Gluteal tendinopathy is thought to be the primary cause of lateral hip pain.1 That is, pain localised to the bony prominence on the outside aspect of the hip (the greater trochanter).
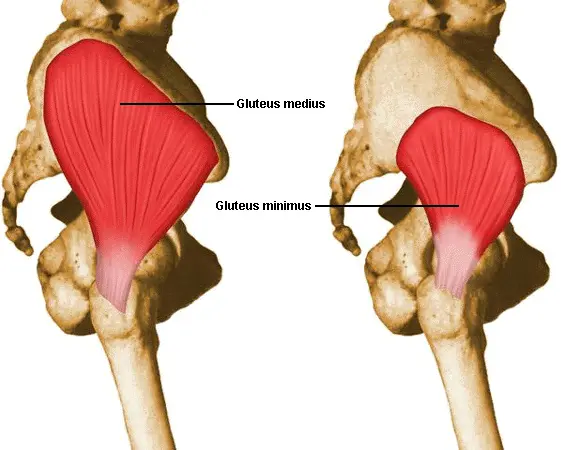
Tendons connect muscles to bone. Simply put, the term tendinopathy refers to persistent tendon pain and loss of function related to mechanical loading of these tendons. In the context of gluteal tendinopathy, the implicated tendons are those of gluteus minimus and gluteus medius (see Figure 1), two muscles that attach between the pelvis and leg. They work together to move the thigh out sideways (abduct), internally rotate the hip, and provide pelvic stability by stopping the pelvis from dropping during activities with periods of single stance (see Figure 2), such as walking.
Many readers may be more familiar with other historical terms used to refer to the gluteal tendinopathy such as trochanteric bursitis, or umbrella terms such as greater trochanteric pain syndrome. While such terms are still commonly used, the most prevalent pathology in those with lateral hip pain is now understood to be gluteal tendinopathy and hence the condition is more accurately referred to by this name.
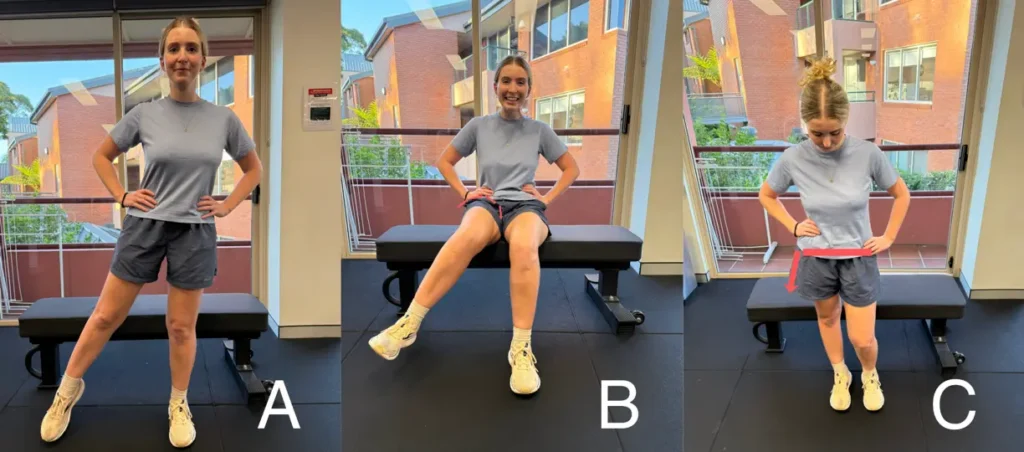
A. Abduction. B. Internal rotation. C. Pelvic stability.
It is important to note that other structures around the hip can cause pain and coincide with the presence of gluteal tendinopathy. The most common perhaps, is the trochanteric bursa, which is a fluid-filled sac that sits between the gluteus medius/minimus tendons and iliotibial band, serving to reduce friction between these structures during tasks such as walking, and running. If this bursa becomes irritates and inflamed (trochanteric bursitis), it too can contribute to pain. In fact, in the 1920’s this was the first understood cause of lateral hip pain, and hence the condition was first referred to as trochanteric bursitis as mentioned above.2 Other smaller, surrounding bursae such the sub-gluteus medius bursa or sub-gluteus minimus bursa may also become inflamed and contribute to lateral hip pain. Additionally, the iliotibial band has observed to thicken in some individuals with gluteal tendinopathy and may also contribute to lateral hip pain.3 See Figure 3, where the greater trochanteric bursa and iliotibial band are shown in relation to the other hip structures.

Two MRI-based studies by Blankenbaker et al. (2008)4 and Lange et al. (2022)5 found the incidence of trochanteric bursitis in those with lateral hip pain to be between 20-30%. Isolated trochanteric bursitis without the presence of gluteal tendinopathy was as low at 2-8% in those with lateral hip pain.
Gluteal Tendinopathy Pathophysiology
Moving forward in this blog, it is important to understand exactly how tendinopathy of the gluteus medius and gluteus minimus tendons develops. This will not only be of aid in understanding what factors contribute to the experience of lateral hip pain, but what strategies can be implemented to reduce it.
As previously mentioned, tendons connect muscles to bone. They are formed collagen fibres arranged in a parallel, longitudinal fashion. The development of tendinopathy (tendon pain and reduced function during mechanical loading) in the gluteus medius and gluteus minimus tendons is thought to be a product of excessive compression and/or tensile loads exerted through the tendons.
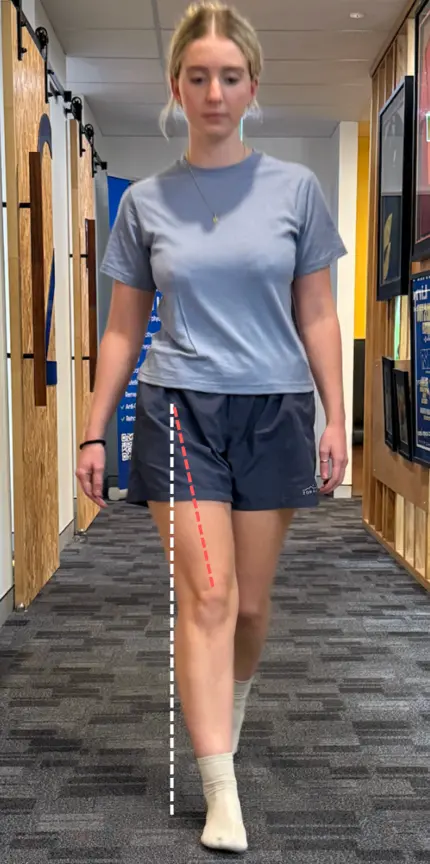
Compression occurs as the tendons are ‘squished’ between different structures in the lateral hip mentioned above, including the greater trochanter and iliotibial band. Compression of the gluteal tendons is greatest in positions of hip adduction.6 That is, when the thigh is moved across, towards the mid-line of the body (see Figure 4). This position of adduction can occur during many positions of standing and sitting, as well as daily activities (more on this below). Compression may also be increased by the orientation of, or bony abnormalities of the greater trochanter, such as coxa vera.
Tensile force describes the ‘pull’ exerted on the tendons during the action of the gluteus medius and gluteus minimus, to abduct and internally rotate the hip, and stabilise the pelvis during single stance. Throughout these actions, tensile forces are exerted by the muscles through longitudinally-orientated tendons.
While the tough collagen connective tissue that forms tendons is designed to help them withstand these compressive and tensile forces, tendons become at risk of tendinopathy when exposed to a relative overload or underload of these forces. More on this soon!
Tendinopathy (pain and loss of function related to mechanical loading) occurs on a continuum from reactive (acute incidence in which the tendons’ connective tissue proliferates) to degenerative (chronic incidence with irreversible changes to the tendons’ connective tissue matrix). However, the relationship between tendon structure and function, and the experience of tendon pain is still not fully understood.7 Individuals with chronic tendinopathy can still drastically improve their symptoms with targeted management. To read more on tendinopathy and its characterised continuum of stages, click this link.
High Risk Populations
There are key populations who are most ‘at-risk’ of developing gluteal tendinopathy, which are important to consider in the context of forming a diagnosis.
Peri- and post-menopausal women
The biggest population that experiences gluteal tendinopathy is undoubtably peri- and post-menopausal women. Gluteal tendinopathy has been observed to affect up to 25% of women over the age of 50, and is 2-4x more common in females than males above this age.8 The wider morphology (structure) of the female pelvis has historically been hypothesised as a strong risk factor for developing gluteal tendinopathy, as it increases the compressive loads put on the gluteus medius and gluteus minimus tendons.9 However, the considerable decline and low circulating levels of oestrogen associated with menopause has been identified as another strong driver of gluteal tendinopathy in this population. Oestrogen is an important hormone for maintaining tendon health in women. As such, low levels during and after menopause contribute to reductions in collagen synthesis and tensile strength in tendons, which contributes to the increased risk of gluteal tendinopathy occurring.10 Reductions in activities levels at this age may also contribute to the increased risk of gluteal tendinopathy occurring (remember, tendons become at risk of tendinopathy when exposed to a relative overload or underload of compressive and/or tensile forces).11
Women after childbirth
Women also appear to show higher rates of gluteal tendinopathy after childbirth. While there is a lack of evidence examining the mechanisms for this, the increased risk can be practically theorised from our current understanding of tendinopathy. Pregnancy (particularly the late-stage) often involves a relative de-loading of the gluteus minimus and medius, followed by a rapid re-loading with childcare and return daily tasks. When this re-loading exceeds the reduced tendons’ capacity, tendinopathy can develop. Additionally, hormonally driven ligamentous laxity associated with pregnancy may reduce pelvic stability, increasing the demand placed on the gluteus medius and minimus tendons to control the pelvis.
Trail runners
The final population that more commonly experiences gluteal tendinopathy are trail runners. The steep gradients of certain trails can increase the tensile loads placed through the gluteus medius and minimus tendons, and the often narrow path of trails force runners to recurrently enter positions of adduction, which increase compressive forces on the tendons too. It is also likely the uneven terrain of trails require greater pelvic stabilisation, increasing gluteus medius and minimus recruitment and reducing recovery time, thereby elevating load on the gluteal tendons.
Clinical Assessment
Subjective
To diagnose gluteal tendinopathy, a clinician should first listen closely for subjective ‘clues’ as discussed above. This may pertain to an individual reporting focal pain that they can ‘put their finger on’, and pain that is aggravated in positions of adduction or single-stance activities (e.g., walking, stairs). Additionally, the typical behaviour of tendinopathy can help guide an accurate diagnosis: pain that is load-dependent, improves (‘warms up’) with activity but worsens afterward, and is preceded by a change in training routine or activity levels.
Considering the patient’s demographic and daily activities will also further inform clinical suspicion. For example, are they an at-risk population (e.g., post-menopausal women or trail runners)?
Objective
Objectively, numerous physical assessments can be utilised to confirm a diagnosis of gluteal tendinopathy.
The single-leg stance test (see Figure 5) is perhaps the first test many clinicians will employ. In this test, a patient is directed to stand on their symptomatic leg for 30 seconds and is only permitted to use one finger against a wall for balance (as to not take any weight through their hand). A positive result (i.e., a result suggesting the presence of gluteal tendinopathy) is reproduction of the patient’s familiar pain over the greater trochanter within 30 seconds. It is useful to pay attention to how quickly an individual’s pain is reproduced, as those with more severe gluteal tendinopathy will experience the onset of their pain much earlier than those with less severe cases. The single leg stance has demonstrated high specificity, making it helpful to rule in gluteal tendinopathy when a test is positive.12 However, the test is less useful to rule out the condition, in the context of a negative (not painful) result.
The FADER (flexion, adduction, external rotation) test is another highly specific test (see Figure 5),12 performed with the patient in a supine lying position. The clinician will bring the patient’s relaxed affected leg into a FADER position, which winds the iliotibial band over the greater trochanter and thus, compresses the gluteal tendons. A positive test is again, reproduction of the patient’s familiar pain over the greater trochanter. If no symptoms are reproduced, the test can be progressed to help ensure a ‘true negative’ by asking the patient to actively resist the external rotation component (FADER-R test). This adds a tensile load to the existing compressive force, which would help to sensitise a symptomatic tendon and provoke the patient’s familiar pain if they truly do have gluteal tendinopathy.
Passive hip adduction (see Figure 5) in side-lying can also be progressed in a similar fashion to the FADER test, by asking the patient to resist against the passive adduction. Both variations bear a similar diagnostic value to the FADER and FADER-R tests, with high specificity.12
The FABER (flexion, abduction, external rotation) test is used less frequently by clinicians (see figure 5),13 as it can provoke symptoms from multiple structures. In the context of gluteal tendinopathy however, it is helpful for identifying a potential coexisting intra-articular hip (hip joint) pathology, such as osteoarthritis. Isolated gluteal tendinopathy should not restrict FABER range of motion so therefore, reproduction of familiar greater trochanteric pain in combination with reduced range compared to the unaffected leg hints at a concurrent hip joint issue.14

A. Single-leg stance test
B. FADER test (+/- resistance)
C. FABER test
D. Passive hip adduction (+/- resistance)
Tenderness on palpation at the gluteal tendon insertion on the greater trochanter is the cardinal clinical sign of gluteal tendinopathy. As palpation is highly sensitive (and local tenderness can be present even in the absence of pathology)¹², the absence of tenderness makes gluteal tendinopathy unlikely. For these reasons, palpation is best performed last to avoid unnecessary tendon sensitisation and potential confirmation bias. When palpation reproduces the patient’s familiar pain and at least one active tendon-loading test (e.g., single-leg stance, FADER-R, ADD-R) is also positive, the likelihood of gluteal tendinopathy is high.12 Clinicians should therefore utilise a battery of tests, both highly sensitive and specific, to reduce the risk of diagnostic errors.
Differential Diagnoses
On the note of diagnostic errors, it is useful to quickly touch on common differential diagnoses. These are conditions that commonly cause pain in the lateral hip and may therefore be mistaken as gluteal tendinopathy, or alternatively mask the presence of gluteal tendinopathy.
The two primary differential diagnoses are: intra-articular hip (hip joint) pathologies and back pain.
Hip joint pathologies, such as osteoarthritis, femoroacetabular impingement (FAI), and labral tears may refer pain laterally to the same area as gluteal tendinopathy and should be considered during examination. These conditions are more likely when groin pain, reduced hip joint range of motion, and pain reproduced with intra-articular tests (e.g., FADIR) are also present.
Back pain includes somatic referral from the lower back into the hip area, and radiculopathies of nerves relaying sensory information from the hip area (L2-S1). A clinician may identify the lower back as a source of symptoms when pain is influenced by spinal movements/positions, or when neurological signs such as sensory change, myotomal weakness, or altered reflexes are identified in the lower extremity.
Management
The management of gluteal tendinopathy requires a multi-faceted approach. Exercise prescription should not be the sole treatment of the condition, especially initially. Once gluteal tendinopathy is identified and diagnosed, there are two aspects to management the clinician must ensure are provided.
- Education + guidance for managing load and provocative activities/positions.
- A structured exercise program.
These two components have been demonstrated as an effective first-line intervention for gluteal tendinopathy. For example, the LatErAl hiP pain (LEAP) trial by Mellor et al. (2018)14 compared an 8-week physiotherapist-led ‘education and exercise intervention’ at 8, 12, 26, and 52 weeks to:
- Cortisone injections.
- Wait-and-see approaches.
Approximately 80% of patients in the ‘education and exercise group’ successfully rehabilitated, compared to 50% in the other two groups.14 These results were independent of (not affected by):
- The severity of participants’ gluteal tendinopathy (both self-reported pain, and as demonstrated by MRI).
- The duration of participants’ symptoms.
- Participants’ menopausal status.
- The extent of participants’ pain catastrophising (a tendency to have heightened negative thoughts and emotional responses about pain, such as feeling helpless or expecting the pain to worsen).
Education + guidance for managing load and provocative activities/positions.
Education should be aimed at empowering the patient to gain control over their condition, which is particularly important given the substantial physical and psychological burden associated with gluteal tendinopathy.¹⁵ Effective education will provide patients with a clear understanding of the condition, the relevant contributing factors, and practical strategies to manage load through the tendons.
Within education, clinicians should immediately guide patients on how to manage load through their symptomatic tendons during provocative activities. This guidance can perhaps have the biggest impact on symptom reduction initially and provide patients with ‘quick wins’ in their pain and ability.
Advice will primarily pertain to modifying positions and activities which impose high compressive and tensile loads on the gluteal tendons, and will serve to settle down the ‘grumpy’ tendons (as well as other coinciding pain contributors, such as the greater trochanteric bursa). Dr Alison Grimaldi (physiotherapist, senior research fellow at the University of Queensland, and widely known hip-related injuries expert) has wisely stated “’Load management’ for gluteal tendinopathy encompasses more than simply reducing and then rebuilding overall volume or intensity of activity. Identifying and reducing individual exposure to excessive, repetitive, loaded and sustained hip adduction in activities of daily living and sport may be key for many patients, particularly in the longer term”.13
Three examples on modifying symptomatic activities are provided below:
1. For those who experience worsened symptoms during sleep, guidance should be provided to trial sleeping with the symptomatic side ‘up’, with multiple pillows between the knees and ankles to keep the hip in a more neutral, slightly abducted position (see Figure 6. Given many individuals have a position preference to lie their symptomatic side, another position to trial is sleeping halfway between lying on their tummy and lying on their affected side (see Figure 6). By rolling slightly forward towards their tummy, an individual will roll off their greater trochanter and reduce compression on the symptomatic tendons. Pillows can be placed underneath the stomach and thigh to prevent fully rolling forward, as demonstrated in Figure 6. Both positions will minimise and compressive forces placed on the symptomatic tendons, therefore reducing the onset of symptoms and improving the quality of sleep.

A. Sleeping with the symptomatic side ‘up’, supported by pillows between the legs to prevent the leg from dropping into adduction
B. Sleeping on the affected side, but rolling forward off the greater trochanter to ensure the gluteal tendons are not compressed (the key is to use pillows to stay supported!)
2. For those who experience pain during walking, hills, and/or stairs, gait assessment should be utilised to identify if a patient enters a position of adduction at the end of their stride on their symptom side (see Figure 4). Individuals who take long strides (overstriding) often enter this position. Cues to reduce stride length or adopt a slightly wider walking pattern can reduce compression on the gluteal tendons while they experience tension stabilising the pelvis. These cues can also be applied to trail runners with gluteal tendinopathy. By modifying these provocative activities with simple cues, we can often facilitate individuals to continue doing the physical activities they enjoy, without aggravating their symptoms.
3. For those who experience pain during sitting and standing, a clinician can draw their attention to potentially provocative sustained positions they may be adopting throughout the day (often without even realising!). Sitting in cross-legged positions (see Figure 7) will place the hip into adduction and can be easily modified. If sitting in a deeper chair is increasing the severity of symptoms, it can be addressed by adjusting the height of a chair, or by implementing frequent standing breaks. Standing while ‘hip hanging’ similarly places the hip in a relative position of adduction, as does crossing the legs (see Figure 8).
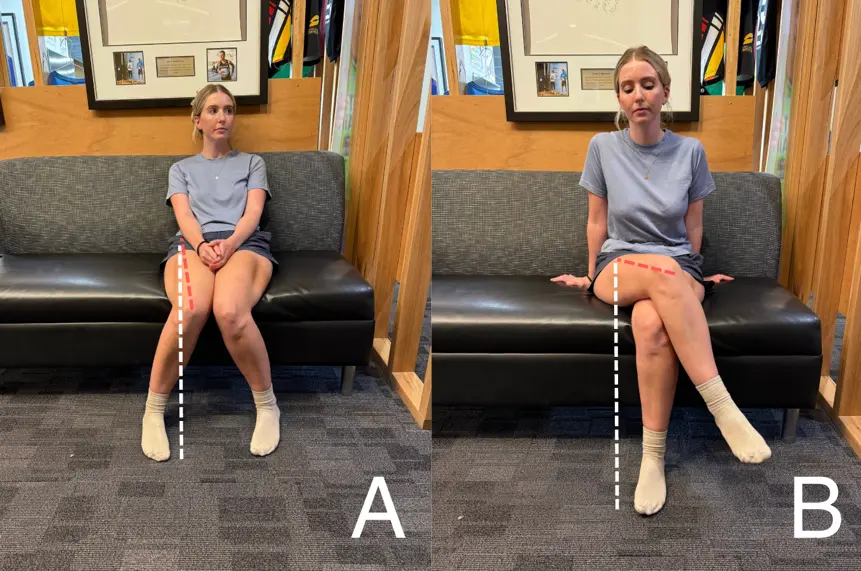
A. Rolling hips in B. Crossing the legs

A. ‘Hanging’ off the hip B. Crossing the legs
In addition to these activity modifications, patients need guidance on how much total load the tendon can tolerate (both during activities of daily life, and their structured exercise program). Rapid increases in load should be avoided, with progression of activities or exercises guided by the 24-hour symptom response. A flare-up of symptoms in the evening after or the next morning following a particular activity or exercise session is a sign that the load was too high and needs to be scaled back.16
A structured exercise program
A structured exercise program is the second component of management and is required to build the capacity of the affected tendons, to therefore reduce symptoms. Exercises must target the gluteus minimus and medius, and commence at low loads, before being progressed as symptoms tolerate.
The following information is largely based on the exercise protocol of the LEAP trial mentioned above, a large study which demonstrated the greater efficacy of an education + exercise approach to managing gluteal tendinopathy, when compared to cortisone injections, and wait-and-see approaches.14 In this trial, the effective exercise prescription included:
- Low-load isometrics.
- Functional loading exercises.
- Abduction loading in the frontal plane.
Low-load isometrics
An exercise approach commonly commences with low-load isometric exercises. Isometric exercises involve contracting a muscle without it lengthening or shortening (easily understood as a ‘static hold’). To target the gluteus minimus and medius, an isometric into a position of abduction is required. A prescribed isometric exercise may thus involve standing in a slightly widened stance (to avoid adduction) and pushing out against the floor (‘pushing the floor apart’), as demonstrated in Figure 9. Another position may be in supine lying, pushing the legs out against a resistance band tied around the ankles, as demonstrated in Figure 9. While the exact instructions for any particular individual should be guided by a physiotherapist, a ‘low-load’ prescription may involve slowly activating the muscles, holding for 5-10 seconds, for 10 repetitions, twice a day. These exercises can provide pain-relief for many patients and are intended to solely engage the gluteus minimus and medius when performed appropriately.

A. Pushing out against the floor
B. Supine resistance band push outs
Functional loading exercises
In addition to commencing isometric, a physiotherapist will introduce functional loading exercises. These are exercises where the feet are in contact with the ground and the gluteus minimus and medius work to stabilise the pelvis, as required throughout common daily activities (see Figure 2 and 4). Activation of gluteus minimus and medius is maximised when the foot remains in contact with the ground during these exercises, as lifting the foot is thought to recruit additional hip muscles, such as the tensor fasciae latae.17 Accordingly, the improvement of load capacity through the symptomatic tendons of gluteus minimus and medius is maximised.
Functional loading exercises includes bridges and squats (see Figure 10). As an individual improves their strength and load capacity of the gluteus minimus and medius tendons, these exercises can be progressed by either intensity (e.g., adding weights) and volume (more sets or repetitions), or by modifications that challenge the pelvic stability function of the gluteal tendons further (e.g., performing on one leg). A rating of perceived exertion (RPE) of at least 5 of 10 (0 = no challenge; 10 = maximal effort) can be used to gauge whether these exercises are appropriately challenging. For populations that wish to return to activities of greater demand of the gluteal tendons (e.g., trail runners, younger athletes), a therapist progress functional loading exercises further to landing or change of direction during running, depending on the required demands of such patients.
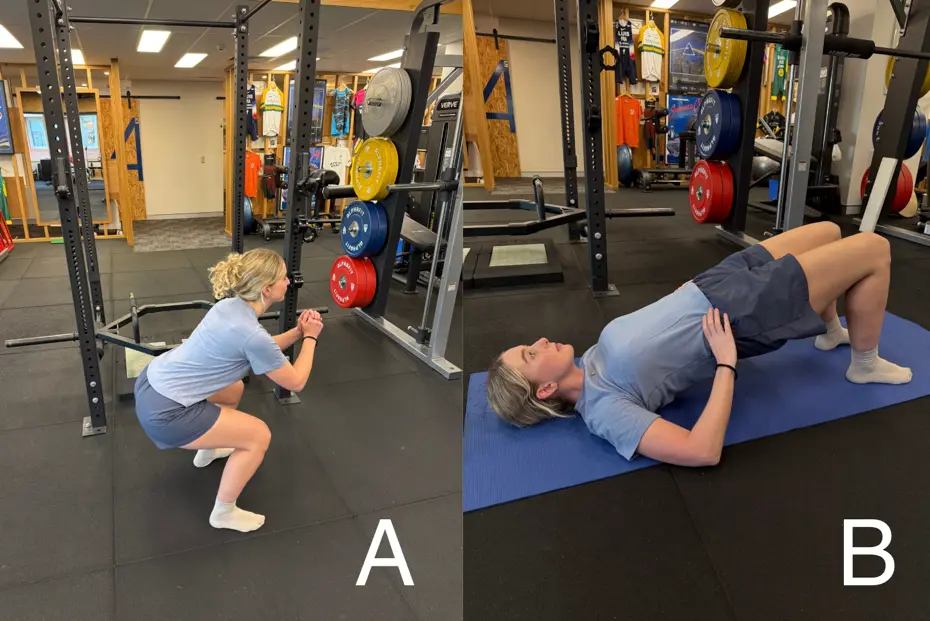
A. Squat
B. Bridge
Abduction loading in the frontal plane
The final component of the exercise program involves targeted abduction loading in the frontal plane. Unlike isometric exercises, these movements involve movement of the hip (gluteal muscles shortening and lengthening). Their aim is to further develop load capacity in the gluteal tendons by directly training their movement role of hip abduction, rather than their pelvic stabilisation role. Ideally, these exercises should be moderately to heavily loaded (RPE >5/10) and in a weight-bearing position, which makes pilates reformers (such as those in the POGO Physio gym) a perfect tool. Standing on a reformer which provides spring-loaded resistance and pushing the legs apart is a great way to load the gluteal tendons in an abduction movement (see Figure 11). Another exercise option involves sliding the foot out along the ground with a resistance band around the ankles (see Figure 11) This requires a slippery surface (e.g., wooden floorboards or tiles) and slippery socks. Patients should keep the foot in contact with the ground at all times to minimise activation of surrounding muscles such as the tensor fasciae latae. As the exercise is performed on a slippery surface, I recommend holding onto a stable object such as a bench or wall for safety, or seeking access to a pilates reformer!

A. Abduction floor slides
B. ‘Skaters’ on a pilates reformer
For all these types of exercises (isometrics, functional loading, abduction loading in the frontal plane), the prescription will generally be lower load and progressive increase as an individual builds capacity in their gluteal tendons. Because of the lower load initially, exercises are generally performed more frequently (commonly daily) to ensure meaningful improvements are achieved. Many patients may find it tedious or overwhelming to be consistent on a daily basis. However, as symptoms quickly improve and the intensity and volume of exercises increase in each session, the amount of days per week rehabilitation needs to be performed will reduce to ensure appropriate recovery between sessions. A final stage of rehabilitation may involve exercises performed as infrequently as once or twice a week!
What if symptoms don’t improve? Injections? Surgery?
As physiotherapists, if a patient comes in for review and reports no improvements or even worsening in symptoms, it is important to first double check adherence to guidance on load management and the individual’s form during prescribed exercises. A lot of the exercises may actually be provocative for the gluteal tendons if the patient is crossing into adduction, or letting the pelvis drop on the opposite side (both compressing the gluteus minimus and medius tendons). If form is good, the dose (intensity, volume, progression) of exercises may be too high in the context of the patient’s daily loading of the tendon. Therefore, either the exercises or daily activities completed by a patient will need to be modified.
Cortisone injections are often the first line medical treatment for lateral hip pain, or are used when exercise therapy is not effective (though this may be due to easily modifiable factors as just discussed). The corticosteroids of these injections rapidly, but temporarily, reduce inflammation and pain. With reference to lateral hip pain, most target the greater trochanteric bursa (as a coinciding pain contributor), though do also affect the surrounding gluteal tendons. However, there are multiple risks of cortisone injections which must be considered by clinicians and patients.
- Corticosteroids are toxic for tendon cells. Injections have been shown to reduce tendon cell proliferation and viability, and increased collagen disorganisation and necrosis.18 As such, the short-term pain reductions of cortisone injections should be weighed against potentially poorer long-term outcomes due to potentially reduced tendon health.
- Additionally, patients who receive a cortisone injection and experience reductions in symptoms will have a reduced perception of pain during provocative activities and are at risk of unknowingly overloading their tendon (which may make their symptoms sorer than to begin with!).
- Similarly, given the reality of human nature, those with temporarily reduced pain tend to be much less likely to complete exercises designed to improve their gluteal tendons’ capacity. This too can lead to worse symptoms than to begin with, or at least lengthen the process of completing rehabilitation successfully.
If education and exercise therapy has not led to meaningful improvements in symptoms despite best efforts from both a clinician and patient, the next step is often a referral to a GP to investigate other potential contributing factors to poor tendon health. These factors may pertain to:
- Hormonal change (often pertaining to menopause ,as discussed above).
- Metabolic factors (metabolic disorders such as type 2 diabetes impair tendon collagen turnover and healing, increasing susceptibility to tendinopathy).19
- Weight (carrying increased weight around the hip and pelvis may increase risk of gluteal tendinopathy, and may therefore be a large contributor for some individuals).9
- Psychosocial factors (some individuals’ pain may be contributed to by psychological stressors and therefore require relevant care to assist with these factors).
Surgical intervention may be considered for individuals with persistent pain and disability that do not respond to appropriate education and exercise-based management. In these cases, patients often demonstrate ongoing deficits in gluteus minimus and medius strength, which may be associated with partial or full-thickness tears of the gluteus minimus and/or medius tendons. As such, imaging may be warranted when conservative treatment has not been effective. In these cases, structural tendon tears demonstrated on imaging may be amenable to surgical repair.20
Acknowledgements
This blog includes a special acknowledgement to Dr Alison Grimaldi, physiotherapist, and Senior Research Fellow at the University of Queensland. Dr Grimaldi is widely recognised for her expertise in hip-related injuries and rehabilitation and has played a leading role in advancing clinical best practice in this area.
The knowledge Dr Grimaldi shares has greatly influenced my own clinical approach and has helped me better support many patients with hip-related pain.
This blog was inspired by Dr Grimaldi’s conversation with Brad Beer on The Physical Performance Show (Episode #360), discussing the assessment and management of gluteal tendinopathy. You can listen to the episode here.
References
- Grimaldi A, Fearon A. Gluteal Tendinopathy: Integrating Pathomechanics and Clinical Features in Its Management. J Orthop Sports Phys Ther. 2015;45(11):910-922. doi:10.2519/jospt.2015.5829
- Board TN, Hughes SJ, Freemont AJ. Trochanteric bursitis: the last great misnomer. Hip Int. Dec 5 2014;24(6):610-5. doi:10.5301/hipint.5000154
- Long SS, Surrey DE, Nazarian LN. Sonography of greater trochanteric pain syndrome and the rarity of primary bursitis. AJR Am J Roentgenol. Nov 2013;201(5):1083-6. doi:10.2214/ajr.12.10038
- Blankenbaker DG, Ullrick SR, Davis KW, De Smet AA, Haaland B, Fine JP. Correlation of MRI findings with clinical findings of trochanteric pain syndrome. Skeletal Radiol. 2008;37(10):903-9. doi:10.1007/s00256-008-0514-8
- Lange J, Tvedesøe C, Lund B, Bohn MB. Low prevalence of trochanteric bursitis in patients with refractory lateral hip pain. Dan Med J. 2022;69(7)
- Grimaldi A, Ganderton C, Nasser A. Gluteal tendinopathy masterclass: Refuting the myths and engaging with the evidence. Musculoskeletal Science and Practice. 2025;76:103253.
- Cook JL, Rio E, Purdam CR, Docking SI. Revisiting the continuum model of tendon pathology: what is its merit in clinical practice and research? Br J Sports Med. 2016;50(19):1187-1191. doi:10.1136/bjsports-2015-095422
- Dancy ME, Alexander AS, Clark CJ, et al. Gluteal Tendinopathy: Critical Analysis Review of Current Nonoperative Treatments. JBJS Rev. 2023;11(10):e23.00101. doi:10.2106/jbjs.Rvw.23.00101
- Grimaldi A, Fearon A. Gluteal Tendinopathy: Integrating Pathomechanics and Clinical Features in Its Management. J Orthop Sports Phys Ther. 2015;45(11):910-922. doi:10.2519/jospt.2015.5829
- Grimaldi DA. 10 of 12 Top Hip Papers of 2022 | Hormone therapy for GTPS. https://dralisongrimaldi.com/blog/hormone-therapy-for-gtps/
- Lin CY, Fredericson M. Greater Trochanteric Pain Syndrome: An Update on Diagnosis and Management. Curr Phys Med Rehabil Rep. 2015;3(1):60-66. doi:10.1007/s40141-014-0071-0
- Grimaldi A, Mellor R, Nicolson P, Hodges P, Bennell K, Vicenzino B. Utility of clinical tests to diagnose MRI-confirmed gluteal tendinopathy in patients presenting with lateral hip pain. Br J Sports Med. 2017;51(6):519-524. doi:10.1136/bjsports-2016-096175
- Grimaldi DA. Diagnosing gluteal tendinopathy in clinical practice. https://dralisongrimaldi.com/blog/diagnosing-gluteal-tendinopathy-in-clinical-practice/
- Mellor R, Bennell K, Grimaldi A, et al. Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: prospective, single blinded, randomised clinical trial. BMJ. 2018;361:k1662. doi:10.1136/bmj.k1662
- Plinsinga ML, Coombes BK, Mellor R, Vicenzino B. Individuals with Persistent Greater Trochanteric Pain Syndrome Exhibit Impaired Pain Modulation, as well as Poorer Physical and Psychological Health, Compared with Pain-Free Individuals: A Cross-Sectional Study. Pain Med. 2020;21(11):2964-2974. doi:10.1093/pm/pnaa047
- Grimaldi A, Ganderton C, Nasser A. Gluteal tendinopathy masterclass: Refuting the myths and engaging with the evidence. Musculoskelet Sci Pract. 2025;76:103253. doi:https://doi.org/10.1016/j.msksp.2025.103253
- Selkowitz DM, Beneck GJ, Powers CM. Which exercises target the gluteal muscles while minimizing activation of the tensor fascia lata? Electromyographic assessment using fine-wire electrodes. J Orthop Sports Phys Ther. 2013;43(2):54-64. doi:10.2519/jospt.2013.4116
- Dean BJF, Lostis E, Oakley T, Rombach I, Morrey ME, Carr AJ. The risks and benefits of glucocorticoid treatment for tendinopathy: A systematic review of the effects of local glucocorticoid on tendon. Semin Arthritis Rheum. 2014;43(4):570-576.
- Baskerville R, McCartney DE, McCartney SM, Dawes H, Tan GD. Tendinopathy in type 2 diabetes: a condition between specialties? Br J Gen Pract. 2018;68(677):593-594. doi:10.3399/bjgp18X700169
- Chandrasekaran S, Gui C, Hutchinson MR, Lodhia P, Suarez-Ahedo C, Domb BG. Outcomes of Endoscopic Gluteus Medius Repair: Study of Thirty-four Patients with Minimum Two-Year Follow-up. J Bone Joint Surg Am. 2015;97(16):1340-7. doi:10.2106/jbjs.N.01229