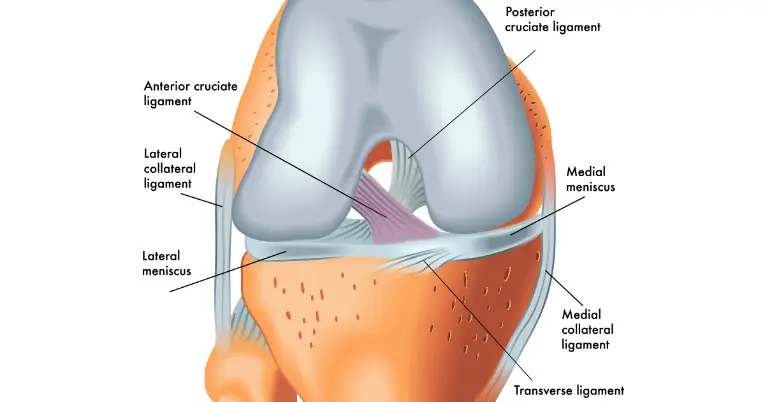
The anterior cruciate ligament (ACL) is a key stabilising ligament within the knee joint, connecting the femur (thigh bone) to the tibia (shin bone) (see Figure 1). Its primary role is to resist both forward movement of the tibia and limit excessive rotational forces acting on the knee, particularly during dynamic movements such as cutting, pivoting, and landing. As such, it plays a crucial role in maintaining knee stability during sport and high-level physical activity.
ACL injuries most commonly occur through non-contact mechanisms involving rapid deceleration, cutting, pivoting, or landing movements (which are particularly common in field-based sports). During these actions, injury typically occurs when the knee collapses into valgus (inward movement), combined with internal rotation of the femur relative to the tibia (see Figure 2). This often happens with the knee in a relatively extended (less flexed) position, which reduces the capacity of the surrounding musculature to absorb load, increasing strain on the ACL. Contact mechanisms, such as a direct blow to the knee resulting in valgus stress or hyperextension, are less common causes of ACL injury but can occur nonetheless.1
In Australia, an increase in sports participation across all levels has led to a rising incidence of ACL injuries. Between 1998 and 2018, ACL injuries increased by 5.2% per year in males and 6.2% per year in females.2
While the ACL is a relatively small structure, the consequences of an ACL injury are far from minor. The prolonged recovery period, increased risk of re-injury,3 and heightened likelihood of developing long-term knee pathology mean ACL injuries can have a significant impact on an individual’s physical, financial, and psychological wellbeing.4
While conservative rehabilitation is an emerging and evolving area, the majority of ACL injuries in populations with aspirations to return to sport are managed with surgical reconstruction, with the goal of restoring knee stability and enabling an appropriate return to sport.
Several graft options are commonly used, including the hamstring tendon (HT), bone–patellar tendon–bone (BPTB), and quadriceps tendon (QT). The choice of graft is typically individualised, based on factors such as patient goals, sport demands, and surgeon preference.
Ongoing Issues Following ACL Surgery
Graft re-rupture/failure remains a key concern following ACL reconstruction, particularly in younger and more active populations returning to high-level sport. Re-injury rates have been reported to range between 5 and 25% and higher rates, and again are more commonly observed in individuals under 25 years returning to pivoting sports in which the mechanism of injury is more prevalent (as shown in Figure 2).5,6

Continued knee instability also remains a challenging issue for many individuals following ACL injury and reconstruction. This most commonly involves tibial anterolateral rotary instability, which characterised by excessive forward movement of the tibia combined with increased opening of the knee joint on the outer (lateral) side.7 This can lead to persistent feelings of instability and may stop high level athletes from resuming their previous level of sports performance. Instability has been shown to increase the risk of ACL graft failure (re-injury).8
What is a Lateral Extra Articular Procedure? What are the different types?
A Lateral Extra-Articular Procedure (LEAP) is an additional surgical technique performed alongside an ACL reconstruction to improve rotational stability of the knee. By reinforcing the lateral structures, LEAPs help to reduce residual laxity and offload stress on the ACL graft, thereby lowering the risk of graft rupture. Essentially, it makes the knee more robust during twisting, cutting, and pivoting movements (where ACL injuries most commonly occur).
It is important to affirm that a LEAP is an ADDITIONAL procedure to ACL reconstruction, NOT a replacement.
LEAPs are done via lateral extra-articular tenodesis (LET) or anterolateral ligament reconstruction (ALL-R) techniques. Choice of specific procedure is driven largely by surgeon preference and experience.
Lateral Extra-Articular Tenodesis (LET)
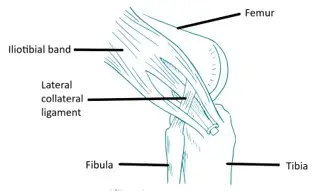
While several techniques exist, a LET most commonly involves re-routing a strip of the iliotibial band (ITB) under the lateral collateral ligament (LCL). The ITB is a thick band of connective tissue that runs from the pelvis (iliac crest) down to the outer part of the tibia, and plays an important role in stabilising the hip and knee during activities such as walking and running.
During a LET, a portion of the ITB is partially detached, passed underneath the LCL, and then commonly fixed back onto the tibia. This creates an additional restraint on the outside of the knee, helping to limit excessive internal rotation of the tibia and improve overall knee stability (see Figure 3).9
Importantly, a LET is a relatively quick addition to surgery, typically adding only 10–15 minutes to the overall procedure.10
Anterolateral Ligament Reconstruction (ALL-R) Techniques
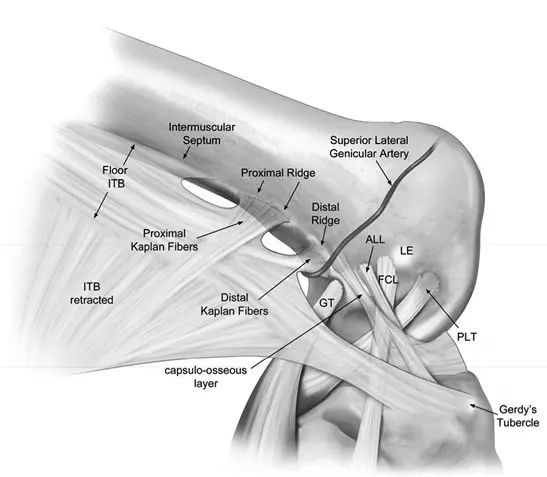
ALL-Rs aims to restore the function of the anterolateral ligament (ALL), an anatomical or ‘native’ structure on the outer side of the knee that contributes to rotational stability.
After many ACL injuries, the ALL may also be compromised, or may not provide sufficient resistance to rotational forces during high-demand activities. ALL-Rs addresses this by recreating the ligament using a tendon graft.
A tendon (most commonly from the hamstrings or adductor complex) is harvested and fixed between the femur and tibia at the anatomical attachment points of the native ALL.9 This helps restore rotational control of the knee and acts as a secondary stabiliser alongside the ACL graft.
Do LEAPs work? What’s the evidence?
A systematic review and meta-analysis was recently published by Kan et al.11 in 2025, performed at the Bond Institute of Health and Sport, Bond University, Robina, Australia (less than 10 minutes from POGO Physio). Systematic reviews and meta-analyses represent the highest level of evidence in the hierarchy of research, as they synthesise findings from multiple individual studies to provide a comprehensive/balanced overview of the available literature. By pooling data across studies, meta-analyses improve precision of effect estimates, reduce the effect of bias, and help identify consistent patterns or discrepancies that may not be clear in single studies alone.
In this thorough review by Kan et al.,11 15 randomised controlled trials investigating the effects of LEAPs in conjunction with ACL reconstructions were studied. 10 were used for pooled meta-analysis.
A total of 1,549 individuals (mean age 26.6 years; 66% male) were therefore analysed. All studies reviewed patients for at least 12 months following their procedure. In 6 studies, an ALL-R was used. In 9 studies, LETs were performed.
The study found that LEAPs performed in ACL reconstructions significantly reduced rotatory stability 12 months post-operation (as measured by orthopaedic special tests such as the pivot shift test, which reflect ongoing anterolateral rotary instability that can increase strain on the ACL graft). No significant difference was observed at 24 months amongst included studies, which may be explained by rehabilitation-related improvements in neuromuscular control and/or the fact ACL grafts are generally fully incorporated by this time.12
Included studies also noted a reduction in graft re-ruptures. Adding a LEAP to ACL reconstructions led to a 79% reduced graft rupture risk at 12 months, and 68% at 24 months.
Interestingly, functional measures (e.g., questionnaires assessing subjects self-reported knee symptoms, function, and sports activity) demonstrated no significant difference between those who did have a LEAP with their ACL reconstruction compared to those who did not. This suggests that while LEAPs improve mechanical stability (as observed clinically) and reduce graft rupture risk, they may not always translate into noticeably superior self-perceived function (across these time-frames).
Short-Term Trade-Offs of the LEAPs
While LEAPs clearly offer benefits in reducing rotatory instability and graft rupture risk, they are associated with greater early postoperative trade-offs (i.e., unwanted symptoms).
Pain
Those who undergo ACL reconstructions with an additional LEAP commonly report increased pain in the first 3-6 months post-op. This is thought to be caused by the additional surgical techniques/incisions required for the LEAP.13 However, Kan et al.11 found short-term elevated pain levels after LEAPs were not detected at 6 months onward within their observed studies. Another study by Marshall et al. (2022)13 reported that pain caused by the addition of LEAPs completely resolved for 98.3% of patients within 12 months post-op.
Range of motion and muscle weakness
In one study, short-term reductions in knee range of motion (extension and flexion) have been observed, alongside increased perceived joint stiffness.13 These deficits may be influenced by postoperative swelling, inflammation, and a slightly higher risk of arthrofibrosis due to the added procedure.11
Similarly, additional early reductions in quadriceps strength and functional performance (e.g., hop tests) are commonly noted,11 and may be explained by muscle inhibition caused by pain and consequent higher muscle wastage.
While Kan et al.11 only noted these effects to be present within the first 6 months post-op, stiffness and additional weakness have the potential to slow progression through rehabilitation phases.
Worth it?
By 6–12 months post-operatively, differences in pain, strength, range of motion, and patient-reported function between those undergoing ACLR with and without a LEAP are no longer evident.11 This suggests that, although the early rehabilitation period may be more challenging, the addition of a LEAP does not negatively impact medium-term recovery or overall functional outcomes. Given the reductions in rotatory instability and graft rupture risk, it can be argued that the risk of short-term increases in pain and reduction in strength and mobility are reasonably acceptable, depending on the individual (more on this consideration below).
Long-Term Trade-Offs of LEAPs
It should be stated that there are concerns around LEAPs relating to an increased risk of degenerative changes and osteoarthritic progression in the long term with the procedure. This is hypothesised to be a potential consequence of overstraining the lateral (outside) aspect of the knee, with the increased tibiofemoral contact pressure after LEAPs potentially accelerating lateral tibiofemoral cartilage wear over time.14,15,16 The current evidence investigating this relationship is limited and somewhat conflicting. One study has reported an increased prevalence of lateral compartment osteoarthritis following LEAPs,15 though numerous others have not via radiographic,11,17,18 and kinematic study methods.11,19,20
To better understand the balance between improved mechanical stability and potential degenerative risk (and therefore draw a definitive conclusion), further high-quality, long-term studies are required.11
The uncertainty of long-term effects reinforces the importance of careful patient selection. Accordingly, LEAPs are most appropriately considered in individuals at higher risk of graft failure (e.g., young, high-level athletes participating in pivoting sports), where the benefits may outweigh the potential long-term risks.
Who Should and Who Shouldn’t Receive a LEAP?
Despite all the benefits of reducing rotatory instability and graft rupture risk, LEAPs should not be viewed as necessary for all individuals.
Rather, LEAPs are increasingly viewed as most appropriate for selected individuals at higher risk of graft failure or persistent rotational instability.11 This includes younger, highly active athletes, particularly if they intend to return to cutting, pivoting, or field-based sports, such as soccer, rugby, AFL, basketball, and netball where rotational strain placed on the graft is higher. It may also be particularly relevant for individuals with a higher grades of anterolateral rotatory instability (as determine with orthopaedic special tests described above), generalised ligamentous laxity, knee hyperextension, or other factors that increase rotational load through the ACL graft.11
LEAPs may be less appropriate in ‘lower-risk patients’, such as those with lower sporting demands (i.e., those not aiming to return to high-risk pivoting sport), or good baseline rotational control. Given the short-term ‘trade-offs’, it should also be considered carefully in patients with high pre-operative pain sensitivity, significant early stiffness risk, or concerns around postoperative morbidity, because LEAPs may increase early pain, stiffness, and quadriceps inhibition. Additionally, it could be argued extra caution is warranted in patients with existing lateral compartment pathology or established tibiofemoral osteoarthritis, given the unresolved concern that some extra-articular procedures may increase lateral compartment loading. While current evidence does not confirm a clear osteoarthritis risk, long-term data remains limited.
Further Information and Resources
For more information on ACL injuries and considerations around surgery and return to sport, please refer to following resources below.
- Listen to Mick Hughes’ (expert physiotherapist in all things relating to ACL) conversation with Brad Beer on The Physical Performance Show (Episode #149), where the two discuss ACL rehabilitation, certain groups of individuals that are more at risk of an ACL injury, and general rehabilitation principles. You can listen to the episode on Spotify.
- Return to Running after ACL Surgery
- ACL Injuries – Surgical Vs Non-Surgical
- ACL Surgery: Return to Sport Testing
References
- Boden BP, Dean GS, Feagin JA, Jr., Garrett WE, Jr. Mechanisms of anterior cruciate ligament injury. Orthopedics. Jun 2000;23(6):573-8. doi:10.3928/0147-7447-20000601-15
- Maniar N, Verhagen E, Bryant AL, Opar DA. Trends in Australian knee injury rates: An epidemiological analysis of 228,344 knee injuries over 20 years. Lancet Reg Health West Pac. Apr 2022;21:100409. doi:10.1016/j.lanwpc.2022.100409
- Rodriguez-Merchan EC, Valentino LA. Return to Sport Activities and Risk of Reinjury Following Primary Anterior Cruciate Ligament Reconstruction. Arch Bone Jt Surg. Aug 2022;10(8):648-660. doi:10.22038/abjs.2021.50463.2504
- Øiestad BE, Engebretsen L, Storheim K, Risberg MA. Knee osteoarthritis after anterior cruciate ligament injury: a systematic review. Am J Sports Med. Jul 2009;37(7):1434-43. doi:10.1177/0363546509338827
- Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD. Risk of Secondary Injury in Younger Athletes After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis. Am J Sports Med. Jul 2016;44(7):1861-76. doi:10.1177/0363546515621554
- Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of Second ACL Injuries 2 Years After Primary ACL Reconstruction and Return to Sport. Am J Sports Med. Jul 2014;42(7):1567-73. doi:10.1177/0363546514530088
- Grassi A, Zicaro JP, Costa-Paz M, et al. Good mid-term outcomes and low rates of residual rotatory laxity, complications and failures after revision anterior cruciate ligament reconstruction (ACL) and lateral extra-articular tenodesis (LET). Knee Surg Sports Traumatol Arthrosc. Feb 2020;28(2):418-431. doi:10.1007/s00167-019-05625-w
- Group AS. ALL, ALC, and LET: What is it All About? https://aclstudygroup.org/Resources/ALL-ACL-LET
- Noailles T, Toanen C, Geffroy L, Lopes R, Hardy A. Anterior Cruciate Ligament and Anterolateral Ligament Reconstruction With Pedicular Hamstrings Tendon Graft, Single-Strand Gracilis for ALL and Single Blind Femoral Tunnel. Arthroscopy Techniques. 2023/07/01/ 2023;12(7):e1145-e1154. doi:https://doi.org/10.1016/j.eats.2023.03.003
- Goldberg DM. Lateral extra-articular tenodesis. Orthosports. https://orthosports.com.au/lateral_extra-articular_tenodesis
- Kan A, English T, Penny A, Franc-Smith J, Tudor F, Sattler L. Does the Addition of a Lateral Extra-articular Procedure to a Primary Anterior Cruciate Ligament Reconstruction Result in Superior Functional and Clinical Outcomes? A Systematic Review and Meta-analysis of Randomized Controlled Trials. The American Journal of Sports Medicine. 2025;53(11):2749-2760. doi:10.1177/03635465241304781
- Runer A, Keeling L, Wagala N, et al. Current trends in graft choice for anterior cruciate ligament reconstruction – part I: anatomy, biomechanics, graft incorporation and fixation. J Exp Orthop. Apr 1 2023;10(1):37. doi:10.1186/s40634-023-00600-4
- Heard M, Marmura H, Bryant D, et al. No increase in adverse events with lateral extra-articular tenodesis augmentation of anterior cruciate ligament reconstruction – Results from the stability randomized trial. J isakos. Aug 2023;8(4):246-254. doi:10.1016/j.jisako.2022.12.001
- Marshall DC, Silva FD, Goldenberg BT, Quintero D, Baraga MG, Jose J. Imaging Findings of Complications After Lateral Extra-Articular Tenodesis of the Knee: A Current Concepts Review. Orthop J Sports Med. Aug 2022;10(8):23259671221114820. doi:10.1177/23259671221114820
- Castoldi M, Magnussen RA, Gunst S, et al. A Randomized Controlled Trial of Bone-Patellar Tendon-Bone Anterior Cruciate Ligament Reconstruction With and Without Lateral Extra-articular Tenodesis: 19-Year Clinical and Radiological Follow-up. Am J Sports Med. Jun 2020;48(7):1665-1672. doi:10.1177/0363546520914936
- Neri T, Cadman J, Beach A, et al. Lateral tenodesis procedures increase lateral compartment pressures more than anterolateral ligament reconstruction, when performed in combination with ACL reconstruction: a pilot biomechanical study. J isakos. Mar 2021;6(2):66-73. doi:10.1136/jisakos-2019-000368
- Devitt BM, Bouguennec N, Barfod KW, Porter T, Webster KE, Feller JA. Combined anterior cruciate ligament reconstruction and lateral extra-articular tenodesis does not result in an increased rate of osteoarthritis: a systematic review and best evidence synthesis. Knee Surg Sports Traumatol Arthrosc. Apr 2017;25(4):1149-1160. doi:10.1007/s00167-017-4510-1
- Zaffagnini S, Marcheggiani Muccioli GM, Grassi A, et al. Over-the-top ACL Reconstruction Plus Extra-articular Lateral Tenodesis With Hamstring Tendon Grafts: Prospective Evaluation With 20-Year Minimum Follow-up. Am J Sports Med. Dec 2017;45(14):3233-3242. doi:10.1177/0363546517723013
- Jacob G, Lim YP, Brito CA, Parker DA. Lateral extra-articular tenodesis does not enhance ACL graft healing, however, does reduce graft tunnel widening. Knee Surgery, Sports Traumatology, Arthroscopy. 2024/11/01 2024;32(11):2885-2894. doi:https://doi.org/10.1002/ksa.12310
- Williams A, Ball S, Stephen J, White N, Jones M, Amis A. The scientific rationale for lateral tenodesis augmentation of intra-articular ACL reconstruction using a modified ‘Lemaire’ procedure. Knee Surg Sports Traumatol Arthrosc. Apr 2017;25(4):1339-1344. doi:10.1007/s00167-017-4537-3