. Taping and bracing may be utilised to reduce and minimise hyper-extension forces. This will often be used in a comprehensive rehabilitation program to strengthen muscles controlling the elbow, particularly the triceps. For hyper-extension injuries caused by repetitive micro-trauma (overload) assessment of technique is necessary to optimise rehabiltation and technique changes to prevent re-occurrence.
Lewis Craig (APAM)
Physiotherapist

References
- Moskal, M. J. (2001). Arthroscopic treatment of posterior impingement of the elbow in athletes. Clinics in sports medicine, 20(1), 11-24.
- Brukner, P. D. & Khan, K. (2007). Clinical Sports Medicine (3rd). McGraw-Hill, Sydney.
- Eygendaal, D., & Safran, M. R. (2006). Postero-medial elbow problems in the adult athlete. British journal of sports medicine, 40(5), 430-434.
- Cohen, S. B., Valko, C., Zoga, A., Dodson, C. C., & Ciccotti, M. G. (2011). Posteromedial elbow impingement: magnetic resonance imaging findings in overhead throwing athletes and results of arthroscopic treatment. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 27(10), 1364-1370.
- Moore, K. L., Dalley, A. F., & Agur, A. M. (2013). Clinically oriented anatomy. Lippincott Williams & Wilkins.






