Patella Tendinopathy in Adolescents
Patella Tendinopathy in Adolescents
Patella tendinopathy is a common injury which affects the knees. This injury occurs as a result of overloading the patella tendon (knee-cap tendon) or forceful/repetitive contraction of the quadriceps muscle (Kerssemakers, Fotiadou, De Jonge, Karantanas & Maas, 2009).
Patella tendinopathy was first referred to as ‘Jumpers Knee’ as the prevalence of this condition was high in sports with jumping such as, volleyball, basketball, long jump, triple jump and high jump (Brukner & Khan, 2006). This condition is very common in the aforementioned sports as well as in sports where athletes change direction (Brukner & Khan, 2006).
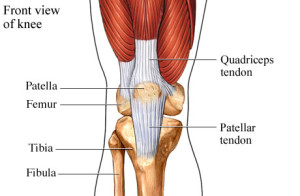
The patella tendon can become painful in its middle (mid-portion) or the insertion into the shin bone (tibial tubercle) or from it’s origin at the base of the patella.
Patella tendinopathy in adolescents
It was first thought that patella tendinopathy was a condition in those aged twenty years or over however this condition has now been recognized in a much younger population (Cook, Khan, Kiss, Purdam & Griffiths, 2000). In the study written by Cook, Khan, Kiss & Griffiths in 2000, they found that 7% of fourteen-eighteen year olds have patella tendinopathy.
Patella tendinopathy in adolescents mainly presents in two types of ways:
-
Osgood-Schlatter syndrome.
This usually affects children around 10 to 15 years of age. It results from excessive traction of the patella tendon on the bony prominence of the tibia/shin bone. One chief reason for this excessive traction can be due to the child or adolescent growing rapidly with and bones that have no yet ossified or reached bone maturity. Therefore, while doing high levels of activity, during a rapid time of growth, the tendon will be pulling on the soft apophysis and potentially cause pain (Brukner & Khan, 2006).
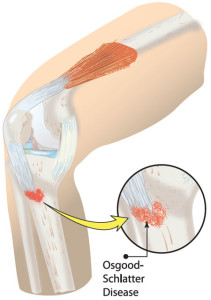
The region of pain of Osgood Schlatter syndrome/’disease’ affecting active adolescents.
-
Sinding-Larsen-Johansson syndrome
Sinding-Larsen-Johansson syndrome is also a self-limiting condition in adolescents where the same pressure and traction forces as experienced by adolescents suffering from Osgood-Schlatter syndrome, can in essence ‘pull’ on the inferior pole of the patella (knee-cap). The area of pain differs from Osgood-Schlatter in that the pain is on the inferior pole of the patella instead of on the tibial tuberosity (Brukner & Khan, 2006).

The region of pain for those suffering from Sinding Larson syndrome of the patella tendon, compared with the region of pain of Osgood Schlatter pain.
The presentation of anterior knee pain in adolescent athletes is relatively common. Patella femoral pain syndrome (knee cap pain) is the most common cause however, Sinding-Larson Johannsen and Osgood Shclatter syndromes are important differential diagnosis’s (Brukner & Khan, 1993). As a patella tendinopathy has a poorer prognosis than that of patella-femoral pain syndrome it is important that this condition is placed highly in therapists differential diagnosis lists as recognizing this condition and treating it sooner is imperative in order to get the young athlete back on the court, track, pool or whatever sport they are partaking in as soon as possible.
Typically patella tendinopathy has a poorer prognosis than that of patella-femoral pain in adolescents #physio #kneepain Share on X
Misdiagnosis can lead to impairment and possible irreversible damage (Kerssemakers, Fotiadou, De Jonge, Karantanas & Maas, 2009).
How to Detect Patella Tendinopathy
Objective signs of patella tendinopathy are anterior knee pain while changing direction and decelerating. The most tender area on patients is usually the inferior pole of the patella (knee cap) or tibial tuberosity (bony prominence on top of calf bone). The tendon as well as inferior pole of the knee cap usually feels very tender on palpation (pressure applied to the area). Sometimes the physiotherapist may feel thickening of the tendon on the affected side in comparison to the other side.
Imaging with diagnostic ultrasound, doppler ultrasound, MRI, or event UTC (ultrasound tissue characterisation) can be useful in confirming at times multiple pathology (eg fat pad irritation of the knee in combination with co-existing patella tendinopathy).Imaging can be particularly useful in confirming the prognosis based on the degree of patella tendinopathy present.
Factors Contributing to the Development of Patella Tendinopathy
There are a number of factors that may predispose adolescents to developing a patella tendinopathy. These factors can include the following:
- weakness in the calves, gluteal muscles, and quadriceps.
- Shortening of the calf muscles can also be a predisposing factor(Brukner & Khan, 2006).
- quadriceps (quads) muscle tightness.
- There are objective functional measures that can be assessed to load up the patella tendon as well. These measures include, jumping, a decline squat (patient has heels up on wedge), and a hop. These few functional tests are actually superior to palpation when monitoring the patient’s progress with rehabilitation (Brukner & Khan, 2006).
Physiotherapy Treatment of Patella Tendinopathy
The treatment for a patella tendinopathy in the adolescent population differs from the adult population in the fact that the condition is ‘self-limiting’ (will resolve with time and activity reduction).
Activity modification is important in this population as this helps to reduce the patients pain (and loading on the patella tendon), however this does not help to quicken the healing process.
Pain should, very much be what guides the patient in what they can and cannot participate in when it comes to sport and physical activity (Brukner & Khan, 2006).
For a guide on how to interpret the pain experienced while exercising pain click HERE.
Ice and isometric quadriceps loading (for example the wall sit) are helpful to reduce symptoms initially and with flair ups. Additionally, addressing bio-mechanical predisposing factors or weakness should be a part of a thorough rehabilitation plan.
See below for a video demonstration of how to perform a wall squat isometric hold for patella tendinopathy treatment.
Vianna Ross (MPhysio, B.A PhEd)
Physiotherapist

References
1.Brukner, P., & Khan, K. (2006). Clinical sports medicine. McGraw Hill.
2. Cook, J. L., Khan, K. M., Kiss, Z. S., Purdam, C. R., & Griffiths, L. (2000). Prospective imaging study of asymptomatic patellar tendinopathy in elite junior basketball players. Journal of Ultrasound in Medicine, 19(7), 473-479.
3. Cook, J. L., Khan, K. M., Kiss, Z. S., & Griffiths, L. (2000). Patellar tendinopathy in junior basketball players: a controlled clinical and ultrasonographic study of 268 patellar tendons in players aged 14–18 years.Scandinavian journal of medicine & science in sports, 10(4), 216-220.
4. De Carlo, M., & Armstrong, B. (2010). Rehabilitation of the knee following sports injury. Clinics in sports medicine, 29(1), 81-106.
Kerssemakers, S. P., Fotiadou, A. N., de Jonge, M. C., Karantanas, A. H., & Maas, M. (2009). Sport injuries in the paediatric and adolescent patient: a growing problem. Pediatric radiology, 39(5), 471-484.